Arq. Bras. Oftalmol. 2026; 89 (3): 10.5935/0004-2749.2025-0332
Total: 347
Carolina Pereira Bigheti1; Roberta Lilian Fernandes de Sousa1; Simone Milani Brandão1; Carlos Roberto Padovani2; Silvana Artioli Schellini1
DOI: 10.5935/0004-2749.2025-0332
ABSTRACT
PURPOSE: To quantitatively compare eyebrow and eyelid positions in anophthalmic sockets reconstructed with conical or spherical orbital implants combined with customized external ocular prostheses.
METHODS: This cross-sectional observational study included 38 patients with unilateral anophthalmic sockets, of whom 21 received conical implants, and 17 received spherical implants. Eyelid and eyebrow parameters—including margin reflex distance 1 and 2, vertical and horizontal palpebral fissure dimensions, eyebrow-to-upper-eyelid margin distance in primary gaze and infraduction, medial and lateral eyelid angles in primary gaze, and superior eyelid sulcus depth —were quantitatively assessed using standardized digital photographs analyzed with Image J software. The contralateral healthy eye served as the control. Statistical analyses were performed to compare measurements between groups.
RESULTS: In the primary gaze position, conical and spherical implants showed comparable margin-reflex distance1, margin-reflex distance2, vertical palpebral fissure height, eyelid margin position, and medial and lateral eyelid angles. During infraduction, the upper eyelid margin was significantly lower in sockets reconstructed with conical implants. Compared with contralateral normal eyes, anophthalmic sockets exhibited a reduced horizontal palpebral fissure and a deeper superior eyelid sulcus, irrespective of implant shape.
CONCLUSION: Anophthalmic sockets reconstructed with conical or spherical implants demonstrate similar eyebrow and eyelid positioning in primary gaze. However, conical implants are associated with a lower eyelid margin during infraduction. Independent of implant format, anophthalmic sockets show a narrower horizontal palpebral fissure and increased superior sulcus depth compared with normal eyes.
Keywords: Anophthalmos; Prosthesis implantation; Anophthalmic socket; Conical implants; Spherical implants; Orbital implants; Eyelid measurements
INTRODUCTION
The orbital and periorbital tissues play a fundamental role in maintaining the anatomical and functional stability of the globe within the orbit(1,2). Following enucleation or evisceration, orbital volume is reduced, and residual tissues undergo structural rearrangement, leading to characteristic morphological changes within the anophthalmic socket. These changes may result in the development of anophthalmic socket syndrome, which is clinically characterized by enophthalmos, upper eyelid ptosis, deepening of the superior sulcus, and lower eyelid laxity or ectropion. These manifestations may occur in isolation or in combination and vary in severity(2,3).
Reconstruction of anophthalmic socket syndrome is optimally achieved through a multidisciplinary "team approach", in which the surgeon restores lost orbital volume using an orbital implant, while a prosthetist fabricates a customized external ocular prosthesis to reestablish facial symmetry and aesthetic appearance(3,4). Most orbital implants currently used for volume replacement in anophthalmic sockets are spherical(5). Conical implants, however, have been proposed as a more anatomically efficient alternative, as they are designed to occupy the intraconal space more effectively, potentially reducing superior sulcus deformity and improving eyelid position(6,7). Despite these theoretical advantages, quantitative evidence evaluating eyebrow and eyelid positioning following orbital reconstruction with spherical versus conical implants combined with customized external ocular prostheses remains lacking.
Therefore, the present study aimed to assess the influence of conical and spherical orbital implants, in association with customized external ocular prostheses, on eyelid and eyebrow position in patients with unilateral anophthalmic sockets.
METHODS
This study was conducted in accordance with the tenets of the Declaration of Helsinki and was approved by the local Research Ethics Committee. Written informed consent was obtained from all participants.
A prospective, observational, cross-sectional study was performed to compare eyebrow and eyelid positions in 38 patients with unilateral anophthalmic sockets reconstructed using spherical or conical orbital implants and fitted with a customized external ocular prosthesis. The contralateral normal eye served as the control. Sample size calculation for each group assumed a 10% loss of participants.
Inclusion criteria
Patients aged ≥10 yr who underwent unilateral evisceration for a blind and painful eye, presented with anophthalmic sockets type 0 or 1(8), and received primary reconstruction with either a conical or spherical orbital implant were included.
Exclusion criteria
Patients with anophthalmic sockets type 2 to 5(8), those with associated conditions such as orbital fractures or infectious processes, or those who had undergone more than one orbital surgery were excluded.
Surgical evisceration technique and implants
Evisceration was performed by two ophthalmologists using the same standardized technique, which included corneal removal, curettage of the intraocular contents, and immediate placement of the orbital implant. Twenty-one patients received a conical biosilicate implant (Biosilicate®, LAMAV Laboratories, São Carlos, Brazil), and 17 received a spherical polymethylmethacrylate (PMMA) implant (Solótica Industry and Commerce, São Paulo, Brazil). Implant format was assigned by lot, and implant size was determined intraoperatively using a sizer according to orbital volume.
Two sizes of conical implants were used: large (18 mm length; anterior and posterior diameters of 12 and 4 mm, respectively) and small (16 mm length; anterior and posterior diameters of 10 and 3 mm, respectively)(9). Spherical implants ranged from 16 to 20 mm in diameter. One month postoperatively, all patients were fitted with a customized external ocular prosthesis fabricated by the same ocularist. Clinical follow-up was conducted by the first author.
Parameters analyzed
Six months after surgery, with the customized external ocular prosthesis in place, the following measurements were obtained:
Margin-reflex distance (MRD): Distance from the upper (MRD1; Figure 1A) and lower (MRD2; Figure 1B) eyelid margins to the pupillary reflex or the center of the prosthesis pupil.
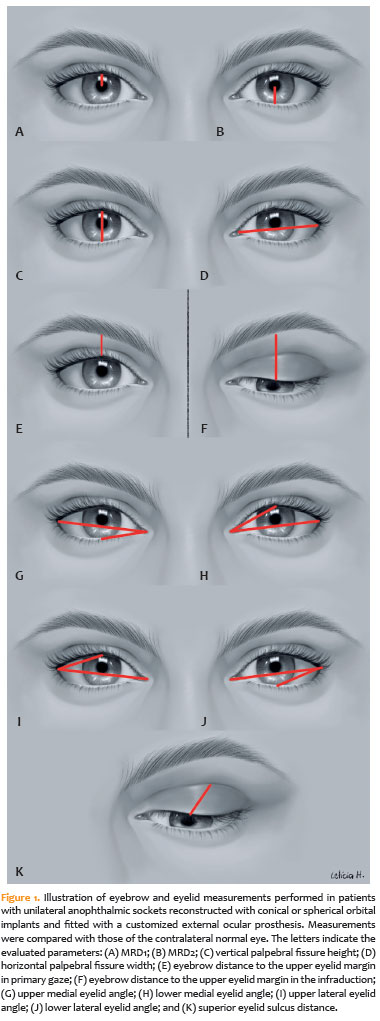
Vertical palpebral fissure height: Distance between the upper and lower eyelid margins through the pupil (Figure 1C).
Horizontal palpebral fissure width: Distance between the medial and lateral canthi (Figure 1D).
Eyebrow distance to the upper eyelid margin (EDM): Measured in primary gaze (Figure 1E) and infraduction (Figure 1F) along a vertical line from the upper eyelid margin above the pupil to the inferior margin of the eyebrow.
Medial and lateral eyelid angles: The palpebral fissure was divided into upper and lower portions using a line connecting the medial and lateral canthi. The angles formed between this line and the superior or inferior eyelid margins defined the medial upper and lower eyelid angles (Figure 1G,H) and the lateral upper and lower eyelid angles (Figure 1I,J).
Superior eyelid margin-to-superior eyelid sulcus distance: Measured along a 45° line from the upper eyelid margin immediately above the pupil to the superior eyelid sulcus (Figure 1K).
Photographic documentation
Standardized photographs were obtained using a Nikon Coolpix E5000 camera (Nikon Corp., Japan). Patients were positioned using a slit-lamp chin and forehead rest to ensure head stabilization. They were instructed to fixate on predefined targets in primary gaze and downgaze. The pupillary reflex was used as a reference, and a surgical marking pen was applied to mark the corresponding pupillary position on the external ocular prosthesis.
Quantitative analysis
All images were transferred to a desktop computer. Measurements were obtained in millimeters and angles in degrees by the first author using ImageJ software (version 1.51K; National Institutes of Health, USA).
Statistical analysis
Data were entered into Microsoft Excel and analyzed using STATA 14.0 (StataCorp LP, College Station, Texas). Descriptive statistics were calculated, and results were presented as frequencies. Differences in eyebrow and eyelid positions were assessed using the Kruskal–Walli's test followed by Dunn's post hoc analysis. A p-value ≤0.05 was considered statistically significant.
RESULTS
This study included 21 patients with unilateral anophthalmic sockets reconstructed using conical implants (mean age, 50.85 ± 19.18 yr; 66.6% male) and 17 patients reconstructed with spherical implants (mean age, 54.88 ± 19.80 yr; 62.5% male). Among patients with conical implants, 13 patients (61.9%) received small implants, seven (33.33%) received large implants, and implant size information was unavailable for one patient (4.7%). Among those with spherical implants, implant diameters were 16 mm in two patients (11.76%), 17 mm in two (11.76%), 18 mm in six (35.29%), and 20 mm in one (5.8%), while implant size data were missing for six patients (35.29%).
Clinical examination revealed no postoperative complications in any anophthalmic socket. There were not cases of conjunctival dehiscence or implant exposure, and all patients exhibited a normal amount of mucous secretion.
In primary gaze, anophthalmic sockets reconstructed with conical or spherical implants as well as the contralateral normal eyes, showed comparable MRD1 (p=0.4486), MRD2 (p=0.6381), vertical palpebral fissure height (p=0.1871), and EDM in primary gaze (p=0.3283; Table 1).
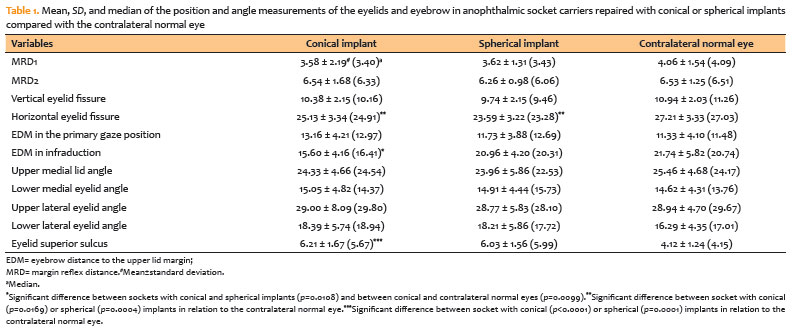
In contrast, statistically significant differences were observed for horizontal palpebral fissure width (p=0.0021), EDM in infraduction (p=0.0166), and superior eyelid sulcus depth in primary gaze (p=0.0001). The conical implant group demonstrated a shorter EDM in infraduction compared with the spherical implant group (p=0.0108) and the contralateral normal eye (p=0.0099). No significant difference was observed between spherical implants and the contralateral normal eye (p=0.3735; Table 1).
Both conical (p=0.0169) and spherical implants (p=0.0004) were associated with a smaller horizontal palpebral fissure compared with the contralateral normal eye, with no significant difference between the two implant formats (p=0.1109; Table 1). Similarly, sockets reconstructed with conical (p<0.0001) or spherical (p=0.0001), implants exhibited a deeper superior eyelid sulcus than the contralateral normal eye, without a significant difference between implant formats (p=0.4091; Table 1).
No statistically significant differences were found between either implant group and the contralateral normal eye with respect to medial upper (p=0.3763) or lower (p=0.9383) eyelid angles, or lateral upper (p=0.9952) or lower (p=0.3796) eyelid angles (Table 1).
DISCUSSION
In this study, orbital implant shape—conical or spherical—did not influence eyebrow or eyelid positions in primary gaze. However, anophthalmic sockets reconstructed with conical implants exhibited a shorter EDM in infraduction compared with sockets reconstructed with spherical implants and the contralateral normal eye, whereas the latter two showed no difference. Both implant types were associated with a reduced horizontal palpebral fissure width and a deeper superior eyelid sulcus compared with the contralateral normal eye.
Despite restoration of orbital volume and the use of a customized external ocular prosthesis, eyelid position abnormalities remain common in anophthalmic socket carriers. These include upper eyelid ptosis, deep superior sulcus, and lower eyelid laxity, often resulting from persistent volume deficiency, heavy or thick prostheses, shallow or contracted fornices, and poor prosthetic fit, which may compromise prosthesis retention and cosmesis(2,10).
To the best of our knowledge, this is the first study to quantitatively evaluate eyebrow and eyelid positions in patients with unilateral anophthalmic sockets reconstructed with conical versus spherical implants. Although spherical implants are widely used,(5) some authors have suggested that conical implants provide superior eyelid support and improved eyelid positioning6. The findings of the present study do not support this hypothesis.
To minimize bias, the surgical technique, photographic documentation, and quantitative assessment of eyebrow and eyelid positions were standardized. Although eyebrow position can be influenced by factors such as age, sex, ethnicity, cultural practices, fashion trends, and cosmetic interventions (e.g., eyebrow shaving or tattooing), the use of the contralateral normal eye as an internal control helped reduce these confounding effects.
All patients were fitted with customized external ocular prostheses, which are preferred over prefabricated prostheses due to improved adaptation, better symmetry with the natural eye, and superior cosmetic outcomes(11).
According to our quantitative measurements, MRD1, MRD2, vertical palpebral fissure height, and EDM in primary gaze were not influenced by orbital implant shape. However, in infraduction, sockets reconstructed with conical implants demonstrated a shorter EDM compared with those repaired with spherical implants and the contralateral normal eye. This finding may reflect an effect of the conical implant on upper eyelid descent during downgaze, producing a phenomenon similar to lid lag or Von Graefe's sign, which is characterized by the appearance of visible sclera between the upper eyelid margin and the corneal limbus during downward gaze. This effect may be related to the influence of the conical implant on the levator palpebrae superioris–superior rectus muscle complex, which is typically displaced inferiorly in anophthalmic sockets, resulting in rotational displacement of the orbital contents(1).
The horizontal palpebral fissure width in sockets reconstructed with conical or spherical implants was similar to and smaller than that of the contralateral normal eye. Reduction in horizontal palpebral fissure width following enucleation or evisceration is likely associated with the rearrangement of residual orbital structures or the medialization of the retinaculum and lateral rectus muscle due to decreased orbital volume, leading to medial displacement of the lateral canthus. Additionally, interposition of the external ocular prosthesis between the socket and the eyelids may contribute to anterior displacement of the eyelids relative to the canthal tendon support structures, resulting in tarsoligamentous laxity(2).
The superior eyelid sulcus was deeper in anophthalmic sockets than in the contralateral normal eye, regardless of implant shape. A deeper superior sulcus is a common finding in anophthalmic sockets and is likely attributable to insufficient volume support, which destabilizes the tendinous support of the upper eyelid and levator muscle, altering the direction of force and shifting the levator pull from upward to posterior(12).
Inferior displacement of the remaining orbital structures may further affect the position of the levator and superior rectus muscles in anophthalmic socket(1). Although some authors have suggested that conical implants improve superior sulcus deformity, these observations were based on subjective assessments performed without an external ocular prosthesis in place(6). In contrast, the quantitative analysis in the present study demonstrated that neither conical nor spherical implants influenced superior eyelid sulcus depth.
Despite the reduced horizontal palpebral fissure observed in sockets reconstructed with either implant format, eyelid angles remained comparable with those of the contralateral normal eye. These angles may be reduced in the absence of an external ocular prosthesis(13).
This study has limitations, including uncontrolled variables related to the customized external ocular prosthesis. Nevertheless, its strengths include the use of a single observer for measurements, appropriate quantitative tools for assessing eyebrow and eyelid position, direct comparison of conical and spherical implants, and the use of the contralateral normal eye as an internal control. Quantification of these findings enhances understanding of the relationship between eyelid position and anophthalmic sockets reconstructed with different implant formats and may aid in achieving improved aesthetic outcomes.
Further studies are warranted to optimize reconstructive strategies aimed at achieving a symmetrical eyelid positioning in anophthalmic sockets relative to the contralateral normal eye and improving cosmetic satisfaction.
In conclusion, eyebrow and eyelid positions were largely similar in anophthalmic sockets reconstructed with conical or spherical implants, except for a reduced EDM in infraduction associated with conical implants. Both implant formats were associated with a deeper superior eyelid sulcus and a smaller horizontal palpebral fissure compared with the contralateral normal eye.
ACKNOWLEDGMENTS
This study was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (nº: 2013/00131-8).
AUTHORS' CONTRIBUTIONS
Significant contribution to conception and design: Silvana Artioli Schellini. Data acquisition: Carolina Bigetti; Roberta Lilian FSMeneghim; Silvana Artioli Schellini. Data analysis and interpretation: Carolina Bigetti; Roberta Lilian FSMeneghim; Silvana Artioli Schellini. Manuscript drafting: Carolina Bigetti; Silvana Artioli Schellini. Significant intellectual content revision of the manuscript: Carolina Bigetti; Roberta Lilian FSMeneghim; Silvana Artioli Schellini, Carlos Roberto Padovani. Final approval of the submitted manuscript: Carolina Bigetti; Roberta Lilian FSMeneghim; Simone Milani Brandão; Carlos Roberto Padovani; Silvana Artioli Schellini. Statistical analysis: Carlos Roberto Padovani. Obtaining funding: Silvana Artioli Schellini. Supervision of administrative, technical, or material support: Silvana Artioli Schellini. Research group leadership: Silvana Artioli Schellini.
REFERENCES
1. Al Eid S, AlSulaiman HM, Elkhamary SM, AlSheikh O, Ferrero-Galindo A, Kandekhar R, et al. Superior rectus-levator complex in acquired anophthalmic socket repaired with spheric implant - a computed tomography scan and topographic study. Int J Ophthalmol. 2024;17(8):1483-8.
2. Quaranta-Leoni FM, Fiorino MG, Quaranta-Leoni F, Di Marino M. Anophthalmic socket syndrome: prevalence, impact and management strategies. Clin Ophthalmol. 2021;15:3267-81.
3. Kamble VB. Prosthetic correction of postenucleation socket syndrome: a case report. J Indian Prosthodont Soc. 2014;14(Suppl 1):172-6.
4. Vardizer Y, Sobeh T, Prat DL, Ben Simon GJ, Tomkins-Netzer O. Assessing the results of anophthalmic prostheses. Indian J Ophthalmol. 2021;69(7):1876-81.
5. Sousa RL, Schellini SA, Zornoff DC, Padovani CR. [Trends on anophthalmic socket repair in Brazil]. Arq Bras Oftalmol. 2012;75(6):394-7.Portuguese.
6. Rubin PA, Popham J, Rumelt S, Remulla H, Bilyk JR, Holds J, et al. Enhancement of the cosmetic and functional outcome of enucleation with the conical orbital implant. Ophthalmology. 1998; 105(5):919-25.
7. Kang MJ, Jung SK, Cho WK, Paik JS, Yang SW. Long-term surgical outcomes of the multi-purpose conical porous synthetic orbital implant. Korean J Ophthalmol. 2015;29(5):294-300.
8. Tawfik HA, Raslan AO, Talib N. Surgical management of acquired socket contracture. Curr Opin Ophthalmol. 2009;20(5):406-11.
9. Brandão SM, Schellini RA, Peitl O, Zanotto ED, Matayoshi S, Meneghim RL, et al. Conical biosilicate implant for volume augmentation in anophthalmic sockets. J Craniofac Surg. 2020;31(6):1838-40.
10. Jurel SK, Talwar N, Chand P, Singh RD, Gupta DS. Customization of stock eye prosthesis for a pediatric patient by a simplified technique. Int J Clin Pediatr Dent. 2012;5(2):155-8.
11. Singh M, Nayak M, Solanki J, Gupta S, Singh A. Management of an anophthalmic patient by the fabrication of custom made ocular prosthesis. Malays J Med Sci. 2015;22(3):75-9.
12. Gradinaru S, Totir M, Iancu R, Leasu C, Pricopie S, Yasin S, et al. Topographic measurements of eyelids and orbit in enucleated eyes with hydroxyapatite integrated implant versus PMMA implant. J Med Life. 2014;7(Spec Iss 4):74-6.
13. Ha SW, Lee JM, Jeung WJ, Ahn HB. Clinical effects of conjunctiva-Müller muscle resection in anophthalmic ptosis. Korean J Ophthalmol. 2007;21(2):65-9.
Data Availability Statement: The datasets generated and/or analyzed during the current study are already available.
Edited by:
Editor-in-Chief: Newton Kara-Júnior
Submitted for publication:
January 8, 2026.
Accepted for publication:
January 21, 2026.
Approved by the following research ethics committee: UNESP – Faculdade de Medicina de Botucatu (CAAE: 61568816.3.0000.5411).
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.