Arq. Bras. Oftalmol. 2020;83 (5 )
:361-365
| DOI: 10.5935/0004-2749.20200044
Abstract
OBJETIVOS: Comparar as taxas de sucesso anatômico da vitrectomia e tamponamento de gás SF6 na cirurgia de buraco macular com e sem a postura pronada pós-operatória.
MÉTODOS: Foi realizado um estudo observacional, longitudinal e retrospectivo de séries de casos. O estudo incluiu 52 olhos de 52 pacientes submetidos à vitrectomia posterior via pars-plana com peeling de membrana limitante interna auxiliada por azul trypan e tamponamento com gás SF6 a 25% para os estágios 2, 3 e 4 dos buracos maculares. Após a cirurgia, todos os pacientes foram orientados a manter um regime postural pós-operatório: 31 pacientes foram orientados a não realizar posição pronada de cabeça, enquanto 21 foram orientados a manter uma pronada pós-operatória por 7 dias. O objetivo principal foi a análise da taxa de fechamento do buraco macular. A análise estatística foi realizada usando Epi-Info 7.1.
RESULTADOS: Um total de 47 (90,3%) pacientes obtiveram fechamento do buraco macular. O grupo de postura não pronada e o grupo de postura pronada obtiveram taxas de fechamento de 90,3%, e 90,4%, respectivamente; essas taxas não foram significativamente diferentes. A análise estatística revelou que não houve diferenças significativas relacionadas ao gênero, idade, duração do buraco macular, estágio do buraco macular, acuidade visual corrigida pré e pós-operatória entre os dois grupos.
CONCLUSÃO: Nossos resultados sugerem que a cirurgia para buraco macular com o uso de gás de curta duração (SF6) é segura e eficaz e que a manutenção de uma orientação pós-operatória de não-pronada também é segura. No entanto, essas recomendações devem ser avaliadas em um estudo prospectivo e randomizado para delinear de forma abrangente os riscos e benefícios associados.
Keywords: Perfurações retinianas; Vitrectomia; Cirurgia vitreorretiniana; Hexafluoreto de enxofre/administração & dosagem; Fluorocarbonetos/administração & dosagem; Decúbito dorsal; Cuidados pós-operatórios
Arq. Bras. Oftalmol. 2021;84 (3 )
:209-213
| DOI: 10.5935/0004-2749.20210035
Abstract
OBJETIVOS: Identificar vasos linfáticos em espécimes orbitários de cadáveres humanos através de microscopia óptica e análise imunohistoquímica.
MÉTODOS: Um estudo postmortem incluiu dez espécimes orbitários provenientes de dez cadáveres humanos. Todos os espécimes orbitários foram obtidos até 12 horas após a morte com uma técnica cirúrgica de exenteração orbitária e dissecados em glândula lacrimal, nervo óptico, gordura órbitária e músculos extraoculares. Para classificar como um vaso linfático, os critérios histológicos incluíram vasos endoteliais de parede única sem membrana basal bem desenvolvida, irregulares e lúmen sem hemácias, e os critérios imunohistoquímicos incluíram vasos endoteliais de parede única, com formato irregular e lúmen sem hemácias e reagentes a podoplanina D2-40.
RESULTADOS: As lâminas histológicas de glândula lacrimal, nervo óptico, tecido adiposo e músculos extraoculares reagiram positivamente a podoplanina D2-40.
CONCLUSÃO: Este estudo demonstrou vasos linfáticos na órbita humana, mais exatamente, na glândula lacrimal, no nervo óptico, na gordura orbitária e nos músculos extrínsecos extraoculares via microscopia óptica e imunohistoquímica.
Keywords: Vasos linfáticos; Órbita; Nervo óptico; Aparelho lacrimal; Músculos oculomotores; Tecido adiposo; Microscopia
Arq. Bras. Oftalmol. 2026;89 (1 )
:1-8
| DOI: 10.5935/0004-2749.2024-0397
Abstract
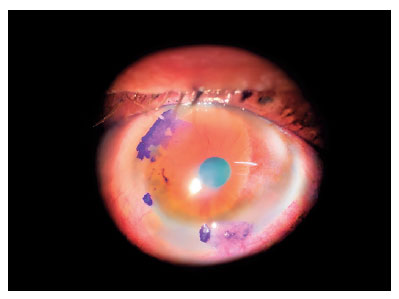
PURPOSE: Glaucoma is one of the leading causes of irreversible blindness worldwide. When topical hypotensive agents or laser trabeculoplasty fail to adequately control the disease, escalation of therapy becomes necessary, with transscleral cyclophotocoagulation being one of the available options. Several variations of transscleral cyclophotocoagulation exist, including traditional continuous wave, MicroPulse, and slow-coagulation techniques. We propose a novel variation – custom slow-coagulation transscleral cyclophotocoagulation – which combines elements of both continuous wave and slow-coagulation approaches. This study aimed to evaluate the outcomes of this technique in patients with refractory glaucoma.
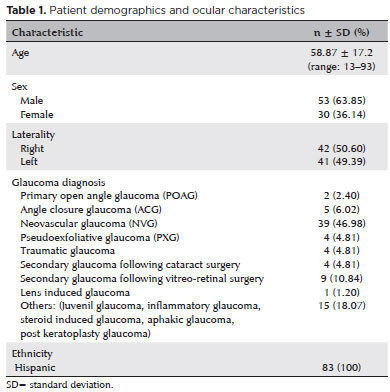
METHODS: This retrospective, interventional study included 104 eyes of 83 patients with refractory glaucoma who underwent custom slow-coagulation transscleral cyclophotocoagulation. Changes in intraocular pressure, visual acuity, the number of glaucoma medications, and postoperative complications were analyzed. A paired t test was used to compare changes in intraocular pressure and visual acuity, while the Wilcoxon signed-rank test was applied to categorical variables. Success rates following custom slow-coagulation transscleral cyclophotocoagulation were estimated using Kaplan–Meier survival analysis.
RESULTS: Mean intraocular pressure decreased significantly from 38.9 ± 15.8 mmHg at baseline to 16.3 ± 9.9 mmHg at Month 12 (p<0.001). The mean number of glaucoma medications also decreased significantly from 3.6 ± 0.6 to 1.8 ± 1.4 (p<0.001). No significant reduction in mean visual acuity was observed during follow-up.
CONCLUSIONS: Custom slow-coagulation transscleral cyclophotocoagulation effectively reduced baseline intraocular pressure and the number of glaucoma medications, with a low rate of complications and no decline in visual acuity over a 12-month follow-up period. This novel technique demonstrated a high safety profile in a Hispanic population and represents a low-cost, minimally invasive procedure with rapid recovery and promising efficacy in intraocular pressure control.
Keywords: Glaucoma/surgery; Sclera; Filtering surgery; Laser coagulation/methods; Lasers, semiconductor/therapeutic use; Intraocular pressure; Blindness/prevention & control; Vision, low/epidemiology; Visual acuity
Arq. Bras. Oftalmol. 2026;89 (4 )
:1-8
| DOI: 10.5935/0004-2749.2025-0313
Abstract
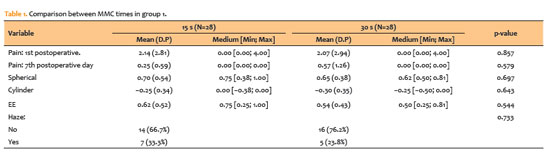
PURPOSE: To compare clinical outcomes associated with different intraoperative mitomycin C exposure times during photorefractive keratectomy for myopia and astigmatism correction.
METHODS: This prospective, comparative, contralateral-eye study included 41 patients (82 eyes), comprising 28 eyes with ablation <60µm and 13 eyes with ablation >60µm, who underwent photorefractive keratectomy with varying mitomycin C application times based on ablation depth. In eyes with ablation <60µm, mitomycin C was applied for 15 s in one eye and 30 s in the fellow eye. In eyes with ablation >60µm, mitomycin C was applied for 30 s in one eye and 60 s in the fellow eye. Outcomes included visual acuity, postoperative pain (visual analog scale), subjective tearing, corneal haze, and refractive results at 3 months.
RESULTS: No statistically significant differences were observed between mitomycin C application times within either group for postoperative pain, tearing, visual acuity, refractive outcomes (spherical, cylindrical, and spherical equivalent), or haze prevalence (p>0.05 for all comparisons). Visual acuity improved in all groups, and no eyes lost ≥2 lines of corrected distance visual acuity.
CONCLUSIONS: Shorter mitomycin C exposure times (15 or 30 s) appear to be as effective and safe as longer durations (30 or 60 s) for haze prevention after photorefractive keratectomy without compromising refractive outcomes or increasing postoperative discomfort at 3-month follow-up.
Keywords: Mitomicin/therapeutic use; Photorefractive keratectomy; Lasers, excimer; Intraoperative period; Miopia/surgery; Astigmatismo/surgery; Corneal opacity; Postoperative pain; Comparative study
Arq. Bras. Oftalmol. 2024;87 (6 )
:1-7
| DOI: 10.5935/0004-2749.2022-0252
Abstract
Objetivo: Determinar as taxas de fechamento de buracos maculares idiopáticos grandes tratados com vitrectomia posterior e técnica de flap invertido 360 graus pediculado de membrana limitante interna, sem posicionamento de cabeça pós-operatório e definir melhora visual, tipos de fechamento do buraco macular e integridade das camadas retinianas externas como objetivo secundário.
Métodos: Este estudo foi uma série retrospectiva de casos. Todos os pacientes foram submetidos a vitrectomia com flap invertido 360 graus pediculado de membrana limitante interna e tamponamento com gás, sem posição de cabeça no pós-operatório. Idade, gênero, tempo de redução da acuidade visual, outras patologias oculares e status do cristalino foram compilados. Medida de melhor acuidade visual corrigida e tomografia de coerência óptica foram registradas durante as visitas de pré e pós-operatório (15 dias e 2 meses após cirurgia).
Resultados: Vinte olhos de 19 pacientes foram incluídos neste estudo. A idade média foi de sessenta e seis anos. Um total de 19 olhos (95%) atingiu fechamento do buraco, observado através das imagens de tomografia de coerência óptica após 2 meses de cirurgia. Melhor acuidade visual corrigida média aumentou +1,08 pré-operatória para +0,66 LogMAR em 2 meses de cirurgia (p<0,001), com média de 20 letras de melhora visual (0,4 LogMAR) na tabela do Early Treatment Diabetic Retinopathy Study. Dois tipos de fechamento do buraco foram observados: V (47,36%) e U (52,63%).
Conclusão: A técnica de flap invertido 360 graus pediculado de membrana limitante interna, sem posicionamento de cabeça no pós-operatório promoveu elevada taxa de fechamento (95%), reestabelecimento das camadas retinianas externas, fechamento com contorno foveal dos tipos V e U, além de melhora visual na maioria dos casos de BMI grandes (mesmo nos buracos maiores que 650 μm). Esta técnica pode representar uma alternativa para o tratamento de buracos maculares grandes em pacientes impossibilitados de cumprir o tradicional posicionamento de cabeça pós-operatório.
Keywords: Perfurações retinianas; Cuidados pós-operatórios; Vitrectomia; Cirurgia vitreorretiniana
Arq. Bras. Oftalmol. 2026;89 (3 )
:1-8
| DOI: 10.5935/0004-2749.2025-0330
Abstract
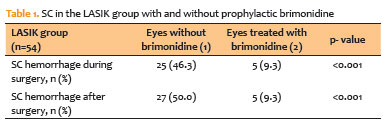
PURPOSE: To assess whether low-concentration brimonidine (0.025%) improves early postoperative signs and symptoms following femtosecond laser-assisted in situ keratomileusis and photorefractive keratectomy without affecting pupil diameter or flap safety.
METHODS: This prospective, randomized, double-masked, contralateral-eye, single-center study was conducted between January and September 2024. In each patient, one eye received 0.025% brimonidine 15–30 min before surgery (mean: 21.3 ± 2.4 min), whereas the fellow eye received 0.15% sodium hyaluronate (control). Primary outcomes on postoperative Day 1 included subconjunctival hemorrhage laser-assisted in situ keratomileusis and patient-reported symptoms (0–10 scale; composite score). Pupil diameter was measured pre-ablation. Statistical analyses included McNemar and paired t tests, with a significant threshold of α=0.05.
RESULTS: A total of 124 patients were included (54 laser-assisted in situ keratomileusis and 70 photorefractive keratectomy). Pupil diameter did not differ significantly between brimonidine-treated and control eyes (laser-assisted in situ keratomileusis: 2.63 ± 0.47 vs. 2.69 ± 0.42 mm, p=0.273; photorefractive keratectomy: 2.56 ± 0.44 vs. 2.61 ± 0.39 mm, p=0.116). In laser-assisted in situ keratomileusis, subconjunctival hemorrhage occurred less frequently in brimonidine-treated eyes both intraoperatively (9.3% vs. 46.3%, p<0.001) and on postoperative Day 1 (9.3% vs. 50.0%, p<0.001). Composite symptom scores were significantly lower in brimonidine-treated eyes in both laser-assisted in situ keratomileusis and photorefractive keratectomy groups (p=0.001 for both).
CONCLUSIONS: Preoperative administration of low-concentration brimonidine (0.025%) significantly reduced subconjunctival hemorrhage in laser-assisted in situ keratomileusis without comprising flap integrity. It also improved early postoperative symptoms in laser-assisted in situ keratomileusis and photorefractive keratectomy, without affecting pupil diameter. These findings support the use of dilute brimonidine as a safe and effective adjunct to enhance the immediate postoperative experience in refractive surgery.
Keywords: Brimonidine tartrate; Postoperative pain; Subconjunctival hemorrhage; Refractive surgery; Hemorrhage; Keratomileusis, laser in situ; Photorefractive keratectomy
Arq. Bras. Oftalmol. 2024;87 (3 )
:1-5
| DOI: 10.5935/0004-2749.2023-0033
Abstract
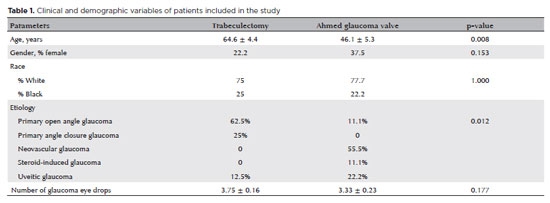
PURPOSE: This study aims to compare the initial ocular discomfort symptoms resulting from trabeculectomy and Ahmed glaucoma valve implantation surgeries.
METHODS: A prospective comparative study was conducted. The evaluation of ocular discomfort employed a questionnaire designed to identify the frequency and severity of distinct symptoms: ocular pain, general discomfort, tearing, foreign body sensation, and burning. This questionnaire was administered prior to surgery as a baseline, and subsequently at 7, 30, and 90 days post-surgery. Simultaneously, the Ocular Surface Disease Index (OSDI) was applied at these same time intervals.
RESULTS: The study encompassed a total of 17 patients (9 undergoing trabeculectomy and 8 undergoing Ahmed glaucoma valve implantation). The Ahmed glaucoma valve implantation group exhibited higher tearing levels at baseline (p=0.038). However, no statistically significant differences in symptoms were observed between the two surgeries at 7 and 30 days post-surgery. At the 90-day mark following surgery, patients who had undergone trabeculectomy reported a significantly higher foreign body sensation (p=0.004). Although OSDI scores did not differ between groups at baseline, the trabeculectomy group showed significantly higher OSDI scores than the Ahmed glaucoma valve implantation group at 7, 30, and 90 days after surgery (p<0.05).
CONCLUSION: Post-surgery, patients who had undergone trabeculectomy experienced increased foreign body sensation. Trabeculectomy appears to cause greater early postoperative ocular discomfort compared to the Ahmed glaucoma valve implantation group.
Keywords: Glaucoma/surgery; Paresthesia; Trabeculectomy; Glaucoma drainage implants; Postoperative care
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
01-tab01.jpg)
02-fig01.jpg)
04-fig01tb.jpg)
02-fig01.jpg)
12-fig01.jpg)
13-fig01tb.jpg)
02-fig01.jpg)
03-fig01.jpg)