Arq. Bras. Oftalmol. 2017; 80 (6): 10.5935/0004-2749.20170095
Total: 1481
Julia Dutra Rossetto1,2; Eduardo Novais2; Hilda Capó1
DOI: 10.5935/0004-2749.20170095
ABSTRACT
Herein, we describe the case of a 4-year-old child with indirect traumatic optic neuropathy and serial changes of the optic nerve head and retinal nerve fiber layer (RNFL) documented using optical coherence tomography (OCT). Visual acuity improved despite progressive RNFL thinning and optic disc pallor. We concluded that OCT may be useful for monitoring axonal loss but may not predict the final visual outcome.
Keywords: Optic nerve injuries; Retina; Retinal neurons; Tomography, optical coherence; Humans; Case report
RESUMO
Descrição do caso de uma criança de 4 anos de idade com neuropatia óptica traumática indireta, cujas alterações no nervo óptico e na camada de fibras nervosas da retina foram documentadas com tomografia de coerência óptica seriadas. A acuidade visual apresentou melhora apesar da diminuição progressiva da camada de fibras nervosas e da palidez do disco óptico. Em conclusão, a tomografia de coerência óptica pode ser útil para monitorar a perda axonal na neuropatia óptica traumática indireta, sem no entanto, predizer o desfecho visual.
Descritores: Traumatismos do nervo óptico; Retina; Neurônios retinianos; Tomografia de coerência óptica; Humanos; Relato de casos
INTRODUCTION
The incidence of traumatic optic neuropathy (TON) varies from 0.5% to 5% after head trauma in adults(1,2). Indirect TON is caused by the transmission of forces to the optic nerve from a distant site without disruption of normal tissue structures after head trauma, and the optic canal is the most common location associated with this type of injury(3). Because the optic disc usually appears normal, it can be difficult to detect indirect TON by ophthalmoscopy and standard imaging techniques(3). The diagnosis of TON is presumed by the history of trauma associated with pupillary defect and a decrease in visual acuity (VA) at the time of injury or, in some cases, several days after the trauma(3). The treatment of TON is controversial and includes observation, corticosteroids, and decompression of the canalicular portion of the optic nerve.
In children, the leading causes of TON are motor vehicle accidents, sports injuries, and falls from high elevations(1,4-6), with blunt trauma happening more frequently than penetrating trauma(1). The visual outcome has been reported as VA worse than 20/80 in 72% of affected children and adolescents(3). Herein, we describe the first report of serial optical coherence tomography (OCT) findings and their correlation with VA in a child with TON.
CASE REPORT
A 4-year-old boy presented to an emergency room a few hours after falling overboard during a boating accident from a height of approximately 3 feet. He suffered no loss of consciousness and had an unquantified visual loss in the left eye and a small cut on the left brow, with no penetrating injury to the left orbit. A non-contrast computed tomography of the head and orbits was performed, demonstrating a non-depressed fracture of the left sphenoid wing and lamina papyracea, with normal orbital contents and no involvement of the left optic canal, hemorrhage, or proptosis. TON was diagnosed, and intravenous corticosteroids were administered for 3 days. The patient had unremarkable past medical and ocular histories, as well as unremarkable family history. He had no history of previous use of relevant medications.
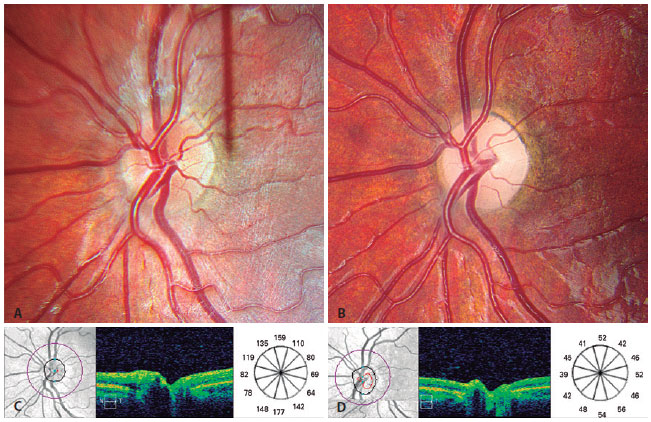
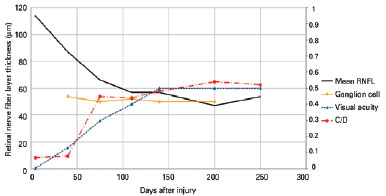
Five days after the trauma, the patient presented to our institution on oral corticosteroids. His best corrected VA was 20/30 OD and 16/400 OS. A left relative afferent pupillary defect was noted. Slit-lamp and ocular motility examinations were normal. The intraocular pressure was 14 mmHg and 12 mmHg in the right and left eyes, respectively. Funduscopic examination revealed no swelling or pallor of the optic nerve heads (ONHs), with a cup-to-disc ratio of 0.1 (Figure 1) and a normal retina in both eyes. The mean peripapillary retinal nerve fiber layer (RNFL) thickness measurement by spectral-domain Cirrus high-definition OCT (Carl Zeiss Meditec Inc., Dublin, CA, USA) was 113 µm OD and 114 µm OS. Although treatment has not been proven to improve visual outcome(1), the family elected to complete a 1-week course of oral steroids. Serial examinations evaluating VA and OCT measurements of the RNFL and ganglion cell (GC) layer thickness were performed at all visits (days 5, 40, 75, 110, 140, 200, and 250) after the injury (Figure 2), except for the GC values on day 5, which could not be obtained because of a lack of cooperation. A diffuse gradual thinning of the RNFL and GC layer and an increase of the cup-to-disc ratio was demonstrated by serial OCT scans, demonstrating stability 75 days after the injury. Optic disc pallor was documented photographically (Figure 1B). Despite retinal and ONH alterations, VA by single HOTV progressively improved until 140 days after the injury (16/400, 20/150, 20/60, 20/50, and 20/40 at days 5, 40, 75, 110, and 140, respectively), and was maintained until the last follow-up (Figure 2).
DISCUSSION
There are few reports on progressive RNFL and GC loss after acute indirect TON in children. Medeiros et al.(7) reported an initial loss of axons after TON in the first month following injury using scanning laser polarimetry, with a subsequent severe decrease in RNFL thickness measurements in a 19-year-old man at 90 days. Another case report showed reductions in RNFL thickness within 20 days of the injury and further loss of nerve fibers with severe thinning of the RNFL at 70 days after the injury, with no visual improvement despite steroid treatment in a 14-year-old boy(8). Miyahara et al. reported an early increase in the RNFL thickness in TON, followed by an increase in the cup-to-disc ratio and progressive loss of the RNFL that was complete by day 90 following the injury(3). Shi et al. studied axonal loss and blood flow disturbance in a cohort of 54 patients with TON, and found a decrease in RNFL thickness after 2 weeks in the better than 'no light perception' (NLP) group. In contrast, in the NLP group, the RNFL thickness slightly increased for 2 weeks following injury, then dramatically reduced after 4 weeks(9).
In our patient, progressive RNFL loss was more pronounced within the first 75 days, and became fairly stable after this period. Although we were unable to obtain an initial value for the GC layer thickness as a result of poor cooperation, it appears that there was an early decrease by day 40 when compared to the fellow eye (average GC layer thickness on day 40: OD= 87 µm, OS= 54 µm), remaining stable thereafter. The increase in the cup-to-disc ratio as assessed by OCT started after day 40, and leveled by day 200. The mean RNFL thickness in our patient was similar to the values reported in a study of three adults with TON (114 µm in the first week and 46 µm in the 20th week), although the authors reported evident GC loss only at 12 weeks after the trauma(10).
In contrast with the aforementioned reports, in our patient, VA progressively improved during the follow-up period, stabilizing at 20/40 after the visit on day 140. Although single optotypes may overestimate VA, the single HOTV was the most sophisticated test that this 4-year-old could perform. This degree of visual improvement may not be typical; however, a visual outcome of ≥20/80 has been reported in 28% of children with TON(1). The reported visual improvement may be associated with childhood neuronal plasticity.
To our knowledge, this is the first report that correlates VA and serial OCT findings in TON in a young child, and documents improved VA despite progressive axonal loss.
The limitations of this study include the difficulty of assessing VA in a 4-year-old, especially with more refined visual tests, and the difficulty of OCT image acquisition, especially in the days immediately following the trauma.
In conclusion, our report illustrates the visual and OCT evolution of a child after severe head trauma, with remarkable visual improvement. In such cases, the family presents with a great deal of anxiety given the possibility of poor visual prognosis. We present data that suggest a minimum follow-up of 6 months for children after TON and the possibility of visual improvement during this period.
REFERENCES
1. Goldenberg-Cohen N, Miller NR, Repka MX. Traumatic optic neuropathy in children and adolescents. J AAPOS. 2004;8(1):20-7.
2. Steinsapir KD, Goldberg RA. Traumatic optic neuropathy. Surv Ophthalmol. 1994;38(6): 487-518.
3. Miyahara T, Kurimoto Y, Kurokawa T, Kuroda T, Yoshimura N. Alterations in retinal nerve fiber layer thickness following indirect traumatic optic neuropathy detected by nerve fiber analyzer, GDx-N. Am J Ophthalmol. 2003;136(2):361-4.
4. Shokunbi T, Agbeja A. Ocular complications of head injury in children. Childs Nerv Syst. 1991;7(3):147-9.
5. Ford RL, Lee V, Xing W, Bunce C. A 2-year prospective surveillance of pediatric traumatic optic neuropathy in the United Kingdom. J AAPOS. 2012;16(5):413-7.
6. Mahapatra A. Optic nerve injury in children. A prospective study of 35 patients. J Neurosurg Sci. 1992;36(2):79-84.
7. Medeiros FA, Susanna R Jr. Retinal nerve fiber layer loss after traumatic optic neuropathy detected by scanning laser polarimetry. Arch Ophthalmol. 2001;119(6):920-1.
8. Medeiros FA, Moura FC, Vessani RM, Susanna R Jr. Axonal loss after traumatic optic neuropathy documented by optical coherence tomography. Am J Ophthalmol. 2003; 135(3):406-8.
9. Shi W, Wang HZ, Song WX, Yang WL, Li WY, Wang NL. Axonal loss and blood flow disturbances in the natural course of indirect traumatic optic neuropathy. Chin Med J (Engl). 2013;126(7):1292-7.
10. Cunha LP, Costa-Cunha LV, Malta RF, Monteiro ML. Comparison between retinal nerve fiber layer and macular thickness measured with OCT detecting progressive axonal loss following traumatic optic neuropathy. Arq Bras Oftalmol. 2009;72(5):622-5.
Submitted for publication:
April 24, 2017.
Accepted for publication:
July 18, 2017.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.