Arq. Bras. Oftalmol. 1999;62 (6 )
:697-700
| DOI: 10.1590/S0004-27491999000600008
Abstract
Objetivo: Estudar os custos de correção dos vícios de refração em grupos de pessoas de distinto poder aquisitivo. Métodos: Os autores estudaram cinqüenta pacientes portadores de vícios de refração. Estes foram separados em dois grupos: grupo I com pacientes escolhidos de forma aleatória na primeira consulta ao ambulatório de Oftalmologia do Hospital Evangélico de Curitiba (HUEC), e grupo II com voluntários médicos do HUEC e acadêmicos de medicina da Faculdade Evangélica de Medicina do Paraná (FEMPAR). Foram analisados dados referentes a sexo, faixa etária, profissão, renda, grau de instrução, uso de correção (óculos ou lentes) e seu custo, consultas oftalmológicas. Os pacientes foram submetidos ao exame oftalmológico de rotina. Resultados: Encontramos no grupo I predominância de pacientes de meia idade (48,5 anos), com renda entre 1 a 5 salários mínimos (SM) e hipermétropes; e no grupo II, pacientes jovens (24,4 anos), com renda acima de 20 SM e míopes foram mais freqüentes. Conclusão: O gasto médio anual com óculos fica no mínimo em R$ 46,50 (0,3 SM); com lentes de contato, no mínimo R$ 196,66 (1,4 SM); e com cirurgia refrativa em R$ 800,00 (5,9 SM). O estudo sugere a cirurgia refrativa como boa indicação para ambos os grupos.
Keywords: Vícios de refração; Aspectos socioeconômicos
Arq. Bras. Oftalmol. 2023;86 (3 )
:1-5
| DOI: 10.5935/0004-2749.20230031
Abstract
Objetivo: Descrever os resultados clínicos do tratamento do crescimento epitelial através da técnica de remoção manual seguido da utilização de um compressor de ar comprimido aquecido após a cirurgia de laser in situ keratomileusis (LASIK).
Métodos: Vinte olhos de 17 pacientes foram incluídos no estudo. Cada paciente havia sido submetido a cirurgia de LASIK com presença de crescimento epitelial e foi submetido a tratamento cirúrgico para sua retirada. O objetivo primário foi identificar a presença de crescimento epitelial recorrente ao final de 3 meses de seguimento. Os objetivos secundários foram as medidas de acuidade visual sem correção, acuidade visual com correção, e complicações pós-operatórias.
Resultados: Dez pacientes (58,8%) eram homens e 7 mulheres. Oito olhos de sete (41,2%) pacientes apresentavam cirurgia de LASIK primária e 12 olhos de 10 pacientes tinham cirurgia de LASIK com retratamento; dezesseis olhos (80%) utilizaram microcerátomo manual e quatro (20%) laser de femtosegundo. A média de idade no momento da cirurgia de remoção do epitélio era de 37,0 anos ± 9,3 (DP) (variando de 24 a 55 anos). Ocorreu recidiva do crescimento epithelial em dois olhos (10%) após 3 meses de seguimento. A acuidade visual sem correção antes da cirurgia era de 0,07 ± 0,09 logMAR, e após a cirurgia passou para 0,02 ± 0,04 logMAR (p=0,06). A chance (odds ration) de aparecimento do crescimento epithelial após uma reoperação de LASIK é 29,41 vezes maior do que no LASIK primário.
Conclusão: A técnica de remoção epitelial manual seguida da utilização de ar comprimido aquecido é segura e efetiva no tratamento do crescimento epitelial após LASIK. Ao final do último acompanhamento, nenhum olho apresentou perda de linhas de visão.
Keywords: Epitélio/crescimento & desenvolvimento; Endotélio corneano; Doenças da córnea; Ceratomileuse assistida por excimer laser in situ; Ceratectomia fotorrefrativa; Procedimentos cirúrgicos refrativos; Acuidade visual
Arq. Bras. Oftalmol. 2023;86 (5 )
:1-6
| DOI: 10.5935/0004-2749.20230070
Abstract
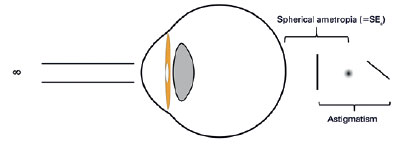
Objetivo: A refração pós-operatória na cirurgia moderna de catarata por microincisão ganha ainda mais importância em pacientes com cirurgia prévia de ceratomileuse in situ assistida por laser (LASIK). As alterações astigmáticas induzidas cirurgicamente nesses olhos podem diferir não apenas em magnitude, mas também em direção em comparação com córneas virgens. O objetivo deste estudo foi comparar as alterações astigmáticas induzidas cirurgicamente após cirurgia de catarata por microincisão entre córneas pós-LASIK e olhos virgens.
Métodos: Foi revisada uma série de casos de cirurgia de catarata por microincisão em olhos com e sem cirurgia LASIK anterior. Os dados demográficos, o comprimento axial no momento da cirurgia de catarata, a espessura central da córnea, os valores esféricos e cilíndricos, as leituras da ceratometria e o astigmatismo corneano posterior pós-operatório foram avaliados retrospectivamente. O método Alpins modificado foi usado para análise vetorial astigmática e foram avaliados o astigmatismo basal, o astigmatismo induzido cirurgicamente, o vetor de diferença, o efeito de achatamento e o torque.
Resultados: Ao todo, 42 olhos de 24 indivíduos foram avaliados. O Grupo I consistiu em 14 olhos com LASIK prévio; o Grupo II incluiu 28 olhos sem qualquer cirurgia refrativa. A média da espessura corneana central pré-operatória no Grupo I foi significativamente mais fina (p=0,012). Não houve diferença significativa no astigmatismo basal entre os grupos em termos de magnitude e vetores de potência. Após a cirurgia de catarata por microincisão, não houve diferenças significativas nos valores médios esféricos, cilíndricos e leituras médias de ceratometria (todos com p>0,05). No entanto, o astigmatismo induzido cirurgicamente e o vetor de diferença foram significativamente maiores no componente do vetor J45 em olhos pós-LASIK, e o efeito de aumento da inclinação pela cirurgia de catarata por microincisão nas córneas pós-LASIK foi significativo em comparação com olhos virgens (p=0,001, p=0,002 e p=0,018, respectivamente).
Conclusões: A cirurgia de catarata aumentou a inclinação das córneas em ambos os grupos, sendo esse aumento significativamente maior nos olhos pós-LASIK. Certamente, a topografia da córnea antes da cirurgia de catarata é particularmente útil para fornecer interpretações mais precisas do astigmatismo induzido cirurgicamente.
Keywords: Cirurgia de catarata; Ceratomileuse; excimer laser in situ; Cirurgia refrativa; Astigmatismo induzido cirurgicamente; Análise vetorial.
Arq. Bras. Oftalmol. 2025;88 (6 )
:1-8
| DOI: 10.5935/0004-2749.2025-0118
Abstract
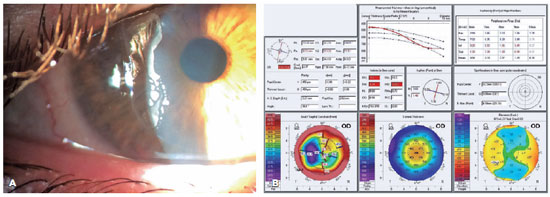
PURPOSE: Using advanced imaging techniques, this study aimed to evaluate corneal stability, epithelial remodeling, and tear film changes over a one-year period in first-time soft-contact lens wearers.
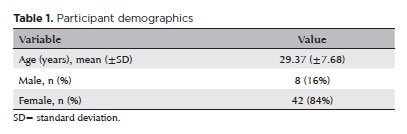
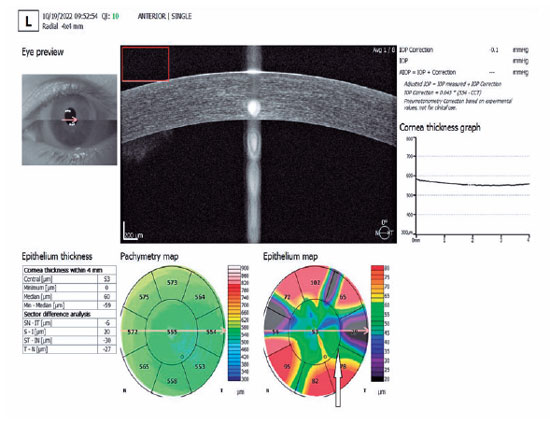
METHODS: A retrospective study was conducted on 100 eyes of 50 first-time daily soft-contact lens users aged 21–65 years with no prior rigid gas-permeable lens wear. The Sirius Scheimpflug imaging system was used to assess corneal topography, epithelial thickness, and non-invasive tear break-up time at baseline, 3, 6, and 12 months. Corneal warpage was evaluated using symmetry indices and Baiocchi Calossi Versaci indices. We performed statistical analysis using repeated-measures analyses of variance with Greenhouse-Geisser correction.
RESULTS: The mean baseline central corneal thickness was 537.83 (±7.92) µm, with no significant thinning after one year. The average simulated keratometry values remained stable, indicating no progressive corneal steepening or flattening. There were no significant changes in warpage indices over time, suggesting corneal shape preservation. Higher-order aberrations (coma, trefoil, and spherical aberrations) and non-invasive tear break-up time remained unchanged throughout the study period.
CONCLUSIONS: Modern silicone hydrogel soft-contact lenses do not induce significant corneal warpage, epithelial remodeling, or optical aberrations over a one-year period. We found that corneal morphology and tear film stability were preserved, supporting the safety of soft-contact lens use. These findings provide clinically relevant insights into the long-term impact of contact lens wear. They may facilitate improved lens fitting strategies and preoperative refractive surgery assessments.
Keywords: Contact lenses, hydrophilic; Cornea/surgery; Corneal diseases; Corneal topography; Adaptation, ocular/physiology; Endothelium, corneal/pathology; Refractive errors; Tears/metabolism.
Arq. Bras. Oftalmol. 2025;88 (2 )
:1-9
| DOI: 10.5935/0004-2749.2023-0292
Abstract
PURPOSE: Myopia, or nearsightedness, is one of the most common eye conditions worldwide. However, a comparison of the effectiveness of different laser-assisted interventions is lacking. Thus, we aimed to compare the efficacy and safety of LASIK and IntraLASIK in addressing myopia.
METHODS: The study was conducted in two ophthalmology clinics in Beijing, China, in 2022. A total of 84 patients (152 eyes) with different degrees of myopia were examined and underwent LASIK (n=46, 80 eyes) or IntraLASIK (n=38, 72 eyes). Keratometry, corneal topography, pachymetry, visual acuity evaluation, and corneal biomechanical analysis were performed before and after the intervention.
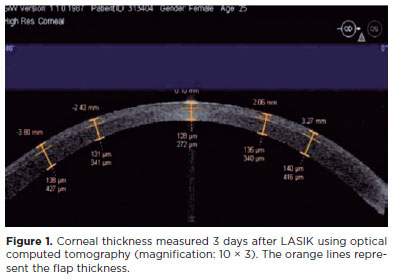
RESULTS: IntraLASIK produced more precise flaps than LASIK, with deviations of <8 mm and 0.1 mm from the intended thickness and diameter, respectively. LASIK resulted in nonuniform flaps, with thickness deviations of 5-86 mm. IntraLASIK demonstrated a superior efficacy for patients with severe myopia and thin corneas, with a mean spherical equivalent of 0.9 D at 6 months compared to the 1.4 D for LASIK. Approximately 91% and 83% of the patients with mild to moderate and severe myopia, respectively, achieved results within ± 0.49 D from the refractive target with IntraLASIK.
CONCLUSIONS: Corneal hysteresis and corneal resistance factor decreased with an increase in laser intensity, and they decreased faster with thinner corneas. Thus, IntraLASIK is more useful than LASIK in patients with thin corneas and severe myopia.
Keywords: Myopia; Lasers; Cornea; Keratomileusis; Laser in situ
Arq. Bras. Oftalmol. 2026;89 (3 )
:1-8
| DOI: 10.5935/0004-2749.2025-0330
Abstract
PURPOSE: To assess whether low-concentration brimonidine (0.025%) improves early postoperative signs and symptoms following femtosecond laser-assisted in situ keratomileusis and photorefractive keratectomy without affecting pupil diameter or flap safety.
METHODS: This prospective, randomized, double-masked, contralateral-eye, single-center study was conducted between January and September 2024. In each patient, one eye received 0.025% brimonidine 15–30 min before surgery (mean: 21.3 ± 2.4 min), whereas the fellow eye received 0.15% sodium hyaluronate (control). Primary outcomes on postoperative Day 1 included subconjunctival hemorrhage laser-assisted in situ keratomileusis and patient-reported symptoms (0–10 scale; composite score). Pupil diameter was measured pre-ablation. Statistical analyses included McNemar and paired t tests, with a significant threshold of α=0.05.
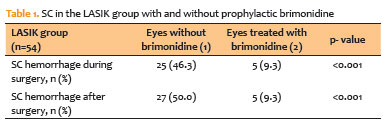
RESULTS: A total of 124 patients were included (54 laser-assisted in situ keratomileusis and 70 photorefractive keratectomy). Pupil diameter did not differ significantly between brimonidine-treated and control eyes (laser-assisted in situ keratomileusis: 2.63 ± 0.47 vs. 2.69 ± 0.42 mm, p=0.273; photorefractive keratectomy: 2.56 ± 0.44 vs. 2.61 ± 0.39 mm, p=0.116). In laser-assisted in situ keratomileusis, subconjunctival hemorrhage occurred less frequently in brimonidine-treated eyes both intraoperatively (9.3% vs. 46.3%, p<0.001) and on postoperative Day 1 (9.3% vs. 50.0%, p<0.001). Composite symptom scores were significantly lower in brimonidine-treated eyes in both laser-assisted in situ keratomileusis and photorefractive keratectomy groups (p=0.001 for both).
CONCLUSIONS: Preoperative administration of low-concentration brimonidine (0.025%) significantly reduced subconjunctival hemorrhage in laser-assisted in situ keratomileusis without comprising flap integrity. It also improved early postoperative symptoms in laser-assisted in situ keratomileusis and photorefractive keratectomy, without affecting pupil diameter. These findings support the use of dilute brimonidine as a safe and effective adjunct to enhance the immediate postoperative experience in refractive surgery.
Keywords: Brimonidine tartrate; Postoperative pain; Subconjunctival hemorrhage; Refractive surgery; Hemorrhage; Keratomileusis, laser in situ; Photorefractive keratectomy
Arq. Bras. Oftalmol. 2025;88 (5 )
:1-9
| DOI: 10.5935/0004-2749.2024-0326
Abstract
PURPOSE: This study was conducted to investigate the effect of injectable platelet-rich fibrin on the recovery of compromised epithelium due to crosslinking treatment.
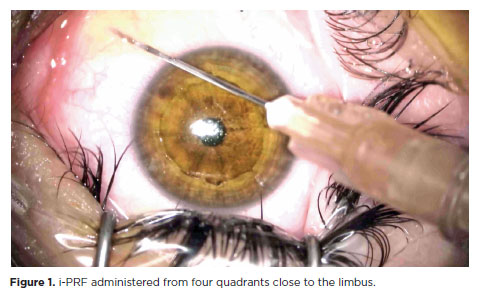
METHODS: In this comparative study, the epithelial closure rates and in vivo confocal biomicroscopy results of 26 patients with keratoconus who underwent subconjunctival injection of injectable platelet-rich fibrin near the limbus after epithelium-off corneal crosslinking treatment were compared with those of 25 patients who did not receive the injection of injectable platelet-rich fibrin.
RESULTS: The average time to epithelial defect closure in the injectable platelet-rich fibrin group was 2.76 ± 0.90 days compared to 3.56 ± 0.86 days in the non-injectable platelet-rich fibrin group (p=0.003). At the end of the 1st month, the mean subbasal nerve plexus density was 1.26 ± 1.61 nerves/mm2 in the injectable platelet-rich fibrin group, whereas it was 0.72 ± 0.89 nerves/mm2 in the non-injectable platelet-rich fibrin group (p=0.016). By the 3rd month, the density increased to 3.42 ± 1.13 nerves/mm2 in the injectable platelet-rich fibrin group and 2.36 ± 1.15 nerves/mm2 in the non-injectable platelet-rich fibrin group (p=0.002). Similarly, the anterior stromal keratocyte density at the end of the 1st month was 93.6 ± 33.5 cells/mm2 in the injectable platelet-rich fibrin group compared to 67.3 ± 26.4 cells/mm2 in the non-injectable platelet-rich fibrin group (p=0.001). By the end of the 3rd month, the density increased to 255.2 ± 45.7 cells/mm2 in the injectable platelet-rich fibrin group and 222.1 ± 43.6 cells/mm2 in the non-injectable platelet-rich fibrin group (p=0.011). In the non-injectable platelet-rich fibrin group, one patient developed a sterile infiltrate at the end of the 1st week, whereas no complications were observed in the injectable platelet-rich fibrin group.
CONCLUSION: Subconjunctival injectable platelet-rich fibrin application is an effective and safe method for corneal epithelial healing after crosslinking treatment.
Keywords: Keratoconus; Platelet-rich fibrin; Epithelium; corneal; Corneal crosslinking; Wound healing
Arq. Bras. Oftalmol. 2024;87 (3 )
:1-7
| DOI: 10.5935/0004-2749.2023-0049
Abstract
PURPOSE: To investigate the association of pre-photorefractive keratectomy Schirmer-1 test value with post-photorefractive keratectomy central corneal epithelial thickness, ocular surface disease index score, and uncorrected distance visual acuity.
METHODS: Patients were categorized according to preoperative Schirmer-1 value: the normal Schirmer Group (n=54; Schirmer-1 test value, >10 mm) and the low Schirmer Group (n=52; Schirmer-1 test value, between 6 and 10 mm). We analyzed ablation depth, visual acuity, result of Schirmer-1 test (with anesthesia), tear film break-up time, ocular surface disease index score, central corneal epithelial thickness, and spherical equivalent refraction.
RESULTS: We found significant differences between the groups in Schirmer-1 test value, tear film break-up time, and ocular surface disease index score, both preoperatively and postoperatively (p<0.001). The preoperative central corneal epithelial thicknesses of the two groups were similar (p>0.05). After photorefractive keratectomy, the Schirmer-1 test value and spherical equivalent refraction decreased in both groups (p<0.05), and ocular surface disease index scores and central corneal epithelial thickness values increased in the low Schirmer Group (p<0.001) but not in the normal Schirmer Group (p>0.05). The postoperative central corneal epithelial thicknesses of the low Schirmer Group were significantly higher than those of the normal Schirmer Group (p<0.001). Postoperative uncorrected distance visual acuity did not differ significantly between the two groups (p>0.05).
CONCLUSIONS: In patients with low Schirmer-1 test values before photorefractive keratectomy, the corneal epithelium thickened and ocular surface complaints increased during the postoperative period. However, changes in the corneal epithelium did not affect the postoperative uncorrected distance visual acuity. To reduce postoperative problems on the ocular surface in these patients, we recommend that dry eye be treated before photorefractive keratectomy.
Keywords: Epithelium, corneal; Cornea; Photorefractive keratectomy; Schirmer test; Visual acuity
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
08-fig01.jpg)
12-tab01tb.jpg)
11-fig01.jpg)
01-tab01tb.jpg)
04-fig01.jpg)
05-fig01tb.jpg)