Arq. Bras. Oftalmol. 2026; 89 (4): 10.5935/0004-2749.2025-0313
Total: 641
Paula Virginia Brom dos Santos Soares1; Elisa Moya Kazmarek1; Elisabeth Brandao Guimaraes1; Marizilda Rita de Andrade1; Renato Giovedi Filho1; Bernardo Kaplan Moscovici2,3
DOI: 10.5935/0004-2749.2025-0313
ABSTRACT
PURPOSE: To compare clinical outcomes associated with different intraoperative mitomycin C exposure times during photorefractive keratectomy for myopia and astigmatism correction.
METHODS: This prospective, comparative, contralateral-eye study included 41 patients (82 eyes), comprising 28 eyes with ablation <60µm and 13 eyes with ablation >60µm, who underwent photorefractive keratectomy with varying mitomycin C application times based on ablation depth. In eyes with ablation <60µm, mitomycin C was applied for 15 s in one eye and 30 s in the fellow eye. In eyes with ablation >60µm, mitomycin C was applied for 30 s in one eye and 60 s in the fellow eye. Outcomes included visual acuity, postoperative pain (visual analog scale), subjective tearing, corneal haze, and refractive results at 3 months.
RESULTS: No statistically significant differences were observed between mitomycin C application times within either group for postoperative pain, tearing, visual acuity, refractive outcomes (spherical, cylindrical, and spherical equivalent), or haze prevalence (p>0.05 for all comparisons). Visual acuity improved in all groups, and no eyes lost ≥2 lines of corrected distance visual acuity.
CONCLUSIONS: Shorter mitomycin C exposure times (15 or 30 s) appear to be as effective and safe as longer durations (30 or 60 s) for haze prevention after photorefractive keratectomy without compromising refractive outcomes or increasing postoperative discomfort at 3-month follow-up.
Keywords: Mitomicin/therapeutic use; Photorefractive keratectomy; Lasers, excimer; Intraoperative period; Miopia/surgery; Astigmatismo/surgery; Corneal opacity; Postoperative pain; Comparative study
INTRODUCTION
Photorefractive keratectomy (PRK) is widely used for the correction of ametropia. The procedure involves epithelial removal using a spatula, rotating brush, or diluted alcohol, followed by laser ablation of the exposed stroma(1-3). However, PRK is associated with slower visual recovery and more intense postoperative pain during the first few days, primarily due to exposure of corneal nerves and the release of cytokines and other inflammatory mediators after surgery(3-6).
PRK is also associated with several complications, including regression, hypo- or overcorrection, corneal haze, corneal ectasia, decentered ablation, and higher-order aberrations. Among these, corneal haze (subepithelial fibrosis) is one of the most common. Corneal transparency depends on the highly organized structure and distribution of collagen fibers and keratocytes as well as their phenotypic stability(5-7).
Haze results from an abnormal wound-healing response following epithelial and stromal injury, accompanied by inflammation that promotes keratocyte migration, proliferation, and differentiation into myofibroblasts. This process leads to disorganized collagen deposition and stromal fibrosis, resulting in reduced corneal transparency(7,8).
Risk factors for haze development include higher ablation depth, delayed re-epithelialization, and stromal irregularity(7). Clinically, two types of corneal haze have been described: type 1, which appears 1–3 months after surgery and usually resolves within 1 yr, and type 2, which appears after 3 months, may persist for more than 3 yr, and is considered late-onset corneal opacity(5). Preventive strategies include intraoperative mitomycin C (MMC), postoperative corticosteroid eye drops, topical nonsteroidal anti-inflammatory drugs, oral vitamin C, and ultraviolet protection(6-9).
MMC was first introduced in ophthalmology in 1963 as an adjunct to pterygium excision. Its prophylactic use in PRK to reduce haze formation is well established, with demonstrated safety and efficacy as an adjuvant therapy(10,11). MMC inhibits keratocyte activation and differentiation into myofibroblasts and reduces disorganized extracellular matrix deposition within the corneal stroma(12). These effects are achieved through direct application to the stromal bed after photoablation, typically at a concentration of 0.02% for 12 s to 2 min(13).
MMC has a broad range of applications in ophthalmology, including glaucoma surgery, strabismus surgery, pterygium excision, conjunctival and corneal neoplasms, ocular cicatricial pemphigoid, vernal keratoconjunctivitis, and refractive procedures. Reported adverse effects include photosensitivity, ocular pain, corneal edema, conjunctival hyperemia, punctal occlusion, scleral thinning, and, rarely, perforation(7-10,14).
Despite its established use, there is no consensus regarding the optimal MMC regimen in PRK, and substantial variability remains in clinical protocols(6,10,11). Although most studies use MMC at a concentration of 0.02%, exposure times vary widely, ranging from approximately 10–15 s to 1–2 min, particularly in eyes at higher risk for haze development(11,15-22).
Because greater ablation depth and higher degrees of ametropia are associated with a stronger wound-healing response, longer MMC exposure times have traditionally been used in these cases to enhance suppression of keratocyte activity(5,7,11,15,17). However, recent comparative studies suggest that shorter exposure times may also be effective, raising questions about the additional benefit of prolonged application(17,22).
Given this variability and lack of standardization, this study aimed to compare the effects of different MMC exposure times on refractive outcomes, postoperative pain, tearing, and corneal haze following PRK surgery.
METHODS
Study design
This prospective, contralateral-eye, comparative study analyzed the medical records of patients who underwent PRK between September 2023 and March 2024. All patients provided written informed consent before surgery. The study protocol was approved by the institutional Research Ethics Committee (Protocol No. 82515124.8.0000.5479).
Inclusion and exclusion criteria
Patients were eligible if they were aged ≥21 yr, had documented refractive stability for at least 12 months before surgery, and had no contraindications for refractive surgery based on Scheimpflug tomography (Pentacam; Oculus, Wetzlar, Germany). All included patients had a best-corrected visual acuity of 20/20 or better. Both eyes were required to have the same planned ablation depth (either both <60µm or both >60µm).
Patients were excluded if the residual stromal bed thickness after ablation was <350 µm, if tomography showed signs of corneal ectasia or irregularity, or if there was a history of ocular trauma, previous ocular surgery, or systemic/ocular conditions affecting corneal healing (e.g., collagen vascular disorders, diabetes mellitus, or severe dry eye disease). Patients with lens opacities, retinal disease, glaucoma, or planned monovision correction were also excluded. In addition, patients with anisometropia or different ablation depths between eyes (threshold: 60 µm) were excluded.
Preoperative assessment
All patients underwent a standardized preoperative evaluation. Uncorrected and best-corrected visual acuity were measured using a 6-m Snellen chart. Manifest and cycloplegic refractions were obtained using an autorefractor followed by manual refinement. Corneal tomography was performed using the Pentacam system (Oculus, Wetzlar, Germany). A complete ophthalmological examination was performed in all cases.
Surgical technique
All procedures were performed as sequential bilateral PRK by the same experienced surgeon using the Schwind Amaris 1050s excimer laser (Schwind, Kleinostheim, Germany). After topical anesthesia with 0.5% proparacaine hydrochloride, the corneal epithelium was mechanically removed using a blunt spatula. Excimer laser ablation was then performed according to the patient’s refractive error and standard surgical MMC; 0.02%) was applied directly to the stromal bed after ablation, with exposure times determined by ablation depth. In corneas with an ablation depth <60 µm (Group 1), MMC was applied for 15 s in the right eye (OD) and 30 s in the left eye (OS). In corneas with an ablation depth >60 µm (Group 2), MMC was applied for 30 s in the OD and 60 s in the OS. These exposure times were based on the institutional protocol.
After MMC application, the corneal surface was irrigated with 20 mL of balanced saline solution. A therapeutic contact lens (PureVision 2; Bausch & Lomb, Rochester, New York) was then placed, and a protective rigid eye shield was applied.
Postoperative care and follow-up
All patients followed a standardized postoperative regimen. This included topical moxifloxacin 0.5% and dexamethasone 1% eye drops every 4 h, ketorolac tromethamine 0.5% eye drops every 12 h, and preservative-free lubricating drops every 4 h. Oral analgesics (paracetamol 500 mg and codeine 30 mg) were prescribed as needed for pain control.
Patients were examined on postoperative days 1, 7, and 30, and at 3 months. At each visit, pain was assessed using a visual analog scale (0=no pain; 10=worst pain). Patients were also asked to compare tearing between eyes (less, equal, or greater tearing).
At the 3-month visit, corneal haze was evaluated by slit-lamp biomicroscopy and graded using the Fantes scale. For statistical analysis, haze was categorized as present or absent (any grade >0)(23). Refractive outcomes, including spherical, cylindrical, and spherical equivalent (SE), were also recorded.
Statistical analysis
Statistical analyses were performed using R software (version 4.2.0; R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics (mean, standard deviation, median, and interquartile range) were calculated for all variables.
Comparisons between MMC exposure times were performed using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. A p-value < 0.05 was considered statistically significant.
RESULTS
A total of 41 patients were included and divided into two groups according to corneal ablation depth. Group 1 comprised 28 eyes with an ablation depth <60 µm, whereas Group 2 comprised 13 eyes with an ablation depth >60µm. In Group 1, the mean age was 31 ± 6 yr (range: 24–43 yr), and 19 patients (68%) were women. In Group 2, the mean age was 28 ± 3 yr (range: 24–35 yr), and six patients (46%) were women.
Group 1: Comparison of 15-s versus 30-s MMC application times
Pain was evaluated on postoperative days (PO) 1 and 7. On PO day 1, the mean pain scores were 2.14 ± 2.81 and 2.07 ± 2.94 in the 15- and 30-s MMC groups, respectively (Table 1). By PO day 7, mean pain scores decreased to 0.25 ± 0.59 and 0.57 ± 1.26, respectively. No statistically significant differences were observed between the two MMC exposure times.
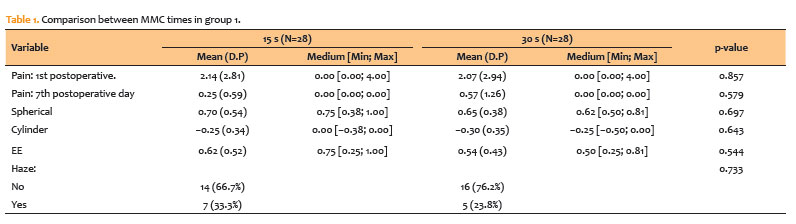
Refractive outcomes were assessed using spherical, cylindrical, and SE values. Mean spherical values were 0.70 ± 0.54 D and 0.65 ± 0.38 D in the 15- and 30-s groups, respectively (Table 1). Mean cylindrical values were −0.25 ± 0.34 D and −0.30 ± 0.35 D, respectively. Mean SE values were 0.62 ± 0.52 D and 0.54 ± 0.43 D, respectively. No statistically significant differences were found between groups for any refractive parameter.
Corneal haze was observed in 33.3% of eyes in the 15-s group and 23.8% of eyes in the 30-s group (Table 1). Most eyes (66.7% and 76.2%, respectively) showed no haze at the 3-month follow-up. The difference in haze prevalence was not statistically significant.
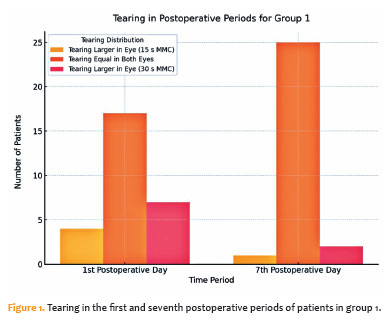
Tearing differences between the eyes are shown in figure 1. On PO day 1, 61% of patients reported equal tearing in both eyes, while 14% reported greater tearing in the 15-s eye and 25% in the 30-s eye. By PO day 7, 89% of patients reported equal tearing, whereas 4% and 7% reported greater tearing in the 15-s and 30-s groups, respectively. By PO day 30, no differences in tearing were observed between eyes.
Group 2: Comparison of 30-s versus 60-s MMC application times
Pain scores on PO day 1 were 3.15 ± 3.31 and 4.15 ± 3.74 in the 30- and 60-s MMC groups, respectively (Table 2). On PO day 7, mean pain scores decreased to 0.77 ± 1.24 and 1.54 ± 2.37, respectively. However, these differences were not statistically significant.
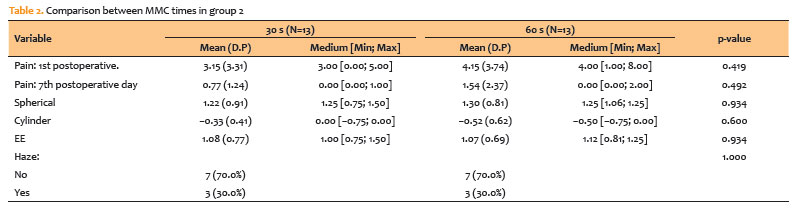
Mean spherical values were 1.22 ± 0.91 D and 1.30 ± 0.81 D in the 30- and 60-s groups, respectively (Table 2). Mean cylindrical values were −0.33 ± 0.41 D and −0.52 ± 0.62 D, respectively. Mean SE values were 1.08 ± 0.77 D and 1.07 ± 0.69 D, respectively. No statistically significant differences were observed between groups for any refractive parameter.
Corneal haze was observed in 30% of eyes in both the 30- and 60-s groups, while 70% showed no haze at the 3-month follow-up (Table 2).
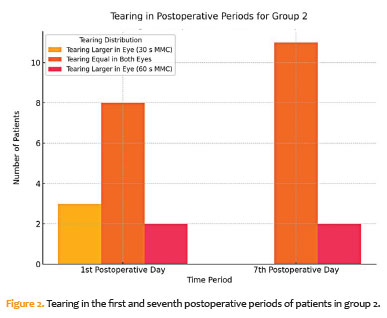
Tearing outcomes are shown in figure 2. On PO day 1, 61% of patients reported equal tearing between eyes, while 23% reported greater tearing in the 30-s eye and 16% in the 60-s eye. By PO day 7, 85% reported equal tearing; none in the 30-s group and 15% in the 60-s group reported greater tearing. By PO day 30, no differences in tearing were observed.
Figures 3 and 4 summarize visual and refractive outcomes at 3 months. In both groups, uncorrected distance visual acuity improved significantly, with most eyes achieving 20/20 or better (Figures 3A, 3F, 4A and 4F). All eyes maintained or improved corrected distance visual acuity, with no eye losing two or more lines (Figures 3B, 3C, 3G, 3H, 4B, BC, 4G and 4H).
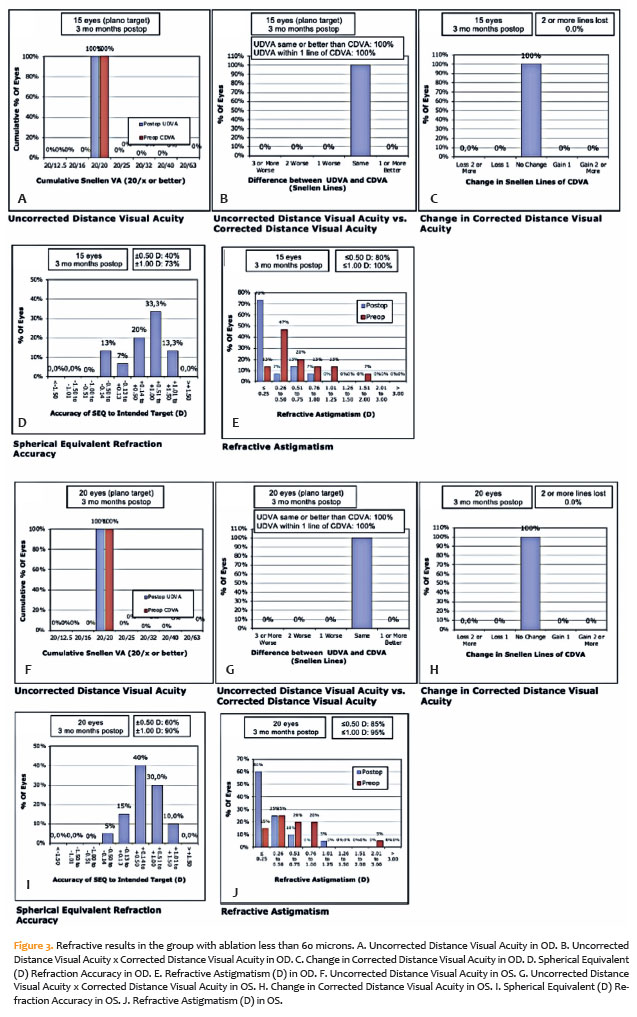
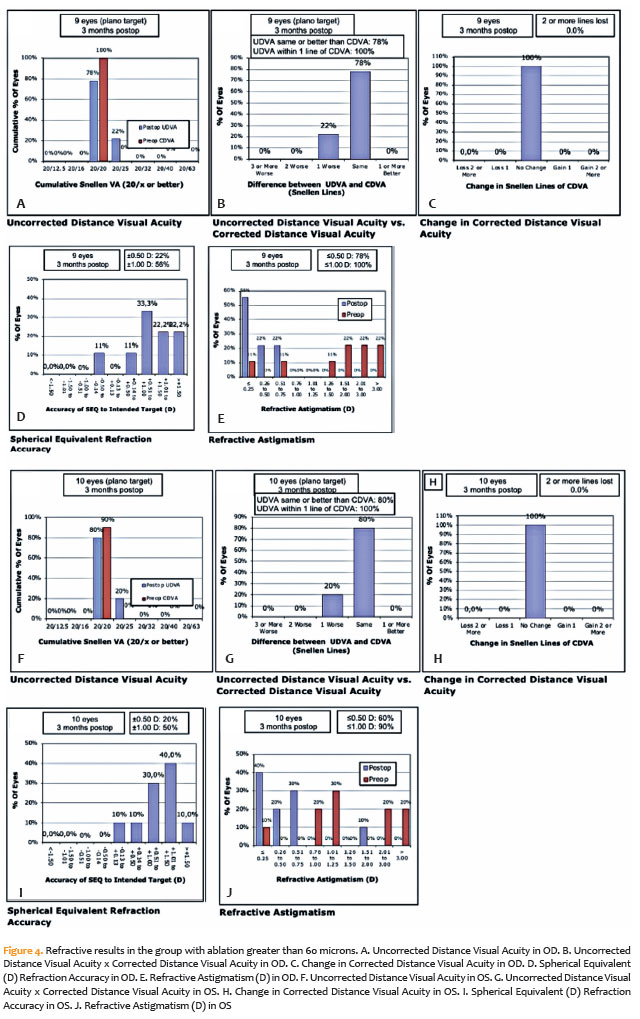
The accuracy of SE correction was high in both groups, with most eyes within ±1.00 D of target refraction (Figures 3D, 3I, 4D, and 4I). Postoperative astigmatism decreased in most eyes compared with preoperative values, with similar outcomes in both cohorts (Figures 3E, 3J, 4E, and 4J).
DISCUSSION
The literature consistently supports PRK as a safe and effective procedure with good visual outcomes. However, complications such as corneal haze and refractive variability remain concerns, mainly related to corneal wound healing. In some cases, intentional undercorrection has been used to minimize the risk of postoperative hypercorrection. The prophylactic use of intraoperative MMC has become widely adopted to reduce haze formation, with multiple studies demonstrating its efficacy and safety(7,13-22). Oliveira et al.(7) demonstrated that MMC significantly reduces haze compared with placebo, without evidence of toxicity, contributing to its widespread use in refractive surgery.
Corneal haze remains the primary concern after PRK due to its effect on visual quality. A systematic review and meta-analysis confirmed that MMC significantly reduces the incidence of corneal opacity(6). Earlier studies reported that 0.02% MMC applied for 2 min reduced haze in high myopia cases, with minimal residual haze resolving during follow-up(15). Other studies have shown that shorter exposure times (12–15 s) may be equally effective compared with longer durations (60–120 s)(16), although some reports suggest that efficacy may depend on both concentration and exposure time(12).
In the present study, no statistically significant differences were observed between MMC exposure times (15 vs. 30 s in Group 1 and 30 vs. 60 s in Group 2). These findings support the hypothesis that shorter MMC exposure times are sufficient to prevent haze after PRK and are consistent with previous reports in the literature.
Postoperative pain after PRK is primarily related to epithelial removal and corneal nerve injury, leading to the release of inflammatory mediators(3). In this study, pain and tearing were more pronounced on PO day 1 and decreased by PO day 7. However, no significant differences were found between MMC exposure times. These findings suggest that MMC does not increase postoperative discomfort, which is consistent with previous reports indicating that pain is mainly related to epithelial healing rather than MMC application(17). It should be noted that oral analgesics were prescribed as needed, which may have influenced pain perception and reduced differences between eyes. In addition, the tearing assessment was subjective, which may introduce reporting bias.
The effect of MMC on refractive outcomes remains controversial. Some studies report improved predictability, whereas others show no differences or increased variability(6,18). In the present study, no statistically significant differences were observed in spherical, cylindrical, or SE values between MMC exposure times in either group. These findings suggest that refractive outcomes are more strongly influenced by individual healing characteristics and corneal biomechanics than by MMC duration.
Concerns regarding MMC-induced hypercorrection have been raised; however, no consistent refractive shift was observed in this study. These findings are consistent with Hofmeister et al.(18), who reported that shorter MMC exposure does not compromise refractive predictability. Similarly, Chang et al.(6,13) found no significant differences between MMC-treated and non-treated eyes.
In contrast, Ghanem et al.(13) reported a tendency toward hypercorrection in MMC-treated eyes, while Sy et al.(21,22) suggested that refractive variability may be related to corneal biomechanical differences rather than MMC exposure time. These findings highlight that patient-specific factors may play a greater role than MMC duration in determining refractive outcomes(23-25).
Overall, no significant differences were observed in pain, refractive outcomes, haze incidence, or tearing between different MMC exposure times. These results suggest that shorter MMC application times (15–30 s) are as effective as longer durations (up to 60 s) in preventing haze, without compromising refractive predictability or postoperative comfort.
This study has limitations, including a relatively small sample size and a short follow-up period of 3 months, which may not capture late-onset haze. Group 2 included a limited number of patients, which may reduce statistical power. In addition, the tearing assessment was subjective, and as-needed analgesic use may have influenced pain scoring in this contralateral-eye design.
Despite these limitations, the findings support the clinical equivalence of shorter MMC exposure times compared with longer durations. This reinforces the trend toward more conservative and individualized MMC use in PRK. MMC remains an effective and safe adjunct in refractive surgery, contributing to reduced haze formation and improved visual outcomes.
ACKNOWLEDGMENTS
The authors would like to express their sincere gratitude to Dr. Niro Kasahara for his invaluable support in the statistical analysis of this study. His expertise and meticulous approach were essential in ensuring the accuracy and robustness of the findings. The authors deeply appreciate his dedication and insightful contributions throughout this work.
AUTHORS’ CONTRIBUTIONS:
Significant contribution to conception and design: Paula Virginia Brom dos Santos Soares, Elisa Moya Kazmarek, Elisabeth Brandão Guimarães, Marizilda Rita de Andrade, Renato Giovedi Filho, Bernardo Kaplan Moscovici. Data acquisition: Paula Virginia Brom dos Santos Soares, Elisa Moya Kazmarek, Elisabeth Brandão Guimarães, Marizilda Rita de Andrade, Renato Giovedi Filho. Data analysis and interpretation: Bernardo Kaplan Moscovici. Manuscript drafting: Paula Virginia Brom dos Santos Soares, Elisa Moya Kazmarek, Elisabeth Brandão Guimarães, Marizilda Rita de Andrade, Renato Giovedi Filho. Significant intellectual content revision of the manuscript: Bernardo Kaplan Moscovici. Final approval of the submitted manuscript: Paula Virginia Brom dos Santos Soares, Elisa Moya Kazmarek, Elisabeth Brandão Guimarães, Marizilda Rita de Andrade, Renato Giovedi Filho, Bernardo Kaplan Moscovici. Statistical analysis: Bernardo Kaplan Moscovici. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Bernardo Kaplan Moscovici. Research group leadership: Bernardo Kaplan Moscovici.
REFERENCES
1. Alasbali T. Transepithelial photorefractive keratectomy compared to conventional photorefractive keratectomy: a meta-analysis. J Ophthalmol. 2022;2022(1):3022672.
2. Mohan S, Gogri P, Murthy SI, Chaurasia S, Mohamed A, Dongre P. A prospective evaluation of the effect of mitomycin-C on corneal endothelium after photorefractive keratectomy for myopia correction. Middle East Afr J Ophthalmol. 2021;28(2):111–5.
3. Rymer P, Moscovici BK, Gomes R, Couto B, Schor P, Campos M. Pain response and symptoms in photorefractive keratectomy: mechanical de-epithelization compared with transepithelial ablation. Arq Bras Oftalmol [Internet]. 2022 [cited 2025 Nov 21];85(2):152–7. Available from: https://www.scielo.br/j/abo/a/kGkVN6PprTDFYSqwvNXgS6w/?lang=en
4. Moshirfar M, Wang Q, Theis J, Porter KC, Stoakes IM, Payne CJ, H, et al. Management of corneal haze after photorefractive keratectomy. Ophthalmol Ther. 2023;12(6):2841–62.
5. Spadea L, Giovannetti F. Main complications of photorefractive keratectomy and their management. Clin Ophthalmol. 2019;13:2305–15.
6. Chang YM, Liang CM, Weng TH, Chien KH, Lee CH. Mitomycin C for the prevention of corneal haze in photorefractive keratectomy: a meta-analysis and trial sequential analysis. Acta Ophthalmol. 2021;99(7):652–62.
7. Oliveira PR, Simão LF, Simão SA, Moreira H, Pereira L, Ventura LM. Prophylactic use of mitomycin C to inhibit haze formation after photorefractive keratectomy in high myopia: results after two years. Rev Bras Oftalmol. 2011;70(4):218–23.
8. Charpentier S, Keilani C, Maréchal M, Friang C, De Faria A, Froussart-Maille F, et al. Corneal haze post photorefractive keratectomy. J Fr Ophtalmol. 2021;44(9):1425–38.
9. Alfawaz AM. Haze prevention following photorefractive keratectomy in brown eyes. J Fr Ophtalmol. 2021;44(6):835–41.
10. Crespo MA, Rapuano CJ, Syed ZA. Applications of mitomycin C in cornea and external disease. Turk J Ophthalmol. 2023;53(3):175–82.
11. Piva C, Santhiago MR. Mitomycin C application in refractive surgery. Rev Bras Oftalmol. 2015;74(6):403–6.
12. Al-Mohaimeed MM. Effect of prophylactic mitomycin C on corneal endothelium following transepithelial photorefractive keratectomy in myopic patients. Clin Ophthalmol. 2022;16:2813–22.
13. Ghanem RC. Corneal wavefront-guided photorefractive keratectomy (PRK) with adjunctive mitomycin C (MMC) for the treatment of hyperopia after radial keratotomy [thesis]. São Paulo: University of São Paulo; 2010.
14. Lui Netto A, Lui GA, Lui AC, Lui TA, Andrade MR. Photorefractive keratectomy (PRK) with mitomycin C 0.02% for the management of high degree of hyperopic astigmatism following radial keratotomy. Rev Bras Oftalmol. 2009;68(3):156–60.
15. Wallau AD, Leoratti MCV, Campos M. Mitomycin C and excimer laser. Arq Bras Oftalmol. 2005;68(6):867–72.
16. Wilson SE. Biology of keratorefractive surgery: PRK, PTK, LASIK, SMILE, inlays and other refractive procedures. Exp Eye Res. 2020;198:108136.
17. Hofmeister EM, Bishop FM, Kaupp SE, Schallhorn SC. Randomized dose-response analysis of mitomycin-C to prevent haze after photorefractive keratectomy for high myopia. J Cataract Refract Surg. 2013;39(9):1358–65.
18. Sy ME, Zhang L, Yeroushalmi A, Huang D, Hamilton DR. Effect of mitomycin-C on the variance in refractive outcomes after photorefractive keratectomy. J Cataract Refract Surg. 2014;40(12):1980–4.
19. Feltrin de Barros G, Susanna BN, Brito L, Lima VL, Moscovici BK. Results of fibrin glue applied over the corneal surface immediately after pterygium surgery: a novel pain relief technique. Cornea. 2023;42(10):1327–31.
20. Moscovici BK, Rodrigues PF, Dantas MP, Okimoto JT, Naves OS, Taguchi FM, et al. Ten-year follow-up of corneal cross-linking and refractive surface ablation in patients with asymmetric corneal topography. Indian J Ophthalmol. 2023;71(9):3210–18.
21. Leccisotti A. Mitomycin C in photorefractive keratectomy: effect on epithelialization and predictability. Cornea. 2008;27(3):288–91.
22. Virasch VV, Majmudar PA, Epstein RJ, Vaidya NS, Dennis RF. Reduced application time for prophylactic mitomycin C in photorefractive keratectomy. Ophthalmology. 2010;117(5):885–9.
23. Fantes FE, Hanna KD, Waring GO 3rd, Pouliquen Y, Thompson KP, Savoldelli M. Wound healing after excimer laser keratomileusis (photorefractive keratectomy) in monkeys. Arch Ophthalmol. 1990;108(5):665–75. Comment in: Arch Ophthalmol. 1991;109(1):15.
24. Oliani CHP, Oliveira NL, Brito Martins LA, Felberg S, Colombo-Barboza MN, Colombo-Barboza GN, Moscovici BK. Lidocaine gel provides superior analgesia compared to oxybuprocaine drops in pterygium surgery: A double-masked randomized trial. Eur J Ophthalmol. 2026 Mar 10:11206721261429131.
25. Moscovici BK, Cesar AS, Nishiwaki-Dantas MC, Mayor SA, Marta AC, Marques JC. Atopic keratoconjunctivitis in patients of the pediatric dermatology ambulatory in a reference center. Arq Bras Oftalmol. 2009;72(6):805-10.portuguese.
Submitted for publication:
October 14, 2025.
Accepted for publication:
March 26, 2026.
Approved by the following research ethics committee: Santa Casa de Misericórdia de São Paulo – SCMSP (CAAE: 82515124.8.0000.5479).
Data Availability Statement: The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request, and subject to justified conditions.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Richard Y. HIda
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.