Arq. Bras. Oftalmol. 2026;89 (2 )
:1-9
| DOI: 10.5935/0004-2749.2025-0113
Abstract
PURPOSE: This study aimed to identify the strategies adopted by Brazilian ophthalmologists to control myopia in clinical practice.
METHODS: This was a prospective cross-sectional study. Data were collected using an online questionnaire.
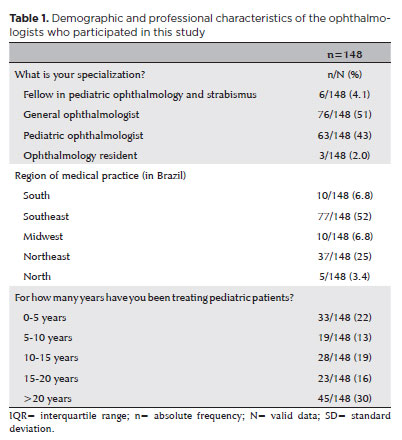
RESULTS: Responses from 148 participants were collected between March and May 2024. The majority of respondents were general ophthalmologists (51%) and pediatric ophthalmologists (43%). They came from all regions of Brazil, but more than half (52%) were from the Southeast region. Most participants (30%) had over 20 years of clinical practice experience. A significant proportion (89.2%) treated progressive myopia. The most requested complementary exams were optical biometry (83.78%) and corneal topography or tomography (69.59%). Behavioral measures were considered the most effective myopia treatment strategies by 41.2% of the respondents, followed by optical (33.8%) and pharmacological interventions (25%). Most recommended spending more time outdoors (94.59%) and reducing screen time (93.92%). Spectacle lenses for myopia (83.11%) and 0.025% atropine eye drops (54.73%) were the most prescribed treatments after the recommendation of environmental and behavioral changes.
CONCLUSION: This study presents a novel analysis of the clinical strategies for myopia control among Brazilian ophthalmologists. Understanding current clinical practices and identifying possible improvements are essential steps toward developing evidence-based guidelines and professional education aimed at improving patient care.
Keywords: Myopia/epidemiology; Refractive errors; Contact lenses; Myopia/drug therapy; Atropine/therapeutic use; Ophthalmologists; Practice patterns, physicians’; Surveys and questionnaires; Brazil/epidemiology
Arq. Bras. Oftalmol. 2021;84 (6 )
:561-568
| DOI: 10.5935/0004-2749.20210093
Abstract
Objetivo: Fornecer orientações sobre a frequência e os componentes dos exames oftalmológicos para crianças saudáveis de 0 a 5 anos.
Métodos: Essas diretrizes foram desenvolvidas com base em revisão bibliográfica e experiência clínica de um comitê de especialistas. Foram realizadas buscas PubMed/Medline; documentos selecionados não se restringiram a revisões sistemáticas, ensaios clínicos randomizados e estudos observacionais. Quando adequado, o perfil GRADE foi aplicado para graduá-los e o consenso de especialistas foi usado nos tópicos sem evidência científica. Também foram revisadas as recomendações pela Academia Americana de Pediatria, Associação Americana de Oftalmologia Pediátrica e Estrabismo, Academia Americana de Oftalmologia, Royal College of Ophthalmologist e Sociedade Canadense de Oftalmologia. O documento final foi aprovado pela Sociedade Brasileira de Oftalmologia Pediátrica e Sociedade Brasileira de Pediatria.
Resultados: Os recém-nascidos devem ser submetidos ao teste do reflexo vermelho e inspeção dos olhos e anexos pelo pediatra dentro de 72 horas de vida ou antes da alta da maternidade. O teste do reflexo vermelho deve ser repetido pelo pediatra durante as consultas de puericultura pelo menos três vezes ao ano durante os primeiros 3 anos de vida. Se factível, um exame oftalmológico completo pode ser feito entre 6 a 12 meses de vida. Até os 36 meses de idade, os marcos visuais, função visual apropriada para a idade, fixação e alinhamento ocular também devem ser avaliados pelo pediatra ou médico da família. Pelo menos um exame oftalmológico completo deve ser realizados entre 3 e 5 anos de idade. O exame deve conter pelo menos inspeção dos olhos e anexos, avaliação da função visual apropriada para a idade, avaliação da motilidade e alinhamento ocular (testes de cobertura), refração sob cicloplegia e avaliação do fundo de olho dilatado.
Conclusões: As diretrizes sobre a frequência da avaliação oftalmológica são ferramentas importantes para orientar os médicos sobre a melhor prática a fim de evitar problemas visuais tratáveis na infância, que poderiam comprometer seu desenvolvimento social, escolar e global, além de causar perda permanente da visão.
Keywords: Técnicas de diagnóstico oftalmológico, Triagem visual; Testes visuais; Criança, Lactente
Arq. Bras. Oftalmol. 2026;89 (1 )
:1-6
| DOI: 10.5935/0004-2749.2025-0049
Abstract
PURPOSE: This cross-sectional study compared best-corrected visual acuity obtained using Cloudscaper symbols, a novel optotype developed according to ETDRS specifications for children's virtual screening, with that obtained using LEA symbols.
METHODS: A total of 560 children aged 3-16 yr underwent visual acuity test with both Cloudscaper symbols and LS. The test application was standardized using the EyeSpy algorithm. Additionally, 147 participants were tested with the standard Snellen E paper chart. Paired t tests were performed to assess the clinical significance of logMAR visual acuity differences.
RESULTS: The mean logMAR visual acuity with LEA symbols was 0.12 (standard deviation [SD]=0.18; range, -0.10 to 0.80), while with Cloudscaper symbols it was 0.18 (SD=0.19; range, -0.10 to 0.80). The mean difference between Cloudscaper symbols and LEA symbols was 0.099 logMAR (approximately 0.5 optotypes; SD=0.08; range, 0.0-0.14; p<0.0001). Cloudscaper symbols slightly underestimated visual acuity compared to LEA symbols. Visual acuity measured by both methods was highly correlated (Spearman's r=0.74, p<0.0001). The mean visual acuity difference between Cloudscaper symbols and the Snellen E chart was 0.0045 (p=0.805; 95% confidence interval [95% CI]), whereas the difference between LEA symbols and Snellen E was 0.0883 (p<0.001; 95% CI).
CONCLUSIONS: Cloudscaper symbols provide a reliable tool for visual screening in children. Although they slightly underestimate visual acuity compared to LEA symbols – a finding also reported when comparing ETDRS letters with LEA symbols – Cloudscaper symbols show strong agreement with Snellen E chart measurements. This suggests that Cloudscaper symbols allow precise visual acuity assessment comparable to the gold standard.
Keywords: Vision screening; Vision tests; Visual acuity; Mobile applications; Eye health; Child health; Diagnostic techniques, Ophthalmological; Child; Preschool child; Adolescent
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.

06-tab01tb.jpg)

10-fig01.jpg)
10-tab01tb.jpg)
04-tab01.jpg)