Arq. Bras. Oftalmol. 2026; 89 (1): 10.5935/0004-2749.2024-0344
Total: 1177
Lígia Barros de Oliveira1; Mauro Eduardo Jurno2,3; Marcelo Maroco Cruzeiro1,5; Leonardo Provetti Cunha1,4,6; Thiago Cardoso Vale1,5
DOI: 10.5935/0004-2749.2024-0344
ABSTRACT
PURPOSE: To evaluate the relationships between retinal changes identified by optical coherence tomography in patients with migraine with aura or migraine without aura and the duration and severity of the disease, as measured by the questionnaire.
METHODS: In this cross-sectional study, 16 patients with migraine with aura and 15 patients with migraine without aura were compared with 16 age- and sex-matched controls without migraine. Retinal parameters were assessed using optical coherence tomography, and disease severity was evaluated using scores.
RESULTS: Foveal choroidal thickness was significantly reduced in migraine patients to controls (p=0.040). Negative correlations were observed between disease duration and total macular thickness (p=0.037), ganglion cell complex thickness (p=0.017), and choroidal thickness (p=0.039) in the migraine without aura Group. Additionally, scores showed an inverse correlation with peripapillary retinal nerve fiber layer thickness (p=0.027) in the migraine without aura Group.
CONCLUSION: Individuals with migraine exhibited significant choroidal thinning compared with controls. Longer disease duration was associated with reduced total macular, ganglion cell complex, and choroidal thickness, while greater migraine-related disability correlated with thinner peripapillary retinal nerve fiber layers.
Keywords: Migraine with aura; Migraine without aura; Nerve fibers; Retina; Macula; Optic disc; Choroid; Tomography, optical coherence; Surveys and questionnaires.
INTRODUCTION
Migraine is one of the most common primary headaches worldwide, with an estimated prevalence of 15.2% in Brazil(1). It is the second leading cause of disability globally and the leading cause of disability among individuals under 50 years of age(2).
Migraine is currently recognized as a neurovascular disorder. Pain attacks are thought to originate from dysfunction in hypothalamic nuclei and brainstem structures, leading to altered cortical excitability, activation of the trigeminovascular pathways and modulation of arterial vasomotor control. These attacks can result in central sensitization and further changes in cortical excitability, predisposing patients to chronic migraine(3).
The retina can be considered an extension of the central nervous system (CNS) because it shares the same embryological and vascular origins and exhibits similar tissue structure. Given these similarities, measurements of retinal and choroidal layer thickness using optical coherence tomography (OCT) may reflect neurovascular changes in patients with migraine. Several studies have investigated the association between migraine and retinal changes assessed by OCT(4). Evidence suggests that structural alterations in the retinal ganglion cell layer (RGCL), peripapillary retinal nerve fiber layer (pRNFL), and choroid occur in both migraine with aura (MwA) and migraine without aura (MwoA) during attack-free periods(4-9). A meta-analysis published in 2021 found that pRNFL thickness is significantly reduced in migraine patients, particularly those with MwA, indicating that this parameter may help differentiate these patients(10).
Given the neurovascular mechanisms underlying migraine, OCT angiography (OCTA) may provide additional information beyond that obtained with OCT. Some studies have reported reduced vascular density (VD) and an enlarged foveal avascular zone in migraine patients compared with controls without headache(11-14). Because the choroid is a highly vascularized tissue, it can be affected not only by migraine attacks but also by other vascular conditions, such as systemic arterial hypertension and diabetic retinopathy(15,16).
The severity and duration of migraine may influence the thickness of retinal and choroidal layers, as previously observed(6,11,17). However, structural changes in the retina and choroid during the interictal phase of migraine remain inconsistent across studies. Therefore, the primary objective of this study was to evaluate the thickness of the retinal layers–specifically the RGCL, pRNFL, and total macula–as well as the choroid, using OCT and OCTA, in patients with MwA and MwoA compared with individuals without migraine. The secondary objective was to evaluate whether migraine duration and severity, measured by the Headache Impact Test-6 (HIT-6)(18), correlate with retinal and choroidal thickness.
METHODS
Study design
This cross-sectional study recruited migraine patients and age- and sex-matched controls without migraine from August 2022 to July 2023. Participants were evaluated at the tertiary headache units of the University Hospital of the and the . OCT and OCTA examinations were performed at the , Minas Gerais. The control group consisted of family members and friends of patients and researchers. All participants provided written informed consent prior to enrollment.
Research participants and instruments
Participants included individuals aged ≤60 years who were diagnosed with MwA or MwoA by neurologists, according to the International Classification of Headache Disorders, 3rd edition (ICHD-3) criteria.(19). The control group consisted of individuals aged ≤60 years without migraine, as confirmed by a neurologist (L.B.O). Inclusion criteria required participants to have spherical refraction within ± 5 diopters, cylinder correction within ± 4 diopters, and intraocular pressure between 10 and 21 mmHg. Exclusion criteria were as follows: (1) neurodegenerative disease of any origin, (2) structural CNS lesion, (3) previous ocular trauma, (4) glaucoma, (5) retinal disease of any cause, (6) myopia or hyperopia greater than four diopters, (7) astigmatism greater than six diopters, (8) cataracts, (9) systemic arterial hypertension, and (10) diabetes mellitus.
All participants underwent comprehensive physical and neurological evaluations. Migraine patients completed the HIT-6 questionnaire(18). A full ophthalmologic examination, including OCT and OCTA images, was performed for all participants and reviewed by ophthalmologist (L.P.C.) to identify any ocular conditions meeting exclusion criteria. OCT and OCTA scans for migraine patients were conducted during the interictal period, defined as at least 48 hours without a migraine attack.
OCT exam
Retinal and choroidal images were acquired in eyes dilated with 1% tropicamide under dark conditions during the same session. A Swept Source OCT device (DRI OCT Triton, Topcon Corporation, Tokyo, Japan) was used with a three-dimensional protocol. High-resolution images (512 × 256 A-scans) of the optic disc (6 × 6-mm) and macula (7 × 7-mm) were obtained(20). Both eyes of each participant were imaged; however, only one eye per patient was included in the analysis. The eye with the best image quality was selected. If both eyes met inclusion criteria, one eye was randomly chosen using a simple coin-flip method (heads or tails). To minimize diurnal variation, all OCT and OCTA examinations were conducted in the morning between 9:00 and 11:00 AM.
The following structures were analyzed: pRNFL; total macula; RGCL plus inner plexiform layer (IPL) plus macular retinal nerve fiber layer (mRNFL), collectively termed the ganglion cell complex (GCC); and the choroid. Ophthalmologic parameters and measurement definitions followed the (APOSTEL) for identification and measurement of the GCC, pRNFL and choroidal thickness(21).
pRNFL thickness was assessed using a three-dimensional optic disc protocol based on a 3.4-mm diameter circle centered on the optic disc. Thickness values were calculated automatically and divided into four quadrants: temporal, superior, nasal, and inferior (Figure 1A).

Total macular and choroidal thicknesses were automatically calculated according to the (ETDRS) grid, divided into nine sectors: fovea, temporal inner, superior inner, nasal inner, inferior inner, temporal outer, superior outer, nasal outer, and inferior outer (Figures 1B and 1C).
Weighted averages of total macular and choroidal thickness were calculated considering the thickness of each of the nine sectors, as detailed in the supplementary material. For GCC measurements, the foveal sector was excluded from the weighted mean because the fovea lacks ganglion cells.
OCTA exam
Superficial VD measurements were acquired using OCTARATM technology (Topcon Corporation, Tokyo, Japan). OCTARA is an algorithm that detects blood flow on the retinal surface by analyzing capillary motion from rapid in vivo Swept Source OCT scans, without the need for contrast injection. This technology allows differentiation between the superficial vascular plexus, located in the ganglion cell layer, and the deep capillary plexus in the inner nuclear layer(21).
OCTA images of the macula were acquired over a 6 x 6 mm area centered on the fovea, but analysis of the superficial capillary plexus was limited to a 3-mm diameter region. VD in the superficial layer was evaluated in five sectors: central, superior, inferior, nasal, and temporal. Values were expressed as percentages, and the mean VD was calculated as a weighted average based on the area of each sector (Figure 2).
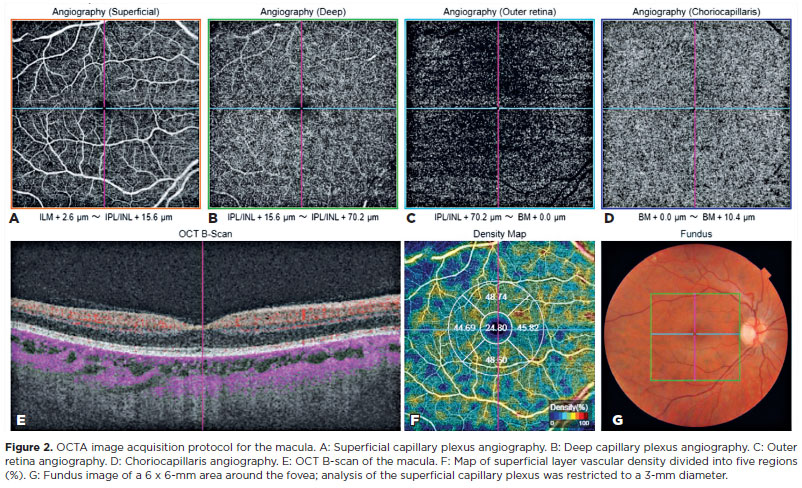
Both the superficial capillary plexus and total choroidal thickness were analyzed. Boundaries and segmentation for OCTA using the Swept-Source Triton were defined as follows:
a) Superficial capillary plexus: from 2.6-µm below the internal limiting membrane to 15.6 µm below the IPL
b) Deep capillary plexus: from 15.6-µm to 70.2-µm below the IPL
c) Outer retina: from 70.2-µm below the IPL to 29-µm below the retinal pigment epithelium (RPE); this layer is primarily avascular in normal eyes
d) Choriocapillaris: from 29-µm to 49 µm below the RPE
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD), and categorical variables are presented as frequencies and percentages. Associations between categorical variables were assessed using the chi-squared test or Fisher's exact test, as appropriate. Correlations between quantitative variables were assessed using Pearson's correlation coefficient. Differences in OCT and OCTA parameters between patients and controls were analyzed using Student's t-test for independent samples. Comparisons among MwA, MwoA, and control groups were performed using one-way analysis of variance (ANOVA) followed by Tukey's post hoc test. Normality and homogeneity of variances were evaluated using the Kolmogorov-Smirnov and Levene tests, respectively. All analyses were conducted using SPSS Statistics version 22.0 (IBM Corp., Armonk, NY, USA). Hypothesis tests were two-tailed, and p-values <0.05 were considered statistically significant. No formal statistical power calculation was performed prior to the study; the sample size was determined by convenience.
RESULTS
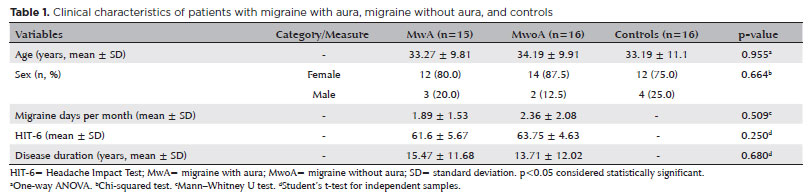
A total of 62 individuals with migraine were invited to participate in the study. Eight were excluded due to clinical comorbidities, 16 did not attend ophthalmological evaluations, 6 had chronic migraine, and 1 was excluded due to poor-quality OCT/OCTA images. The final migraine cohort included 31 patients with episodic migraine: 15 with MwA and 16 with MwoA. Eighteen individuals initially volunteered for the control group; two were excluded due to cataracts and referred for appropriate treatment. Sixteen controls were included in the analysis. There were no missing data. Participant characteristics are presented in table 1. No significant differences were observed between migraine patients and controls in terms of age or sex. Similarly, stratification into MwA (n=15) and MwoA (n=16) subgroups revealed no significant differences. Most participants were female (80.6% of patients and 75% of controls). The mean age ± SD was 33.7 ± 9.7 years for migraine patients and 33.2 ± 11.1 years for controls (p=0.861). Among migraine patients, the mean HIT-6 score ± SD was 62.7 ± 5.2, and the mean disease duration ± SD was 14.6 ± 11.6 years.
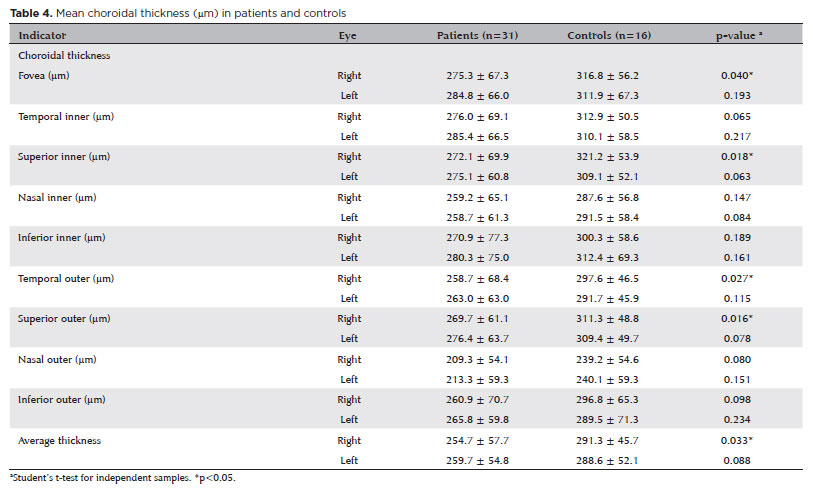
No statistically significant differences were observed between migraine patients and controls in pRNFL, GCC, or total macula thickness. Similarly, macular OCTA variables did not differ significantly between the groups (Tables 2 and 3). Choroidal thickness was significantly reduced in the right eyes of migraine patients compared with controls in the foveal (p=0.040), superior inner (p=0.018), temporal outer (p=0.027), and superior outer (p=0.016) regions, as well as in the average thickness (p=0.033) (Table 4).
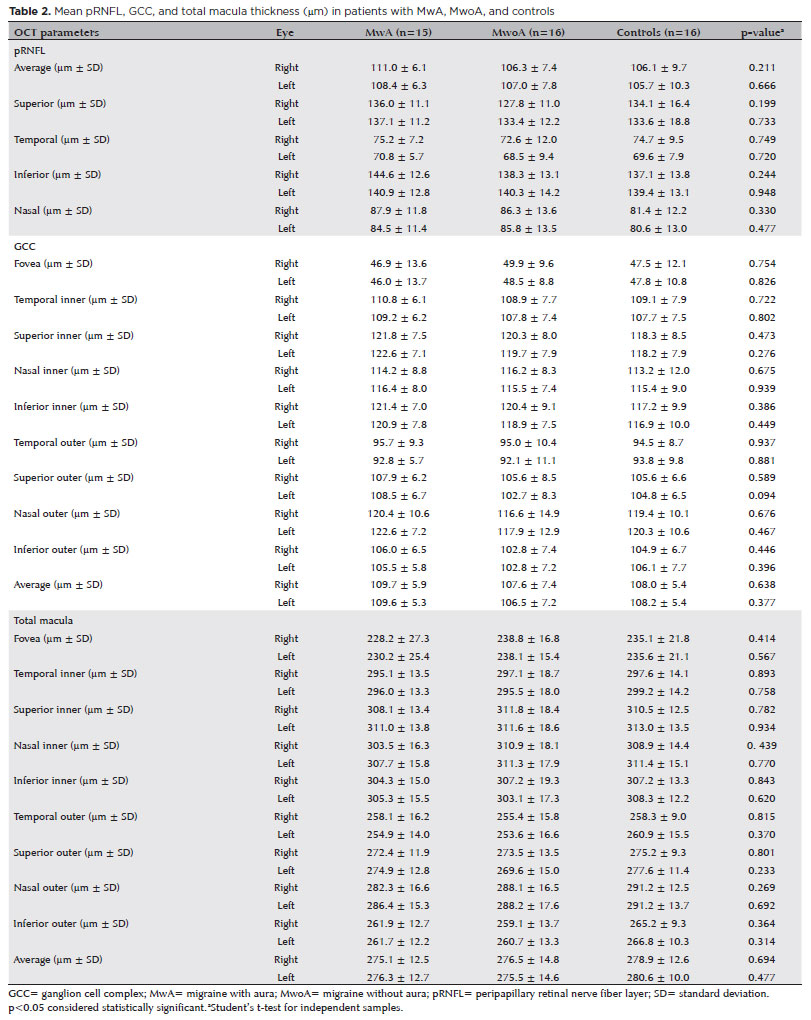
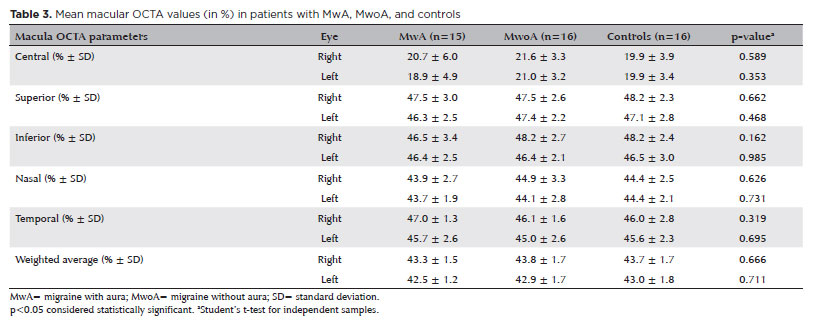
Stratification by migraine subtype (MwA and MwoA) and comparison with controls using ANOVA revealed no significant differences in OCT variables (pRNFL, total macula, GCC, and choroid) or macular OCTA parameters.
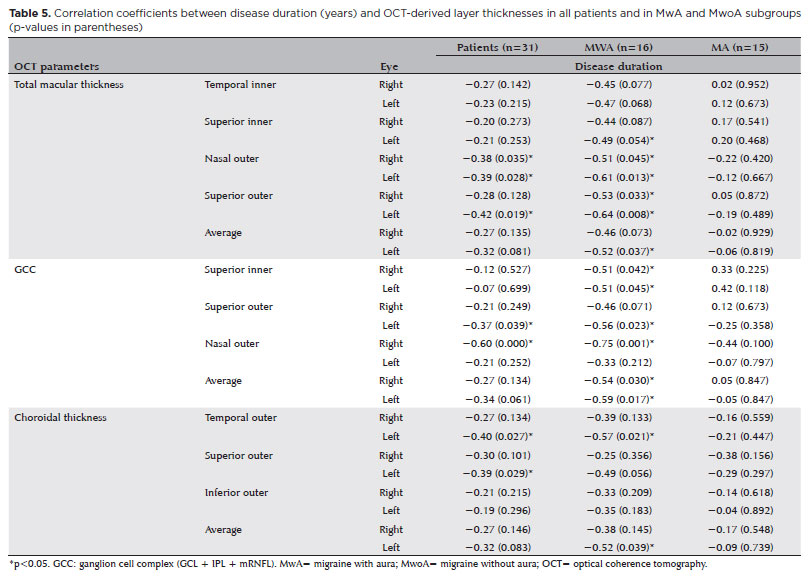
Correlation analysis showed a positive, statistically significant relationship between disease duration and HIT-6 score (r=0.37; p=0.039; n=31). This correlation was stronger in MwA patients (r=0.64; p=0.010; n=15) but not significant in MwoA patients (r=0.14; p=0.611; n=16). Regarding OCT-derived retinal and choroidal thicknesses, negative correlations were observed between disease duration and total macula, GCC, and choroidal thicknesses, with stronger associations in MwoA patients (Table 5).
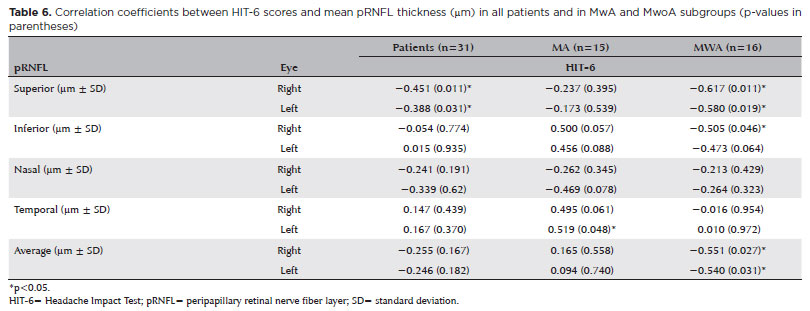
Analysis of the relationship between HIT-6 scores and OCT-derived thickness measurements revealed a statistically significant negative correlation in the average and superior regions of the pRNFL. For the average pRNFL thickness, correlations were observed in both the right (r=−0.55) and left eyes (r=−0.54), with no significant differences between MwA and MwoA Groups. In the superior pRNFL region, correlations were significant in the right (r=−0.45) and left eyes (r=−0.39), with stronger associations in the MwoA Group (right eye, r=−0.62; left eye, r=−0.58) (Table 6).
DISCUSSION
The association between retinal and choroidal thickness changes in migraine patients has been investigated for nearly two decades. In the present study, no statistically significant differences were observed in pRNFL, total macula, GCC, or macular VD measured by OCTA between patients with episodic migraine and controls. In contrast, choroidal thickness was significantly reduced in the fovea, superior inner, temporal outer, and superior outer sectors, as well as in the average thickness, in migraine patients compared with controls.
These findings partially differ from previous studies. A 2012 meta-analysis by Lin et al.(10) reported that pRNFL thickness is reduced in patients with MwA compared with individuals without headache. Other studies have shown that both MwA and MwoA patients exhibited decreased pRNFL thickness compared with healthy controls(6,7). and that RGCL thickness is reduced during the interictal phase in both MwA and MwoA(8,9). However, similar to our results, Taşlı et al. (22) found no differences in pRNFL, GCC, or total macular thickness between MwoA patients and healthy controls. In addition, a population-based study in Finland including 375 migraine patients and 1,489 controls reported no significant differences in pRNFL, macula, or RGCL-IPL thickness(23). Likewise, Lamparter et al.(24), evaluating 1,973 individuals, found no significant associations between migraine and pRNFL thickness changes.
Most OCT studies in migraine patients have reported significant thinning of the choroid. Because the choroid is highly vascularized, its structural changes may reflect the neurovascular pathophysiology of migraine(3,25). Electrophysiological evidence indicates direct activation of trigeminovascular neurons during migraine attacks(26). Sensory innervation of the eye arises from the ophthalmic branch of the trigeminal nerve,(27) positioning the choroid as an input of the trigeminoautonomic system(9). Consistent with prior studies and meta-analyses of observational data, migraine patients exhibited significantly reduced choroidal thickness compared with healthy controls(25). However, this difference was not observed when patients were stratified into MwA and MwoA. This may be explained by the fact that migraine pain primarily involves activation of the trigeminovascular system via peripheral nociceptive neurons, and most migraine attacks occur without aura(4). Consequently, choroidal vascular changes are likely proportional to the frequency and intensity of pain attacks rather than the presence of aura. In line with this, we observed a significant negative correlation between disease duration and choroidal thickness, consistent with findings reported by Abdellatif et al. in 2018(6).
We observed a significant inverse correlation between disease duration and both total macular and GCC thickness. This suggests that longer migraine duration may lead to greater activation of the trigeminovascular system, resulting in vasoconstriction that affects not only the choroid but also the macula and GCC through prolonged oligemia(6). The reduction in choroidal thickness, alongside normal OCTA findings, may indicate a pathophysiological mechanism involving transient ischemia during migraine attacks that spares vascular structures in the interictal period but induces long-term changes in non-vascular components of the choroid and retina. An alternative explanation is direct neurogenic damage to choroidal and retinal tissues, primarily affecting non-vascular structures.
Regarding migraine-related disability, assessed using the HIT-6 questionnaire, we found a statistically significant inverse correlation with average and superior pRNFL thickness. Similar findings have been reported by Martinez et al.(17), who observed an inverse correlation between pRNFL thickness and migraine severity. Abdellatif et al. also demonstrated that migraine severity significantly influences pRNFL and GCC thinning(6). Assessing headache-related disability is a valuable tool for guiding treatment selection, and the HIT-6 is a reliable, widely applicable, and easy-to-use instrument for this purpose(28).
Migraine, particularly with aura, is a recognized risk factor for ischemic stroke and cardiovascular disease(29), which is partly explained by its neurovascular pathophysiology. Previous studies have reported reduced peripapillary and macular VD and an increased foveal avascular zone in patients with MwA(12,13). However, microvascular changes in the retina may manifest primarily when neuroaxonal damage is present. As shown by other authors(30,31), reductions in RNFL and GCC thickness, which reflect neuroaxonal injury, strongly correlate with decreased VD. Accordingly, VD reduction is typically observed alongside significant RNFL and GCC thinning, consistent with findings from prior studies(12-14). These changes may be influenced by disease duration and severity, as supported by our results and previous reports demonstrating inverse correlations between disease duration and GCC thickness, and between migraine severity and RNFL thickness(6,17). In contrast, we observed significant choroidal thinning even in the absence of neuroaxonal damage, suggesting that structural changes in this highly vascularized layer may occur earlier in the disease process in migraine patients.
The variability in retinal layer thickness and macular VD reported across studies may be influenced by differences in study populations (e.g., MwA vs. MwoA, episodic vs. chronic migraine), characteristics of migraine in these populations (attack frequency, intensity, and disease duration), and sociodemographic factors. In addition, technical differences in OCT and OCTA devices and protocols may contribute to inconsistent findings.
This study has several limitations. The relatively small sample size and recruitment from only two research centers may increase the risk of type II errors. Its cross-sectional design precludes causal inferences between retinal or choroidal changes and migraine. Moreover, some statistically significant correlations–many with low correlation coefficients–between disease duration and OCT parameters could be subject to cumulative type I error. Conversely, a major strength of this study is the use of a Swept-Source OCT device, which employs a near-infrared light source (~1,050-nm) that enables deeper tissue penetration and improved visualization of retinal and choroidal layers–a key advantage for examining migraine patients. The device also automatically generates thickness maps based on the ETDRS grid divided into nine sectors, allowing for precise, topographically guided analysis and enhancing the accuracy and reproducibility of the measurements.
In conclusion, compared with controls, individuals with migraine exhibited a significant reduction in choroidal thickness. Longer disease duration was associated with thinner total macula, GCC, and choroidal layers. Furthermore, pRNFL thickness was inversely correlated with migraine-related disability.
AUTHOR CONTRIBUTIONS:
Significant contribution to conception and design: Thiago Cardoso Vale, Leonardo Provetti Cunha. Data Acquisition: Lígia Barros de Oliveira, Mauro Eduardo Jurno, Leonardo Provetti Cunha. Data Analysis and Interpretation: Lígia Barros de Oliveira, Leonardo Provetti Cunha, Marcelo Maroco Cruzeiro, Thiago Cardoso Vale. Manuscript Drafting: Lígia Barros de Oliveira, Mauro Eduardo Jurno, Leonardo Provetti Cunha, Thiago Cardoso Vale. Significant intellectual content revision of the manuscript: Leonardo Provetti Cunha, Marcelo Maroco Cruzeiro, Thiago Cardoso Vale. Final approval of the submitted m anuscript: Lígia Barros de Oliveira, Mauro Eduardo Jurno, Leonardo Provetti Cunha, Marcelo Maroco Cruzeiro, Thiago Cardoso Vale. Statistical analysis: Lígia Barros de Oliveira. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Thiago Cardoso Vale. Research group leadership: Thiago Cardoso Vale.
REFERENCES
1. Peres MF, Queiroz LP, Rocha-Filho PS, Sarmento EM, Katsarava Z, Steiner TJ. Migraine: a major debilitating chronic non-communicable disease in Brazil, evidence from two national surveys. J Headache Pain. 2019;20(1):85.
2. Steiner TJ, Stovner LJ, Vos T, Jensen R, Katsarava Z. Migraine is first cause of disability in under 50s: will health politicians now take notice? J Headache Pain. 2018;19(1):17.
3. Goadsby PJ, Holland PR, Martins-Oliveira M, Hoffmann J, Schankin C, Akerman S. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. 2017;97(2):553-622.
4. Feng YF, Guo H, Huang JH, Yu JG, Yuan F. Retinal nerve fiber layer thickness changes in migraine: a meta-analysis of case-control studies. Curr Eye Res. 2016;41(6):814-22.
5. Reggio E, Chisari CG, Ferrigno G, Patti F, Donzuso G, Sciacca G, et al. Migraine causes retinal and choroidal structural changes: evaluation with ocular coherence tomography. J Neurol. 2017;264(3):494-502.
6. Abdellatif MK, Fouad MM. Effect of duration and severity of migraine on retinal nerve fiber layer, ganglion cell layer, and choroidal thickness. Eur J Ophthalmol. 2018;28(6):714-21.
7. Ekinci M, Ceylan E, Cağatay HH, Keleş S, Hüseyinoğlu N, Tanyildiz B, et al. Retinal nerve fibre layer, ganglion cell layer and choroid thinning in migraine with aura. BMC Ophthalmol. 2014;14(1):75.
8. Acer S, Oğuzhanoğlu A, Çetin EN, Ongun N, Pekel G, Kaşıkçı A, et al. Ocular pulse amplitude and retina nerve fiber layer thickness in migraine patients without aura. BMC Ophthalmol. 2016;16(1):1.
9. Ao R, Wang R, Yang M, Wei S, Shi X, Yu S. Altered retinal nerve fiber layer thickness and choroid thickness in patients with migraine. Eur Neurol. 2018;80(3-4):130-7.
10. Lin X, Yi Z, Zhang X, Liu Q, Zhang H, Cai R, et al. Retinal nerve fiber layer changes in migraine: a systematic review and meta-analysis. Neurol Sci. 2021;42(3):871-81.
11. He N, Shao H, He J, Zhang X, Ye D, Lv Z. Evaluation of retinal vessel and perfusion density in migraine patients by optical coherence tomography angiography. Photodiagnosis Photodyn Ther. 2022;40:103060.
12. Chang MY, Phasukkijwatana N, Garrity S, Pineles SL, Rahimi M, Sarraf D, et al. Foveal and peripapillary vascular decrement in migraine with aura demonstrated by optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2017;58(12):5477-84.
13. Romozzi M, Cuffaro G, Rollo E, Mattei R, Marcelli S, Rizzo S, et al. Microvascular involvement in migraine: an optical coherence tomography angiography study. J Neurol. 2023;270(8):4024-30.
14. Hamurcu MS, Gultekin BP, Koca S, Ece SD. Evaluation of migraine patients with optical coherence tomography angiography. Int Ophthalmol. 2021;41(12):3929-33.
15. Wang W, Liu S, Qiu Z, He M, Wang L, Li Y, Huang W. Choroidal Thickness in Diabetes and Diabetic Retinopathy: A Swept Source OCT Study. Invest Ophthalmol Vis Sci. 2020;61(4):29.
16. Schlenker MB, Thiruchelvam D, Redelmeier DA. Intravitreal anti-vascular endothelial growth factor treatment and the risk of thromboembolism. Am J Ophthalmol. 2015;160(3):569-80.
17. Martinez A, Proupim N, Sanchez M. Retinal nerve fibre layer thickness measurements using optical coherence tomography in migraine patients. Br J Ophthalmol. 2008;92(8):1069-75.
18. Kosinski M, Bayliss MS, Bjorner JB, Ware JE Jr, Garber WH, Batenhorst A, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12(8):963-74.
19. The International Classification of Headache Disorders. 3rd edition (beta version) Cephalalgia. 2013;33(9):629-808.
20. Aytulun A, Cruz-Herranz A, Aktas O, Balcer LJ, Balk L, Barboni P, et al. APOSTEL 2.0 Recommendations for Reporting Quantitative Optical Coherence Tomography Studies. Neurology. 2021; 97(2):68-79.
21. Stanga PE, Tsamis E, Papayannis A, Stringa F, Cole T, Jalil A. Swept-source optical coherence tomography Angio™ (Topcon Corp, Japan): technology Review. Dev Ophthalmol. 2016;56:13-7.
22. Taşlı NG, Ersoy A. Altered macular vasculature in migraine patients without aura: is it associated with ocular vasculature and white matter hyperintensities? J Ophthalmol. 2020;2020:3412490.
23. Ristioja S, Leiviskä IL, Saarela VO, Liinamaa MJ. Retinal neural tissue and vascular calibres in migraine: the Northern Finland Birth Cohort Eye Study. Acta Ophthalmol. 2023;102(5):600-9.
24. Lamparter J, Schmidtmann I, Schuster AK, Siouli A, Wasielica-Poslednik J, Mirshahi A, et al. Association of ocular, cardiovascular, morphometric and lifestyle parameters with retinal nerve fibre layer thickness. PLoS One. 2018;13(5):e0197682.
25. Gouravani M, Salehi MA, Mohammadi S, Arevalo JF. Choroidal thickness in eyes of migraine patients measured using spectral domain-optical coherence tomography: A meta-analysis. Surv Ophthalmol. 2023;68(1):67-77.
26. Zhang X, Levy D, Kainz V, Noseda R, Jakubowski M, Burstein R. Activation of central trigeminovascular neurons by cortical spreading depression. Ann Neurol. 2011;69(5):855-65.
27. Dadaci Z, Doganay F, Oncel Acir N, Aydin HD, Borazan M. Enhanced depth imaging optical coherence tomography of the choroid in migraine patients: implications for the association of migraine and glaucoma. Br J Ophthalmol. 2014;98(7):972-5.
28. Shin HE, Park JW, Kim YI, Lee KS. Headache Impact Test-6 (HIT-6) scores for migraine patients: their relation to disability as measured from a headache diary. J Clin Neurol. 2008;4(4):158-63.
29. Sacco S, Kurth T. Migraine and the risk for stroke and cardiovascular disease. Curr Cardiol Rep. 2014;16(9):524.
30. Suzuki AC, Zacharias LC, Preti RC, Cunha LP, Monteiro ML. Circumpapillary and macular vessel density assessment by optical coherence tomography angiography in eyes with temporal hemianopia from chiasmal compression. Correlation with retinal neural and visual field loss. Eye (Lond). 2020;34(4):695-703.
31. Ugurlu A, Agcayazi SB, Icel E, Budakoglu O, Unver E, Barkay O, et al. Assessment of the optic nerve, macular, and retinal vascular effects of COVID-19. Can J Ophthalmol. 2023;58(6):570-6.
Submitted for publication:
November 22, 2024.
Accepted for publication:
July 18, 2025.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.
Approved by the following research ethics committee: Hospital Universitário da Universidade Federal de Juiz de Fora - UFJF (CAAE: 57756422.0.0000.5133).
Data Availability Statement: The datasets generated and/or analyzed during the current study are included in the manuscript.
Edited by:
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Mário Luiz R. Monteiro
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.