Arq. Bras. Oftalmol. 2026; 89 (3): 10.5935/0004-2749.2025-0330
Total: 538
Natália Fernandes Gonçalves Napolitano1; Ana Vega Carreiro de Freitas1,2; Luís Gustavo de Imparato Rodrigues Ribeiro1; Daniella Villas Boas Fairbanks1; Fernando Antonio Galhardo Tarcha1,3; Vagner Loduca Lima1; Bernardo Kaplan Moscovici4,5; Edmundo José Velasco Martinelli1,3
DOI: 10.5935/0004-2749.2025-0330
ABSTRACT
PURPOSE: To assess whether low-concentration brimonidine (0.025%) improves early postoperative signs and symptoms following femtosecond laser-assisted in situ keratomileusis and photorefractive keratectomy without affecting pupil diameter or flap safety.
METHODS: This prospective, randomized, double-masked, contralateral-eye, single-center study was conducted between January and September 2024. In each patient, one eye received 0.025% brimonidine 15–30 min before surgery (mean: 21.3 ± 2.4 min), whereas the fellow eye received 0.15% sodium hyaluronate (control). Primary outcomes on postoperative Day 1 included subconjunctival hemorrhage laser-assisted in situ keratomileusis and patient-reported symptoms (0–10 scale; composite score). Pupil diameter was measured pre-ablation. Statistical analyses included McNemar and paired t tests, with a significant threshold of α=0.05.
RESULTS: A total of 124 patients were included (54 laser-assisted in situ keratomileusis and 70 photorefractive keratectomy). Pupil diameter did not differ significantly between brimonidine-treated and control eyes (laser-assisted in situ keratomileusis: 2.63 ± 0.47 vs. 2.69 ± 0.42 mm, p=0.273; photorefractive keratectomy: 2.56 ± 0.44 vs. 2.61 ± 0.39 mm, p=0.116). In laser-assisted in situ keratomileusis, subconjunctival hemorrhage occurred less frequently in brimonidine-treated eyes both intraoperatively (9.3% vs. 46.3%, p<0.001) and on postoperative Day 1 (9.3% vs. 50.0%, p<0.001). Composite symptom scores were significantly lower in brimonidine-treated eyes in both laser-assisted in situ keratomileusis and photorefractive keratectomy groups (p=0.001 for both).
CONCLUSIONS: Preoperative administration of low-concentration brimonidine (0.025%) significantly reduced subconjunctival hemorrhage in laser-assisted in situ keratomileusis without comprising flap integrity. It also improved early postoperative symptoms in laser-assisted in situ keratomileusis and photorefractive keratectomy, without affecting pupil diameter. These findings support the use of dilute brimonidine as a safe and effective adjunct to enhance the immediate postoperative experience in refractive surgery.
Keywords: Brimonidine tartrate; Postoperative pain; Subconjunctival hemorrhage; Refractive surgery; Hemorrhage; Keratomileusis, laser in situ; Photorefractive keratectomy
INTRODUCTION
Laser-assisted in situ keratomileusis (LASIK) and photorefractive keratectomy (PRK) are widely performed surgical procedures for the correction of refractive errors(1-3). Both techniques generally yield favorable visual outcomes and high levels of patient satisfaction. However, patients frequently experience transient discomfort and ocular surface disturbances during the early postoperative period(4).
Previous studies have demonstrated that preoperative instillation of brimonidine before excimer laser activation can improve postoperative comfort in LASIK and reduce conjunctival hyperemia and subconjunctival hemorrhage(5-7). In contrast, although PRK is commonly associated with more pronounced discomfort and conjunctival hyperemia due to epithelial removal, the effects of brimonidine in this setting have not been adequately investigated. Based on clinical observations, a single preoperative dose of diluted brimonidine (0.025%) administered 15-30 min before surgery may improve early postoperative comfort in both LASIK and PRK.
Postoperative findings such as conjunctival hyperemia, subconjunctival hemorrhage, and ocular discomfort are typically mild and self-limiting and do not compromise long-term refractive outcomes(8). Nevertheless, these symptoms may lead to patient anxiety, cosmetic dissatisfaction, and increased demand for unscheduled postoperative visits, thereby negatively affecting the overall patient experience(9-11). Therefore, minimizing these early postoperative effects may enhance patient satisfaction and reduce psychological and aesthetic concerns.
Brimonidine tartrate is a selective α2-adrenergic receptor agonist available in 0.1% and 0.2% ophthalmic formulations, primarily indicated for the treatment of glaucoma and ocular hypertension(12,13). In addition to its intraocular pressure-lowering effects, brimonidine exhibits vasoconstrictive properties(14-17), which may reduce proinflammatory mediator release and improve postoperative comfort(18,19).
In LASIK, preoperative use of 0.2% brimonidine has been shown to reduce conjunctival hyperemia, subconjunctival hemorrhage, and discomfort. However, concerns have been raised regarding potential interference with lamellar flap adherence and stability(5,6). More recent evidence suggests that lower concentrations (0.025%) preserve therapeutic benefits while minimizing adverse effects on corneal structure and wound healing(7,20-24).
In the United States, a 0.025% brimonidine tartrate ophthalmic solution is commercially available as Lumify (Bausch & Lomb Incorporated, Rochester, New York) and was approved by the Food and Drug Administration in 2018 as an ocular vasoconstrictor(20,21). Although this formulation is not commercially available in Brazil, it can be prepared by compounding pharmacies using brimonidine tartrate 0.025% with standard ophthalmic excipients.
Despite growing evidence supporting the use of low-concentration brimonidine in LASIK, its role in PRK remains insufficiently explored. Therefore, this study aimed to evaluate the effects of preoperative 0.025% brimonidine in both LASIK and PRK, focusing on its impact on subconjunctival hemorrhage and early postoperative symptoms, including pain, burning, stinging, irritation, itching, tearing, and foreign-body sensation.
METHODS
Study design and ethical aspects
This prospective, randomized, double-masked, contralateral-eye clinical study was conducted at a single refractive surgery center in Brazil, in accordance with the Declaration of Helsinki. The protocol was approved by the institutional ethics committees (CAAE: 81430024.5.3001.9867 and 81430024.5.1001.0082). Written informed consent was obtained from all participants.
Setting and participants
Consecutive adult patients scheduled for bilateral, same-day keratorefractive surgery (LASIK or PRK), with stable refraction (≥1 yr) and a healthy ocular surface, were eligible.
Exclusion criteria included prior ocular surgery, keratoconus or risk of ectasia, glaucoma or ocular hypertension, moderate-to-severe dry eye disease, pregnancy or lactation, known hypersensitivity to study medications, and systemic conditions that could impair wound healing. Patients with intraoperative complications were excluded.
Preoperative assessment
All patients underwent comprehensive ophthalmic evaluation, including dynamic and static refraction, slit-lamp biomicroscopy, Goldmann applanation tonometry, dilated fundus examination, and corneal tomography.
Tomography was performed using the Galilei Dual Scheimpflug Analyzer (Ziemer Ophthalmic Systems AG, Port, Switzerland) and/or Orbscan II (Bausch & Lomb/Orbtek Inc., Salt Lake City, Utah). Surgical indication and technique (LASIK or PRK) were determined by a faculty team.
Interventions
Fifteen to thirty minutes before excimer laser activation, one eye received a single drop of compounded brimonidine tartrate 0.025% (Neuvye Pharmacy, Curitiba, Brazil), and the fellow eye received 0.15% sodium hyaluronate (control).
The formulation contained brimonidine tartrate 0.025%, benzalkonium chloride, monobasic sodium phosphate, dibasic sodium phosphate, and water for injection. The mean interval between instillation and laser activation was 21.3 ± 2.4 min.
Immediately before surgery, both eyes received topical anesthesia with 0.5% proxymetacaine hydrochloride. Study drops were identical in appearance and were administered by an independent staff member not involved in surgery or outcome assessment to ensure masking.
Randomization and masking
Treatment allocation (brimonidine vs. control) was performed at the eye level using a coin toss by an independent staff member, who also administered the drops and recorded allocation.
Surgeons, patients, and outcome assessors were masked to treatment assignment. Because subconjunctival hemorrhage is visually apparent, complete intraoperative masking of the surgeon was not feasible. However, all postoperative Day 1 assessments, including symptom evaluation and slit-lamp examination, were performed by a masked examiner using standardized forms.
Surgical techniques
LASIK technique
Flaps were created using the Ziemer FEMTO LDV “Classic” femtosecond laser (Ziemer Ophthalmic Systems AG, Port, Switzerland), targeting a thickness of 110 µm and a diameter of 8.5-9.5 mm, according to keratometry.
Three gentian-violet marks were placed before flap lifting to aid repositioning. Stromal ablation was performed using the WaveLight EX500 excimer laser (Alcon Laboratories, Fort Worth, Texas). The stromal bed was irrigated with balanced saline solution, and the flap was repositioned and dried with cellulose sponges. No bandage contact lens was used.
PRK technique
The central epithelium was mechanically removed within a marked oval optical zone using a blunt spatula. A cellulose sponge cooled with balanced saline solution (0°C-4°C) was applied before and immediately after ablation to reduce corneal nerve sensitivity.
Stromal ablation was performed using the WaveLight EX500 excimer laser. Mitomycin-C 0.02% was applied for a duration proportional to ablation depth, followed by thorough irrigation with balanced saline solution. A silicone hydrogel bandage contact lens was placed.
Postoperative regimen
Postoperative treatment was standardized.
LASIK eyes received prednisolone acetate 10 mg/mL every 6 h, gatifloxacin 3 mg/mL every 8 h, and sodium hyaluronate 0.15% every 4 h, with oral dipyrone (500 mg) as needed.
PRK eyes received fluorometholone 1 mg/g every 8 h, gatifloxacin 3 mg/mL every 8 h, ketorolac trometamol 5 mg/mL every 8 h, and sodium hyaluronate 0.15% hourly, along with codeine (30 mg) plus paracetamol (500 mg) every 12 h.
Outcomes
Pupil diameter was measured immediately before excimer ablation using an infrared pupillometer integrated into the excimer platform. As pre-instillation measurements were not obtained, pre-ablation pupil diameter was used as an intraoperative surrogate for potential drug-induced miosis.
On postoperative Day 1, a masked examiner evaluated each eye using a standardized checklist. Patients rated eight predefined symptoms (discomfort, pain, burning, stinging, irritation, itching, tearing, and foreign-body sensation) separately for each eye on a 0-10 scale (0=none; 10=worst). Symptoms were elicited systematically rather than recorded spontaneously.
A prespecified composite symptom score (primary endpoint) was calculated as the mean of the eight symptom ratings, with equal weighting.
Subconjunctival hemorrhage (presence/absence) was assessed by slit-lamp examination. In LASIK cases, both intraoperative and early postoperative hemorrhage were recorded.
The primary endpoints were Day 1 postoperative signs and symptoms. Follow-up at Days 7, 13, 19, and 180 was conducted as part of routine care.
Bias mitigation related to symptom assessment
To minimize suggestion bias, symptom assessment was performed using a standardized form that did not disclose treatment allocation or require patients to identify the treated eye.
Adherence controls
The use of cooled balanced saline solution in PRK followed a standardized protocol. Postoperative regimens were reinforced both verbally and in writing. On postoperative Day 1, the use of prescribed oral analgesics was recorded(9).
Statistical analysis
The eye was considered the unit of analysis in this contralateral paired design.
Categorical variables were compared using McNemar’s test, and continuous paired data were analyzed using the paired Student’s t test. Normality was assumed based on the central limit theorem for sample sizes ≥30.
A two-sided α level of 0.05 was considered statistically significant. The primary analysis focused on the composite symptom score. Individual symptoms were analyzed as exploratory outcomes without adjustment for multiple comparisons.
Statistical analyses were performed using SPSS version 20.0 (IBM Corp., Armonk, New York) and Stata version 17 (StataCorp LLC, College Station, Texas).
Sample size considerations
Based on prior variability in subconjunctival hemorrhage after refractive surgery, approximately 63 patients (63 paired observations; 126 eyes) were estimated to provide 80% power (α=0.05) to detect a clinically meaningful difference in symptom scores between groups.
A total of 124 patients (124 paired observations; 248 eyes) were enrolled, exceeding the required sample size.
RESULTS
Sample characterization
A total of 124 patients were included: 54 (43.5%) in the LASIK group and 70 (56.5%) in the PRK group. In the LASIK cohort, 30 patients (55.6%) were women, and 24 (44.4%) were men, with a mean age of 33.5 ± 8.6 yr (range, 18-51 yr). In the PRK group, 48 patients (68.6%) were women, and 22 (31.4%) were men, with a mean age of 30.2 ± 7.2 yr (range, 19-52 yr). No significant demographic differences were observed between the groups. All patients completed the postoperative Day 1 assessment.
Pupil size
In the LASIK group, the mean pupil size was 2.63 ± 0.47 mm in eyes pretreated with diluted brimonidine and 2.69 ± 0.42 mm in contralateral control eyes, with no significant difference (p=0.273). In the PRK group, the mean pupil size was 2.56 ± 0.44 mm in brimonidine-treated eyes and 2.61 ± 0.39 mm in control eyes, also showing no significant difference (p=0.116). These findings indicate that 0.025% brimonidine does not significantly affect pupillary diameter in either surgical technique.
Subconjunctival hemorrhage
Subconjunctival hemorrhage was prespecified and systematically recorded only in the LASIK group, in which suction-related conjunctival or limbal bleeding is a known intraoperative occurrence. This outcome was not prespecified for PRK and was therefore not recorded in a standardized manner.
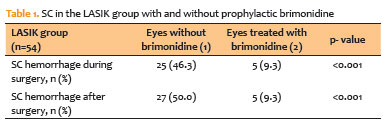
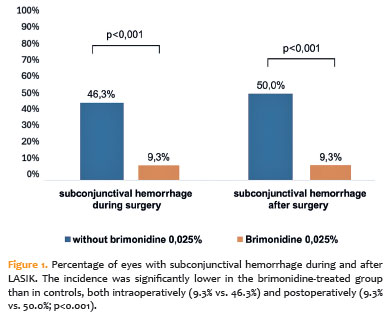
In the LASIK group, intraoperative subconjunctival hemorrhage occurred in five eyes (9.3%) treated with brimonidine compared with 25 eyes (46.3%) in the control group (p<0.001). Postoperatively, hemorrhage was observed in five eyes (9.3%) in the brimonidine group versus 27 eyes (50.0%) in controls (p<0.001). These results demonstrate a significant protective effect of prophylactic brimonidine against both intraoperative and postoperative subconjunctival hemorrhage (Table 1 and Figure 1).
Postoperative symptoms
LASIK
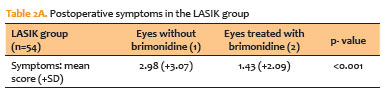
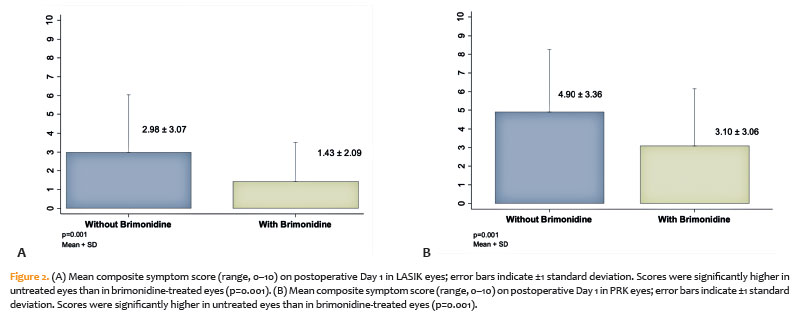
On postoperative Day 1, 29.6% of LASIK patients reported no symptoms. Among symptomatic patients, the most common complaint was foreign-body sensation (27.8%), followed by tearing, burning, and mild discomfort. The mean composite symptom score was significantly higher in control eyes than in brimonidine-treated eyes (p=0.001; table 2A and Figure 2A).
PRK
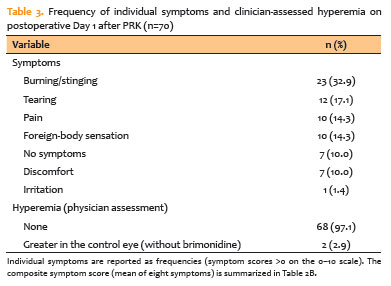
In the PRK group, the most frequently reported symptoms were burning or stinging (32.9%) and tearing (17.1%), whereas photophobia and discomfort were less common. The mean composite symptom score was significantly higher in control eyes than in brimonidine-treated eyes (p=0.001; Table 2B and Figure 2B). Individual symptom frequencies are presented in table 3.
Follow-up beyond Day 1 in both groups
Patients were scheduled for routine follow-up at postoperative Days 7, 13, 19, and 180. However, because the prespecified endpoints were limited to postoperative Day 1, data from subsequent visits were not collected using standardized research instruments and were therefore excluded from formal analysis.
Illustrative cases
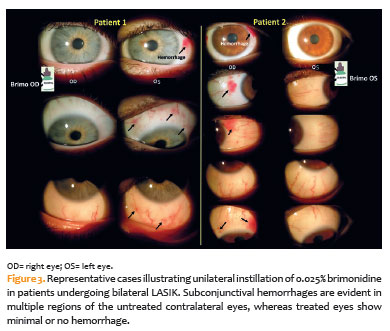
Figure 3 provides photographic evidence demonstrating a marked contrast in postoperative conjunctival hemorrhage between treated and untreated eyes.
DISCUSSION
This study extends previous LASIK-focused research by demonstrating that a very low concentration of brimonidine (0.025%) provides early clinical benefits in both LASIK and PRK without the flap-related complications reported at higher concentrations(5-7,20,24-27). Prior studies using 0.1%-0.2% brimonidine consistently reported reduced subconjunctival hemorrhage but raised safety concerns, particularly flap instability or dislocation, likely due to excessive vasoconstriction. Notably, Muñoz et al.(5,6,24,25) reported flap dislocation with 0.2% brimonidine in femtosecond LASIK. In contrast, no such events were observed in our cohort using 0.025% brimonidine. Although femtosecond flaps are generally more stable than microkeratome flaps, the findings of Muñoz et al.(5) suggest that dose reduction may provide an additional safety margin even with femtosecond platforms.
Pupil dynamics remained stable with low-dose brimonidine. Because excimer laser centration and eye-tracking accuracy can be affected by pupillary fluctuations, the absence of significant differences in pre-ablation pupil diameter between treated and control eyes in both LASIK and PRK supports procedural precision without pharmacologically induced miosis(13-16,19-21). These findings reduce concerns regarding decentration or cyclotorsion associated with drug-induced pupillary changes(13-16).
The PRK arm contributes novel data to a relatively understudied area. Epithelial removal in PRK is typically associated with substantial early postoperative discomfort. In this contralateral-eye study, brimonidine-treated eyes exhibited a lower symptom burden on postoperative Day 1 compared with controls (Table 2B and Figure 2B), with individual symptom frequencies detailed in Table 3. These findings are consistent with prior evidence from anterior segment and dermatologic studies, in which brimonidine reduced postoperative redness and prolonged the effects of topical anesthetics, potentially through vasoconstriction and modulation of nociceptive pathways(18,19,27). Although this study was not designed to evaluate anesthetic-sparing effects, the observed reduction in symptoms suggests a clinically meaningful improvement in patient comfort beyond cosmetic benefits.
In the LASIK cohort, the antihemorrhagic effect of brimonidine corroborates previous findings(20,24,25). Brimonidine-treated eyes demonstrated significantly fewer intraoperative and immediate postoperative subconjunctival hemorrhages than control eyes (Table 1 and Figure 1), without compromising flap stability or altering pupil size. Clinically, reducing early hyperemia and hemorrhage may improve patient experience by decreasing anxiety, minimizing unplanned postoperative visits, and enhancing perceived surgical success. This benefit may be particularly relevant in PRK, where early postoperative discomfort is more pronounced(5-8,10-12,25-30).
To minimize bias, postoperative Day 1 symptom assessments were conducted under masked conditions using standardized, neutral prompts without identifying the treated eye. Objective endpoints, such as the presence of subconjunctival hemorrhage, further reduced susceptibility to expectation bias. Symmetrical perioperative regimens in both eyes minimized confounding factors, including adherence-related variability. Oral analgesic use on Day 1 was recorded; in a contralateral-eye design, any systemic analgesic effect would likely bias results toward the null rather than exaggerate inter-eye differences. Because PRK does not involve a suction ring, subconjunctival hemorrhage was not prespecified as an endpoint in this group; therefore, PRK analyses focused on clinically relevant outcomes such as early symptoms and clinician-assessed hyperemia. Visual and refractive outcomes were not prespecified and were not analyzed.
This study has several limitations. The primary analyses were restricted to Day 1 outcomes; longer follow-up is needed to assess durability and delayed adverse effects, including ocular surface changes. The study population consisted of otherwise healthy individuals undergoing elective surgery, which may limit generalizability to patients with ocular surface disease or glaucoma. Corneal nerve parameters and validated quality-of-life measures were not assessed. Although higher concentrations of brimonidine have been associated with potential neuroprotective effects(23), it remains unclear whether similar benefits occur at a concentration of 0.025%. Enhancement rates up to 180 days were not evaluated, precluding comparison with historical data (e.g., Walter et al.(6)). The study was not powered to detect rare events such as flap dislocation or enhancement. Additionally, generalizability to commercially available formulations may be limited, as compounded preparations can differ in composition (e.g., vehicle, pH, osmolality, and preservative content), potentially influencing tolerability and clinical effects(20,21,30). Finally, although prespecified, the composite symptom score was not a validated patient-reported outcome measure and was intended as a pragmatic assessment of early postoperative symptoms.
In summary, brimonidine 0.025% reduced early subconjunctival hemorrhage and postoperative discomfort in LASIK and decreased discomfort in PRK, without affecting pupil diameter or compromising flap integrity. These findings reconcile the known efficacy of brimonidine with an improved safety profile suitable for contemporary refractive surgery. Low-concentration brimonidine (0.025%) represents a simple and effective adjunct for enhancing the early postoperative experience.
AUTHOR CONTRIBUTIONS:
Significant contribution to conception and design: Natália Fernandes Gonçalves Napolitano, Ana Vega Carreiro de Freitas, Luís Gustavo de Imparato Rodrigues Ribeiro, Daniella Villas Boas Fairbanks, Fernando Antonio Galhardo Tarcha, Vagner Loduca Lima, Bernardo Kaplan Moscovici, Edmundo José Velasco Martinelli. Data Acquisition: Natália Fernandes Gonçalves Napolitano, Ana Vega Carreiro de Freitas, Luís Gustavo de Imparato Rodrigues Ribeiro, Daniella Villas Boas Fairbanks, Fernando Antonio Galhardo Tarcha, Vagner Loduca Lima, Bernardo Kaplan Moscovici, Edmundo José Velasco Martinelli. Data Analysis and interpretation: Natália Fernandes Gonçalves Napolitano, Ana Vega Carreiro de Freitas, Luís Gustavo de Imparato Rodrigues Ribeiro, Daniella Villas Boas Fairbanks, Fernando Antonio Galhardo Tarcha, Bernardo Kaplan Moscovici. Manuscript Drafting: Natália Fernandes Gonçalves Napolitano, Ana Vega Carreiro de Freitas, Daniella Villas Boas Fairbanks, Bernardo Kaplan Moscovici. Significant intellectual contente revision of the manuscript: Luís Gustavo de Imparato Rodrigues Ribeiro, Fernando Antonio Galhardo Tarcha, Vagner Loduca Lima, Edmundo José Velasco Martinelli, Bernardo Kaplan Moscovici. Final approval of the submitted manuscript: Natália Fernandes Gonçalves Napolitano, Ana Vega Carreiro de Freitas, Luís Gustavo de Imparato Rodrigues Ribeiro, Daniella Villas Boas Fairbanks, Fernando Antonio Galhardo Tarcha, Vagner Loduca Lima, Bernardo Kaplan Moscovici, Edmundo José Velasco Martinelli. Statistical analysis: Bernardo Kaplan Moscovici, Ana Vega Carreiro de Freitas. Obtaining funding: not applicable. Supervision of Administrative, technical, or material support: Luís Gustavo de Imparato Rodrigues Ribeiro, Vagner Loduca Lima. Research group leadership: Bernardo Kaplan Moscovici, Ana Vega Carreiro de Freitas, Edmundo José Velasco Martinelli.
REFERENCES
1. Kim TI, Alió Del Barrio JL, Wilkins M, Cochener B, Ang M. Refractive surgery. Lancet. 2019;393(10185):2085-98.
2. Sandoval HP, Donnenfeld ED, Kohnen T, Lindstrom RL, Potvin R, Tremblay DM, et al. Modern laser in situ keratomileusis outcomes. J Cataract Refract Surg. 2016;42(8):1224-34.
3. Piovella M, Camesasca FI, Fattori C. Excimer laser photorefractive keratectomy for high myopia: four-year experience with a multiple zone technique. Ophthalmology. 1997;104(10):1554-65.
4. Betz J, Behrens H, Harkness BM, Stutzman R, Chamberlain W, Blanco MP, et al. Ocular pain after refractive surgery: interim analysis of frequency and risk factors. Ophthalmology. 2023;130(7):692-701.
5. Muñoz G, Albarrán-Diego C, Sakla HF, Javaloy J. Increased risk for flap dislocation with perioperative brimonidine use in femtosecond laser in situ keratomileusis. J Cataract Refract Surg. 2009;35(8):1338-42.
6. Walter KA, Gilbert DD. The adverse effect of perioperative brimonidine tartrate 0.2% on flap adherence and enhancement rates in laser in situ keratomileusis patients. Ophthalmology. 2001;108(8):1434-8.
7. Norden RA. Effect of prophylactic brimonidine on bleeding complications and flap adherence after laser in situ keratomileusis. J Refract Surg. 2002;18(4):468-71.
8. Wen D, McAlinden C, Flitcroft I, Tu R, Wang Q, Alió J, et al. Postoperative efficacy, predictability, safety, and visual quality of laser corneal refractive surgery: a network meta-analysis. Am J Ophthalmol. 2017;178:65-78.
9. Martinelli EJ. Refinamentos nas cirurgias fotorrefrativas. In: Santhiago MR, Chamon W, editores. Cirurgia refrativa. Rio de Janeiro: Cultura Médica; 2017. Cap 45, p.296-9.
10. Mohebbi M, Rafat-Nejad A, Mohammadi SF, Asna-Ashari K, Kasiri M, Heidari-Keshel S, et al. Postphotorefractive keratectomy pain and corneal sub-basal nerve density. J Ophthalmic Vis Res. 2017;12(2):151-5.
11. Jabbur NS, Sakatani K, O’Brien TP. Survey of complications and recommendations for management in dissatisfied patients seeking a consultation after refractive surgery. J Cataract Refract Surg. 2004;30(9):1867-74.
12. Rahman MQ, Ramaesh K, Montgomery DM. Brimonidine for glaucoma. Expert Opin Drug Saf. 2010;9(3):483-91.
13. Torkildsen GL, Sanfilippo CM, DeCory HH, Gomes PJ. Evaluation of efficacy and safety of brimonidine tartrate ophthalmic solution, 0.025% for treatment of ocular redness. Curr Eye Res. 2018;43(1):43-51.
14. McLaurin E, Cavet ME, Gomes PJ, Ciolino JB. Brimonidine ophthalmic solution 0.025% for reduction of ocular redness. Optom Vis Sci. 2018;95(3):264-71.
15. Ackerman SL, Torkildsen GL, McLaurin E, Vittitow JL. Low-dose brimonidine for relief of ocular redness: integrated analysis of four clinical trials. Clin Exp Optom. 2019;102(2):131-9.
16. Lee JS, Kim CY. Brimonidine tartrate ophthalmic solution 0.025% for redness relief: an overview of safety and efficacy. Expert Rev Clin Pharmacol. 2022;15(8):911-9.
17. Steigleman WA, Rose-Nussbaumer J, Al-Mohtaseb Z, Santhiago MR, Lin CC, Pantanelli SM, et al. Management of pain after photorefractive keratectomy: a report by the American Academy of Ophthalmology. Ophthalmology. 2023;130(1):87-98.
18. Kwon HJ, Kim JM, Jeong GJ, Lee SJ, Lee HW, Park KY, et al. Topical brimonidine as an effective adjuvant to local anesthetics for post treatment erythema and pain reduction. Ann Dermatol. 2019;31(3):315-9.
19. Rodrigues PF, Moscovici BK, Hirai F, Mannis MJ, de Freitas D, Campos M, et al. Vision-related quality of life in patients with keratoconus with enantiomorphic topography after bilateral intrastromal corneal ring implantation. Cornea. 2024;43(2):190-4.
20. Hosten LO, Snyder C. Over-the-counter ocular decongestants in the United States - mechanisms of action and clinical utility for management of ocular redness. Clin Optom (Auckl). 2020;12:95-105.
21. Food and Drug Administration (FDA). Approval letter for Lumify (brimonidine tartrate ophthalmic solution, 0.025%). NDA 208144. United States: Silver Spring (MD): FDA; 2017. [cited 2024 Sep 7]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/208144Orig1s0000Approv.pdf
22. McCarty TM, Hardten DR, Anderson NJ, Rosheim K, Samuelson TW. Evaluation of neuroprotective qualities of brimonidine during LASIK. Ophthalmology. 2003;110(8):1615-25.
23. Rodríguez-Galietero A, Martínez JV, Del Buey A, Bescós JA. Use of brimonidine before LASIK with femtosecond laser-created flaps for the correction of myopia: a contralateral eye study. J Refract Surg. 2010;26(1):28-32.
24. Pasquali TA, Aufderheide A, Brinton JP, Avila MR, Stahl ED, Durrie DS. Dilute brimonidine to improve patient comfort and subconjunctival hemorrhage after LASIK. J Refract Surg. 2013;29(7):469-75.
25. Hong S, Kim CY, Seong GJ, Han SH. Effect of prophylactic brimonidine instillation on bleeding during strabismus surgery in adults. Am J Ophthalmol. 2007;144(3):469-70.
26. Ucar F, Cetinkaya S. The results of preoperative topical brimonidine usage in pterygium surgery. J Ocul Pharmacol Ther. 2020;36(4):234-7.
27. Rodrigues PF, Moscovici BK, Lamazales L, Freitas MM, Gomes JÁ, Nosé W, et al. Measurement of the visual axis through two different methods: quantification and differences for measuring chord μ. Arq Bras Oftalmol. 2023;87(4):e2022-0035.
28. Rymer P, Moscovici BK, Gomes R, Couto B, Schor P, Campos M. Pain response and symptoms in photorefractive keratectomy: mechanical de-epithelization compared with transepithelial ablation. Arq Bras Oftalmol. 2021;85(2):152-7.
29. Colombo-Barboza GN, Rodrigues PF, Colombo-Barboza FD, Moscovici BK, Colombo-Barboza LR, Colombo-Barboza MN, et al. Radial keratotomy: background and how to manage these patients nowadays. BMC Ophthalmol. 2024;24(1):9.
30. Moscovici BK, Cesar AS, Nishiwaki-Dantas MC, Mayor SA, Marta AC, Marques JC. [Atopic keratoconjunctivitis in patients of the pediatric dermatology ambulatory in a reference center]. Arq Bras Oftalmol. 2009;72(6):805-10. Portuguese.
Data Availability Statement: The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request, subject to justified conditions.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Richar Y. Hida
Submitted for publication:
November 7, 2025.
Accepted for publication:
February 25, 2026.
Approved by the following research ethics committee: H.Olhos Paulista (CAAE: 81430024.5.3001.9867) and Centro Universitário FMABC (CAAE: 81430024.5.1001.0082).
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.