Arq. Bras. Oftalmol. 2026; 89 (4): 10.5935/0004-2749.2025-0216
Total: 264
Ana Flavia Belfort1; Heloisa Andrade Maestrini2; Heloisa Helena Abil Russ Giacometti3; Aline Domingos Pinto Ruppert4; Emilio Rintaro Suzuki Junior5; Herika Danielle de Miranda Santos2; Alberto Basile Neto6; Clarice Freire Dayrell de Souza5,7; Marcos Balbino8; Marcelo Jordão Lopes da Silva9; Lunna Pires Moreira7; Regina Cele Silveira Seixas4
DOI: 10.5935/0004-2749.2025-0216
ABSTRACT
PURPOSE: To compare the efficacy and safety of trabeculectomy with mitomycin C, performed with versus without adjunctive Ologen collagen matrix in a multicenter real-world setting.
METHODS: This multicenter retrospective comparative study included 277 patients (365 eyes) who underwent trabeculectomy with mitomycin C, with or without Ologen, between 2017 and 2022 across five Brazilian centers. Extracted data comprised demographic characteristics, glaucoma subtype, intraocular pressure, number of glaucoma medications, postoperative interventions, complications, and additional surgical procedures. Surgical success was defined using two criteria: (1) intraocular pressure ≤21mmHg with ≥20% reduction from baseline and (2) final intraocular pressure between 6 and 21mmHg. Outcomes were categorized as complete (without medications) or qualified (with medications).
RESULTS: Both groups achieved substantial reductions in intraocular pressure and medication burden at 12 months, with high rates of complete and qualified success under both definitions. The Ologen group required fewer suture lysis procedures (49.0% vs. 60.8%; p=0.025), suggesting a modulatory effect on early postoperative fibrosis. Rates of other postoperative interventions, complications, and additional glaucoma surgeries were comparable between groups. Kaplan–Meier analysis demonstrated no significant difference in cumulative success over time.
CONCLUSION: Trabeculectomy with mitomycin C is effective and safe regardless of adjunctive Ologen use. Although Ologen did not confer superior long-term efficacy, its association with reduced suture lysis suggests a potential role in modulating early wound healing.
Keywords: Trabeculectomy, Intraocular pressure, Mitomycin C; Wound healing; Sutures
INTRODUCTION
Glaucoma is a chronic, progressive optic neuropathy and the leading cause of irreversible blindness worldwide(1). Its global prevalence is projected to reach 111.8 million by 2040(1). Elevated intraocular pressure (IOP) remains the most important modifiable risk factor(2), and its reduction is the only intervention proven to delay disease progression. Management strategies include pharmacologic therapy, laser procedures, and surgical intervention.
Trabeculectomy, first described by Cairns in 1968, remains the reference standard for surgical management of advanced glaucoma. However, long-term success is frequently limited by subconjunctival fibrosis, resulting in bleb failure(3). The intraoperative use of antimetabolites, particularly mitomycin C (MMC), enhances surgical success by suppressing fibroblast proliferation. Nevertheless, MMC is associated with sight-threatening complications, including thin avascular blebs, hypotony, and late-onset bleb-related infections(4). These limitations have prompted exploration of alternative strategies for modulating wound healing.
Ologen is a biodegradable collagen-glycosaminoglycan scaffold designed to promote physiological wound healing. By facilitating randomized fibroblast growth and organized extracellular matrix deposition, it aims to reduce scarring and support the formation of diffuse, functional blebs(5,6). However, evidence regarding its clinical benefit remains inconsistent. Some studies and meta-analyses report reduced postoperative interventions and improved bleb morphology, whereas others demonstrate no significant advantage in long-term IOP control compared with conventional approaches(7-12).
Although Ologen was available in Brazil during the study period, it has since been discontinued locally, while remaining accessible in other regions, including parts of Asia and Europe. Therefore, evaluating its real-world performance remains relevant for informing clinical practice and guiding the development of next-generation biomaterials.
In this context, the present study aimed to compare the real-world outcomes of trabeculectomy with MMC performed with and without adjunctive Ologen, focusing on IOP reduction, medication burden, safety profile, and postoperative management requirements.
METHODS
Study design
This multicenter retrospective cohort study was based on a review of medical records from patients who underwent trabeculectomy with mitomycin C (MMC), with or without adjunctive Ologen, between 2017 and 2022 at five glaucoma referral centers in Brazil. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, and a completed STROBE checklist is provided as a supplementary file.
Surgical procedure
Patients were allocated to treatment groups according to surgeon preference, availability of the Ologen implant, and individual clinical characteristics. As such, group allocation was non-randomized and reflective of real-world clinical practice.
All procedures were performed using a fornix-based conjunctival approach with a standard rectangular scleral flap. MMC was applied beneath the scleral flap and conjunctiva for 1-3 min, followed by copious irrigation. In the Ologen group, the implant was placed in the subconjunctival space prior to final closure.
Postoperative management included topical corticosteroids and antibiotics, tapered according to clinical response. Additional interventions — such as bleb massage, laser suture lysis, and needling — were performed as clinically indicated based on bleb morphology and IOP.
Selection criteria and data collection
Eligible participants were adults with primary open-angle glaucoma requiring filtering surgery. Exclusion criteria included prior glaucoma filtering procedures (trabeculectomy, glaucoma drainage devices, or minimally invasive glaucoma surgery), incomplete medical records, and follow-up shorter than 12 months. Both eyes from the same patient were included if they met the eligibility criteria.
Collected variables included demographic characteristics, glaucoma subtype, preoperative and postoperative IOP, number of glaucoma medications, postoperative complications, need for additional interventions, and requirement for further glaucoma surgery. Postoperative interventions were systematically recorded. No imputation was performed for missing data, and eyes lacking complete 12-month follow-up were excluded from outcome analysis.
Outcome measures and success criteria
A formal sample size calculation was not performed due to the retrospective study design. The primary outcomes were IOP reduction and surgical success.
Surgical success was defined using two criteria: (1) IOP ≤21mmHg with a ≥20% reduction from baseline and (2) final IOP between 6 and 21mmHg. Success was categorized as complete (without medications) or qualified (with medications). Failure was defined as the need for additional glaucoma surgery, loss of light perception, or persistently uncontrolled IOP.
Statistical analysis
Data distribution was assessed using skewness and kurtosis tests. Depending on the distribution, parametric or non-parametric tests were applied. Continuous variables are presented as mean ± standard deviation, whereas categorical variables are expressed as frequencies and percentages and compared using the chi-square or Fisher's exact test, as appropriate.
Because some patients contributed both eyes, a prespecified assessment was conducted to evaluate potential intra-patient correlation. The proportion of unilateral versus bilateral cases was compared between groups. In the absence of a significant imbalance, all eligible eyes were included in the analysis.
Kaplan-Meier survival curves were generated based on predefined success criteria, and Cox proportional hazards regression models were used to evaluate surgical outcomes. Statistical significance was defined as p<0.05. All analyses were performed using Stata software.
Ethics
The study protocol was approved by the Institutional Review Board of HCLOEOftalmologia Especializada (São Paulo, Brazil). Given the retrospective design and use of anonymized data, the requirement for informed consent was waived in accordance with institutional policy and national regulations. The study was conducted in compliance with the principles of the Declaration of Helsinki across all participating centers.
RESULTS
Of 449 screened eyes, 365 eyes from 277 patients met the inclusion criteria. Among these, 212 eyes underwent trabeculectomy with MMC alone, and 153 eyes underwent trabeculectomy with MMC plus Ologen. The proportion of unilateral and bilateral cases did not differ significantly between groups (chi-square test, p=0.34); therefore, all eligible eyes were included in the analysis. Baseline characteristics — including age, sex, glaucoma severity, baseline IOP, and number of preoperative medications — were comparable between groups (Table 1). Most patients had advanced glaucoma and required multiple medications preoperatively.
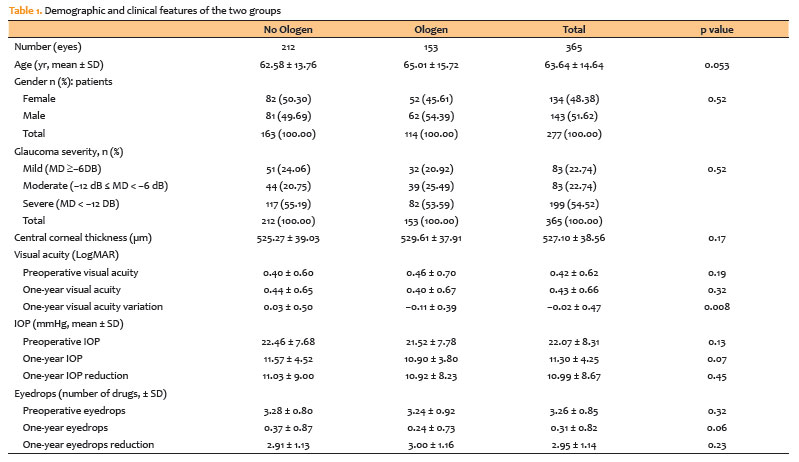
At 12 months, mean IOP decreased from 22.46 ± 7.68 to 11.57 ± 4.52mmHg in the MMC group and from 21.52 ± 7.78 to 10.9 ± 3.8mmHg in the MMC plus Ologen group (p=0.45; 95% CI, −1.2 to 2.8mmHg). Both groups also demonstrated substantial reductions in medication burden. Changes in visual acuity were minimal and comparable between groups (Table 1).
Surgical success rates were similar between groups under both predefined criteria. For criterion 1 (IOP ≤21mmHg with ≥20% reduction), complete success was achieved in 69.8% of eyes in the MMC group and 78.4% in the MMC plus Ologen group (p=0.42; 95% CI, −5.3 to 22.3), whereas qualified success was observed in 81.6% and 85.6% of eyes, respectively (p=0.31; 95% CI, −4.1 to 11.9).
Using criterion 2 (IOP >6 mmHg ≤21 mmHg), complete success rates were 75.0% in the MMC group and 81.1% in the MMC plus Ologen group (p=0.95; 95% CI, −8.4 to 16.2), while qualified success rates were 91.8% and 91.7%, respectively (p=0.87; 95% CI, −6.0 to 5.0; Table 3).
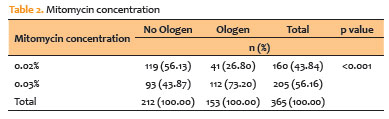
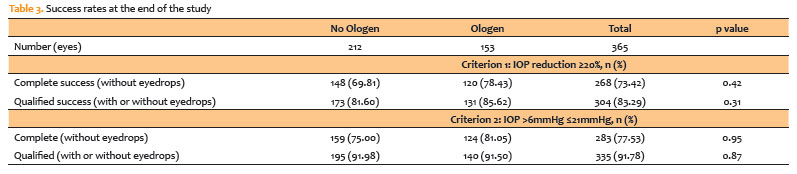
Figure 1 shows longitudinal changes in IOP and medication use. Kaplan-Meier survival analysis (Figure 2) demonstrated comparable cumulative success probabilities between groups over time. Although a slight early advantage was observed in the Ologen group, this difference was not sustained during follow-up.
Postoperative suture lysis was performed more frequently in the MMC group than in the MMC plus Ologen group (60.8% vs. 49.0%; p=0.025; 95% CI, 1.7-22.3). No other significant differences were observed in postoperative interventions. Rates of needling and bleb massage were similar between groups (Table 4).

The overall incidence of complications — including hypotony, shallow anterior chamber, and choroidal detachment — was low and did not differ significantly between groups (Table 5).

Additional glaucoma surgery was required in a small proportion of eyes, with comparable rates between groups (Table 6). Secondary procedures included repeat trabeculectomy, implantation of glaucoma drainage devices, and cyclophotocoagulation, reflecting standard management approaches for surgical failure in advanced glaucoma.

DISCUSSION
In this retrospective multicenter study, trabeculectomy augmented with MMC, with or without the addition of the Ologen® collagen matrix, resulted in significant reductions in IOP and decreased dependence on glaucoma medications over a 12-month follow-up, with comparable safety profiles between groups. These findings are consistent with those of previous comparative studies evaluating Ologen as an adjunct to trabeculectomy, which generally report similar IOP-lowering efficacy across techniques(2,7,8,10).
The Ologen® collagen matrix was developed to modulate subconjunctival wound healing by reducing excessive fibrosis and potentially improving long-term trabeculectomy outcomes(5-7). In this study, the addition of Ologen did not confer a statistically significant advantage in terms of reductions in IOP or medication use at 1 year. The Kaplan-Meier survival analysis (Figure 2) demonstrated that the probability of surgical success over time was comparable between the two groups, with the survival curves remaining closely aligned during follow-up. The slightly higher success probability observed in the Ologen Group at early time points may suggest a short-term benefit in maintaining target IOP, which is consistent with the reduced need for suture lysis. However, this difference was not statistically significant, reinforcing that Ologen does not appear to improve long-term surgical success when used with MMC. These results are consistent with previous reports that failed to demonstrate superior long-term pressure control with Ologen(9,10) and are supported by a meta-analysis showing comparable IOP reduction, surgical success rates, and adverse event profiles between trabeculectomy with Ologen® and trabeculectomy with MMC alone(11).
The only statistically significant difference observed was a lower need for suture lysis in the Ologen group. This finding may reflect a milder early scarring response associated with the implant's modulation of wound healing modulation, potentially resulting in a less fibrotic bleb and fewer postoperative manipulations(8,10). However, this result should be interpreted cautiously. An imbalance in MMC concentration was observed between the groups, with 0.03% MMC more frequently used in the Ologen® Group and 0.02% in the control group. Previous studies have shown that higher MMC concentrations may be associated with increased bleb diffusion and reduced postoperative fibrosis, which could independently decrease the need for suture lysis(6). Given the retrospective design and sample size, both subgroup and multivariate analyses were limited in scope, thereby preventing definitive conclusions regarding the independent contribution of Ologen® to this outcome.
Few large, multicenter retrospective studies have evaluated the role of Ologen in trabeculectomy(9-11). Differences in published outcomes may be attributed to variations in surgical technique, postoperative management, and patient-related factors influencing wound healing(9). Papaconstantinou et al. reported improved bleb architecture over time following Ologen use(5), whereas other studies have yielded mixed results(7,12). While Ji et al. found no significant differences in outcomes, Cillino et al. reported a trend toward higher complete success rates with Ologen, although this difference did not reach statistical significance(7,9). Such discrepancies underscore the need to better define the clinical scenarios in which Ologen® may be most beneficial.
This study has several strengths, including its multicenter design, relatively large sample size, and inclusion of well-matched groups, which enhance external validity and improve generalizability to real-world practice. Nonetheless, limitations must be acknowledged. The retrospective, non-randomized design introduces potential selection bias because the decision to use Ologen® was based on surgeon discretion, implant availability, and case characteristics. The criteria used for defining surgical success partially followed World Glaucoma Association recommendations. While a lower IOP limit of 6mmHg and distinctions between complete and qualified success were applied, only a single upper IOP threshold (21mmHg) was used. Using multiple upper thresholds (e.g., ≤18 or ≤15mmHg) could enhance the comparability across studies. Moreover, a detailed bleb morphology assessment was not performed, and Ologen is currently not commercially available in Brazil, limiting the local applicability of the findings. Furthermore, the limited follow-up limits the robust assessment of late complications, such as bleb failure, blebitis, or infection, which, although uncommon, are clinically relevant outcomes. Despite these limitations, this series represents one of the larger multicenter cohorts comparing trabeculectomy with and without Ologen using survival analysis to evaluate surgical success. The findings contribute to the existing body of evidence by reinforcing that, in real-world settings, the addition of Ologen to MMC-augmented trabeculectomy does not improve long-term efficacy, while it may affect early postoperative management.
In conclusion, trabeculectomy with MMC, performed with or without the addition of the Ologen® collagen matrix, resulted in a significant and sustained reduction in IOP and a substantial decrease in the use of glaucoma medications after 1 year of follow-up. Rates of complete and qualified success were high and similar between the groups, confirming the effectiveness of trabeculectomy with MMC in advanced glaucoma.
The only significant difference observed was a lower frequency of suture lysis in the Ologen group, suggesting a potential effect on early postoperative wound healing and bleb modulation. Although Ologen did not show superior long-term efficacy, its association with fewer postoperative manipulations may be clinically relevant in selected clinical cases.
These findings, derived from a large multicenter real-world cohort, add to the existing evidence regarding the role of Ologen as an adjunct in trabeculectomy. Future prospective randomized studies with longer follow-up and standardized assessment of bleb morphology will be required to better define its clinical utility and identify patient subsets that may benefit from its use.
ACKNOWLEDGEMENTS
The authors would like to thank Regina Cele Silveira Seixas for her leadership and commitment to research quality and excellence, which were instrumental to the completion of this study.
AUTHORS' CONTRIBUTIONS:
Significant contribution to conception and design: Ana Flavia Belfort, Heloisa Andrade Maestrini, Emilio Rintaro Suzuki Junior, Clarice Freire Dayrell de Souza, Marcos Balbino, Marcelo Jordão Lopes da Silva, Regina Cele Silveira Seixas.
Data acquisition: Ana Flavia Belfort, Heloisa Andrade Maestrini, Heloisa Helena Abil Russ Giacometti, Aline Domingos Pinto Ruppert, Emilio Rintaro Suzuki Junior, Herika Danielle de Miranda Santos, Alberto Basile Neto, Clarice Freire Dayrell de Souza, Marcelo Jordão Lopes da Silva, Lunna Pires Moreira, Regina Cele Silveira Seixas.
Data analysis and interpretation: Ana Flavia Belfort, Heloisa Andrade Maestrini, Heloisa Helena Abil Russ Giacometti, Aline Domingos Pinto Ruppert, Emilio Rintaro Suzuki Junior, Clarice Freire Dayrell de Souza, Lunna Pires Moreira, Regina Cele Silveira Seixas.
Manuscript drafting: Ana Flavia Belfort, Heloisa Andrade Maestrini, Alberto Basile Neto, Marcos Balbino, Marcelo Jordão Lopes da Silva, Lunna Pires Moreira, Regina Cele Silveira Seixas.
Significant intellectual content revision of the manuscript: Ana Flavia Belfort, Heloisa Andrade Maestrini, Heloisa Helena Abil Russ Giacometti, Emilio Rintaro Suzuki Junior, Marcos Balbino, Regina Cele Silveira Seixas.
Final approval of the submitted manuscript: Ana Flavia Belfort, Heloisa Andrade Maestrini, Heloisa Helena Abil Russ Giacometti, Aline Domingos Pinto Ruppert, Emilio Rintaro Suzuki Junior, Herika Danielle de Miranda Santos, Alberto Basile Neto, Clarice Freire Dayrell de Souza, Marcos Balbino, Marcelo Jordão Lopes da Silva, Lunna Pires Moreira, Regina Cele Silveira Seixas.
Statistical analysis: Heloisa Andrade Maestrini, Marcos Balbino, Regina Cele Silveira Seixas.
Obtaining funding: not applicable.
Administrative, technical, or material support supervision: Marcos Balbino, Regina Cele Silveira Seixas.
Research group leadership: Regina Cele Silveira Seixas.
REFERENCES
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081-90.
2. Sharma AK, Gupta P, Sharma HR. Outcome of trabeculectomy with collagen matrix implant versus mitomycin c in primary glaucoma: a comparative study. Int J Appl Basic Med Res. 2021;11(2):80-4.
3. Cairns JE. Trabeculectomy. Preliminary report of a new method. Am J Ophthalmol. 1968;66(4):673-9.
4. Azuara-Blanco A, Katz LJ. Dysfunctional filtering blebs. Surv Ophthalmol. 1998;43(2):93-126.
5. Papaconstantinou D, Georgalas I, Karmiris E, Diagourtas A, Koutsandrea C, Ladas I, et al. Trabeculectomy with Ologen versus trabeculectomy for the treatment of glaucoma: a pilot study. Acta Ophthalmol. 2010;88(1):80-5.
6. Eldaly ZH, Maasoud AA, Saad MS, Mohamed AA. Comparison between Ologen implant and different concentrations of Mitomycin C as an adjuvant to trabeculectomy surgery. Oman J Ophthalmol. 2017;10(3):184-92.
7. Cillino S, Casuccio A, Di Pace F, Cagini C, Ferraro LL, Cillino G. Biodegradable collagen matrix implant versus mitomycin-C in trabeculectomy: five-year follow-up. BMC Ophthalmol. 2016;16(1):24.
8. Yuan F, Li L, Chen X, Yan X, Wang L. Biodegradable 3D-Porous Collagen Matrix (Ologen) Compared with Mitomycin C for Treatment of Primary Open-Angle Glaucoma: Results at 5 Years. J Ophthalmol. 2015;2015:637537.
9. Ji Q, Qi B, Liu L, Guo X, Zhong J. Efficacy and Safety of Ologen Implant Versus Mitomycin C in Primary Trabeculectomy: A Meta-analysis of Randomized Clinical Trials. J Glaucoma. 2015;25(5):e88-94.
10. Song DS, Qian J, Chen ZJ. Ologen implant versus mitomycin-C for trabeculectomy: A meta-analysis. Medicine (Baltimore). 2019;98(25):e16094.
11. He M, Wang W, Zhang X, Huang W. Ologen implant versus mitomycin C for trabeculectomy: a systematic review and meta-analysis. PLoS One. 2014;9(1):e85782.
12. Rosentreter A, Schild A, Jordan J, Krieglstein GK, Dietlein TS. A prospective trial of trabeculectomy using mitomycin C vs an ologen implant in open angle glaucoma. Eye (Lond). 2010;24(9):1449-57.
Submitted for publication:
September 18, 2025.
Accepted for publication:
March 26, 2026.
Data Availability Statement: The data underlying this study are not publicly available because they were derived from patient medical records and are subject to privacy restrictions. De-identified data may be shared with qualified researchers upon reasonable request.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Jayter de Paula
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.