Abstract
Objetivo: Apresentar nossos resultados de longo período de vitrectomia pars plana combinada com fotocoagulação panretiniana com endolaser, implantação da válvula Ahmed para glaucoma e/ou facoemulsificação em pacientes com glaucoma neovascular complicado. Métodos: Foram incluídos no estudo 15 olhos de 15 pacientes com glaucoma neovascular como complicação da retinopatia diabética e devido à oclusão isquêmica da veia central da retina. Todos os casos tiveram hemorragia vítrea. Além disso, 8 dos casos apresentaram diferentes graus de hifema. A injeção intravítrea de bevacizumabe foi administrada em todos os casos 3 dias antes da cirurgia. Facoemulsificação, vitrectomia pars plana e implantação da válvula Ahmed para glaucoma foram realizadas em 12 pacientes fáquicos. A vitrectomia pars plana e a implantação da válvula Ahmed para glaucoma foram realizadas em 3 pacientes pseudofáquicos. Complicações perioperatórias e pós-operatórias, valores de pressão intraocular e valores de melhor acuidade visual corrigida pré-operatório e pós-operatório foram registrados.
Resultados: O acompanhamento médio foi de 24,4 ± 14,56 meses. A média da pressão intraocular pré-operatória foi de 50,06 ± 7,6 mmHg. Em 1 dia, 7 dias e 1,3,6,12 meses, e última visita após cirurgia, a média da pressão intraocular foi de 11,06 ± 8,22, 12,66 ± 7,27, 13,8 ± 7,73, 18,64 ± 7,05, 19,28 ± 4,61, 16,28 ± 1,68 e 16,92 ± 2,12 mmHg, respectivamente (p=0,001 para cada visita de acompanhamento). A média da acuidade visual na última visita foi de 1,18 ± 0,42 logMar (p=0,001 para cada visita de acompanhamento). Vários graus de reações de hifema e fibrina foram registrados como complicações precoces pós-operatórias. Phthisis bulbi foi desenvolvido em um caso durante o acompanhamento. A cirurgia de revisão da válvula Ahmed para glaucoma foi necessária em 4 casos.
Conclusões: Os procedimentos cirúrgicos combinados que realizamos são seguros, eficazes e preferenciais, tanto em termos de controle da alta pressão intraocular quanto fornecimento de habilidades visuais razoáveis em pacientes com glaucoma neovascular complicado.
Keywords: Glaucoma neovascular/complicações; Vitrectomia; Implantes para drenagem de glaucoma; Facoemulsificação
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
03-tab01.jpg)
11-tab01tb.jpg)
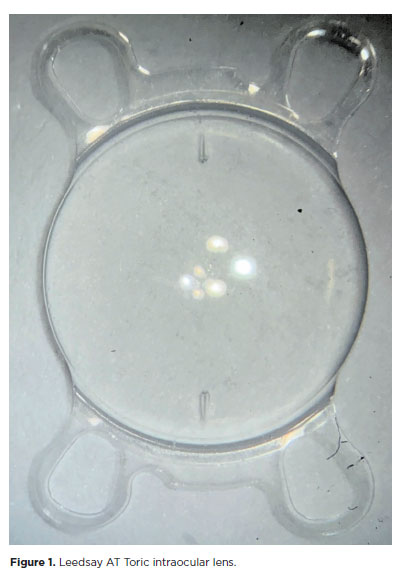
11-fig01.jpg)
09-tab01tb.jpg)