Arq. Bras. Oftalmol. 2025; 88 (5): 10.5935/0004-2749.2024-0103
Total: 1755
Alisson Lima Andrade1; Thiago Pereira Faria1; Roberta Lilian Fernandes de Sousa Meneghim1; Mitsuo Hashimoto1; Edson Nacib Jorge1; Silvana Artioli Schellini1; Eliane Chaves Jorge1
DOI: 10.5935/0004-2749.2024-0103
ABSTRACT
PURPOSE: This study aimed to evaluate abnormalities in the retinal nerve fiber layer and ganglion cell layer in patients with thyroid-associated orbitopathy using optical coherence tomography and to examine their relationship with disease severity.
METHODS: A cross-sectional study was conducted involving 74 participants, comprising 45 individuals with thyroid-associated orbitopathy and 29 healthy controls. All subjects underwent a comprehensive ophthalmological examination and optical coherence tomography using the Cirrus HD-OCT. The clinical activity score and the European Group on Graves’ Orbitopathy severity were also evaluated.
RESULTS: In the thyroid-associated orbitopathy group, the mean peripapillary retinal nerve fiber layer thickness was significantly reduced in the temporal quadrant (p<0.05). No significant differences were found in ganglion cell layer thickness across all sectors when compared with the control group. Besides, a significant correlation was observed between orbitopathy severity and decreased mean peripapillary retinal nerve fiber layer thickness (p<0.001).
CONCLUSION: Optical coherence tomography may serve as a useful tool for identifying changes in the retinal nerve fiber layer and ganglion cell layer in patients with thyroid-associated orbitopathy, including in the inactive phase and prior to the clinical manifestation of dysthyroid optic neuropathy. It may be a helpful adjunct in monitoring disease progression.
Keywords: Graves’ ophthalmopathy; Optic nerve disorders; Retinal nerve fiber layer; Retinal ganglion cells; Optical coherence tomography
INTRODUCTION
Thyroid-associated orbitopathy (TAO) is an autoimmune condition and the most common extra-thyroidal manifestation of Graves’ disease (GD)(1). It is characterized by an initial active or inflammatory phase that primarily affects the orbital soft tissues, including fat, extraocular muscles, and the optic nerve, followed by a prolonged inactive phase(2,3).
TAO is usually bilateral, often asymmetric, and generally mild. However, in 5%-8% of cases, it can progress to a severe form known as dysthyroid optic neuropathy (DON). In approximately 90% of these cases, DON results from optic nerve compression due to enlarged extraocular muscles at the orbital apex, while about 10% are attributed to optic nerve stretching(4,5). This serious complication of TAO necessitates timely evaluation and management to avoid permanent vision loss(6).
Spectral-domain optical coherence tomography (SD-OCT) is a noninvasive diagnostic method that can be used to evaluate TAO activity and detect early signs of DON(7,8). Previous studies suggest that measuring the thickness of the retinal nerve fiber layer (RNFL) and ganglion cell layer (GCL) may help identify structural impairment, even during the inactive phase of TAO(9). OCT findings in individuals with TAO vary, with some studies reporting thickening of the RNFL and choroid, while others have observed RNFL thinning in these patients(10-14). Based on this, the current study aims to compare RNFL and GCL thickness between TAO patients and healthy controls and to examine their correlation with the severity of orbitopathy.
METHODS
A prospective, cross-sectional, controlled study was carried out at the University Hospital of Botucatu Medical School- UNESP, Brazil, between October 2020 and July 2021. The study protocol was approved by the Research Ethics Committee (approval no. 3553947), and all participants provided written informed consent in accordance with the Declaration of Helsinki.
The study involved two groups: a TAO group and a control group. Inclusion criteria for the TAO group were individuals over 18 years of age with a clinical diagnosis of TAO, regardless of gender, ethnicity, or disease stage. For the control group, inclusion criteria were individuals over 18 years old, regardless of gender or ethnicity, with best-corrected visual acuity (BCVA) >20/30 and intraocular pressure (IOP) <21 mmHg, and without a diagnosis of GD or any intraocular pathology.
Exclusion criteria included any conditions that could affect OCT measurements, such as amblyopia, glaucoma, optic nerve or retina disorders, media opacities, and strabismus. The Clinical Activity Score (CAS) was used to assess disease activity based on signs including conjunctival and eyelid redness and swelling, as well as retro-orbital pain; a CAS of ≥3 out of 7 was considered indicative of active TAO. Clinical features were assessed using the criteria established by the European Group on Graves’ Orbitopathy (EUGOGO), which include quality of life impairment, proptosis measurement, lid retraction, diplopia, signs of optic neuropathy, or corneal involvement(15), and the disease was classified as mild, moderate-to-severe, or very severe (sight-threatening)(15).
DON was suspected when a combination of findings was present, including reduced visual acuity, relative afferent pupillary defect, abnormal color vision, visual field defects, optic disc swelling or atrophy, or evidence of orbital apex crowding.
Data collection included demographic information, clinical evaluation, and a comprehensive ophthalmological examination. This involved BCVA (converted to logMAR for statistical analysis), biomicroscopy, exophthalmometry, color vision testing using the Ishihara test, IOP measurement, and indirect fundoscopy. Extraocular muscle thickness was measured using computed tomography (CT) OPTIMA 64 (GE Healthcare, Arlington Heights, USA), with contiguous axial and direct coronal slices of 0.5-1 mm through the orbit. SD-OCT was performed using the Cirrus HD-OCT (Carl Zeiss Meditec Inc., Germany) to evaluate peripapillary RNFL thickness. This was done through three consecutive 360o scans centered on the optic disc with a diameter of 3.4 mm, each composed of 256 A-scans acquired in a single session. Mean RNFL thickness was analyzed in four quadrants: superior, inferior, nasal, and temporal (each covering 90o). GCL thickness was measured using the Macular Cube 512 × 128 protocol, focusing on the area between the GCL and the inner plexiform layer (IPL). Inclusion criteria for scans required a signal strength of ≥6, absence of motion artifacts or segmentation errors, and proper centration on the fovea.
All data were entered into an Excel spreadsheet and analyzed using the SAS® software for Windows (version 9.4, SAS Inc.). The Student’s t-test was used to compare the mean RNFL thickness between the TAO group and the control group. To assess the association between RNFL thickness and ethnicity, only the measurement from the right eye was considered. Variables that did not follow a normal distribution were analyzed using a generalized linear model with a gamma distribution. Discrete variables were evaluated using a Poisson regression model. The chi-squared test was used to examine associations between categorical variables and groups. Spearman’s correlation was used to assess the relationship between RNFL thickness and visual parameters, including dyschromatopsia, logMAR visual acuity, and fundoscopic findings. The correlation between TAO severity and OCT measurements was analyzed and adjusted for potential confounders using the ANOVA test. A p-value <0.05 was considered statistically significant.
RESULTS
The study included 89 eyes from 45 TAO patients and 58 eyes from 29 control participants. The average age was 49.3 ± 14 years for the TAO group and 49.7 ± 14.9 years for the control group. Among the TAO patients, 35 (77.8%) were female, while in the control group, 24 (82.8%) were female. There were no significant differences between the groups regarding age (p=0.90) and gender (p=0.63). Most participants identified as white (66,2%). One eye from the TAO group was excluded due to media opacity.
Systemic arterial hypertension was the most common comorbidity (37.8% in TAO vs. 31% in the control group), followed by diabetes (20% in TAO vs. 17% in the control group) and smoking (13.3% in TAO vs. 3.4% in the control group), with no significant difference between the groups.
Of the 45 TAO patients, 42 (93.3%) were in the inactive phase, with a mean CAS of 1.1 and an average disease duration of 6.6 years. Thirty patients had mild TAO, 12 had moderate-to-severe TAO, and 3 had sight-threatening disease. BCVA and mean IOP did not differ significantly between the TAO and control groups (p>0.05) (Table 1).

The Ishihara test showed abnormalities in only four patients (8.9%) in the TAO group, and no changes were noted in the fundoscopy.
The mean exophthalmometry measurement was significantly higher in the TAO group (20.1 ± 2.86 mm) compared to the control group (14.3 ± 1.86 mm; p<0.05) (Table 1). CT imaging of extraocular muscle thickness was performed in 31 TAO patients, with 3 of them having undergone orbital decompression.
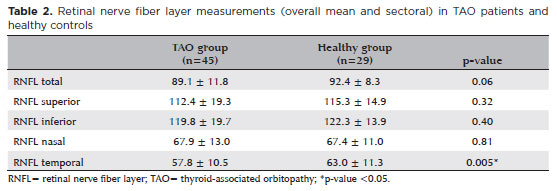
The mean RNFL thickness was lower in the TAO group (89.1 ± 11.8 μm) compared to the control group (92.4 ± 8.3 μm), though this difference was not statistically significant (p=0.06). However, RNFL thickness was significantly reduced in the temporal quadrant of the TAO group compared to the control group (TAO, 57.8 ± 10.5 μm vs. control, 63.0 ± 11.3 μm; p<0.05) (Table 2).
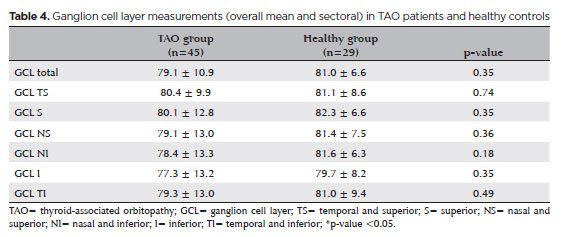
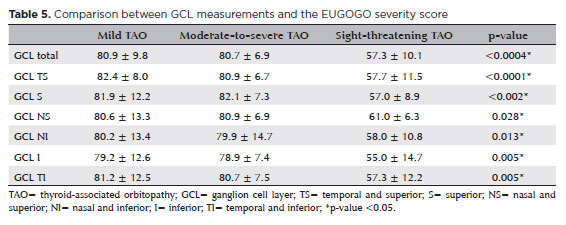
A strong correlation was found between the severity of orbitopathy and the reduction in mean RNFL thickness (p<0.0001), except in the nasal sector (p=0.06), after adjusting for sex and age (Table 3). Additionally, no significant differences were observed in mean GCL thickness between the TAO and control groups (Table 4). However, a correlation was noted between TAO severity and reduced mean GCL thickness (Table 5), particularly in the temporal sector (p<0.0001).

Further analysis showed that ethnicity was not associated with RNFL thickness (p=0.33), while poorer visual acuity was weakly correlated with decreased RNFL thickness (r=-0.317; p<0.001). Dyschromatopsia was also linked to RNFL thinning (r=-0.323; p<0.0001).
DISCUSSION
This study highlights abnormalities in RNFL and GCL measurements using SD-OCT in TAO patients, showing a positive correlation with disease severity.
Our sample shares similar characteristics with previous studies, such as a higher proportion of women(10,16) and a majority of inactive cases without visual impair-ment(17). Although most patients were in the inactive phase and did not show signs of neuropathy, OCT evaluation revealed a significant reduction in RNFL thickness, particularly in the temporal quadrant.
Previous studies have also reported a sectoral reduction in peripapillary RNFL in TAO patients, with many being in the inactive phase(8,9,13,14). Decreased temporal RNFL thickness has been observed in very severe TAO, as well as in acute or chronic optic neuropathy(18), suggesting that RNFL changes can occur even during the quiescent phase of TAO.
This study’s analysis of total peripapillary thickness (including all four quadrants) did not show a statistical difference between the TAO and control groups. However, a lower thickness was observed in the TAO group.
The predominance of inactive TAO patients (93.3%) may have contributed to the small difference between the mean and sectoral RNFL thicknesses. This finding aligns with previous studies that analyzed full-thickness RNFL in TAO patients and healthy controls(19).
Regarding the relationship between TAO severity and RNFL thickness, previous studies have reported varying results(10,13,14). Our study found a strong correlation between orbitopathy severity and reduced mean RNFL thickness, consistent with the findings of Kurt et al., Mugdha et al., and Luo et al.(13,14,17). In contrast, Blum-Meirovitch et al. observed RNFL thickening in the nasal, superior, and inferior sectors, while the temporal sector remained normal(10). These differences may be attributed to the higher proportion of active and severe cases in the Blum-Meirovitch study and others, where RNFL thickening may be associated with the extent of inflammation and optic nerve and orbital swelling in patients with active or severe TAO(9,10,20).
Interestingly, OCT angiography (OCT-A) studies have shown an increase in thickness and a decrease in peripapillary vascular density in eyes with active TAO, a pattern not observed in eyes without activity(21). However, individuals with moderate-to-severe TAO demonstrated a reduction in mean peripapillary RNFL thickness in the nasal and temporal sectors. Conversely, those with sight-threatening TAO showed thickened RNFL in all quadrants(17).
These findings suggest that TAO may exhibit a disconnect between the structural and functional aspects of the optic nerve(8), with structural damage likely occurring before functional impairment. In the current study, patients with more severe TAO did not show visible fundoscopic changes in the optic nerve but exhibited signs of chronic DON process, leading to subclinical RNFL atrophy. This may explain the weak correlation between dyschromatopsia and RNFL thinning.
In line with previous studies, the GCL/IPL thickness was thinner in patients with sight-threatening TAO compared to those with mild or moderate-to-severe orbitopathy in our study(9,22).
The limitations of our study include the relatively small sample size and the low number of patients with severe TAO. Additionally, the absence of data on visual field and refractive errors limited our analysis.
Our study emphasizes RNFL changes in TAO patients, comparing orbitopathy severity and OCT measurements in our racially diverse population. However, no difference in RNFL were observed in relation to race due to the small percentage of self-identified Black and Asian participants.
Our findings suggest that OCT may be a useful tool for detecting changes in peripapillary RNFL and GCL in inactive TAO patients, even in the absence of clinical sign of DON, as OCT can reveal a reduction in RNFL (13,14,17,23).
The key finding was the detection of RNFL abnormalities, even in the most inactive and mild cases of TAO. However, further research and prospective studies are needed to confirm these results and monitor the long-term effects of TAO on the optic nerve in our population.
ACKNOWLEDGMENTS
We would like to thank Dr. Jose Eduardo Corrente for his assistance with the statistical analysis.
AUTHORS’ CONTRIBUTIONS
Significant contribution to conception and design: Alisson Lima Andrade, Edson Nacib Jorge, Eliane Chaves Jorge. Data acquisition: Alisson Lima Andrade, Thiago Pereira Faria. Data analysis and interpretation: Alisson Lima Andrade, Thiago Pereira Faria, Roberta Lilian Fernandes de Sousa Meneghim, Mitsuo Hashimoto, Silvana Artioli Schellini, Eliane Chaves Jorge. Manuscript drafting: Alisson Lima Andrade, Thiago Pereira Faria, Roberta Lilian Fernandes de Sousa Meneghim, Edson Nacib Jorge, Eliane Chaves Jorge. Significant intellectual content revision of the manuscript: Alisson Lima Andrade, Roberta Lilian Fernandes de Sousa Meneghim, Mitsuo Hashimoto, Edson Nacib Jorge, Silvana Artioli Schellini, Eliane Chaves Jorge. Final approval of the submitted manuscript: Alisson Lima Andrade, Thiago Pereira Faria, Roberta Lilian Fernandes de Sousa Meneghim, Mitsuo Hashimoto, Edson Nacib Jorge, Silvana Artioli Schellini, Eliane Chaves Jorge. Statistical analysis: Alisson Lima Andrade, Thiago Pereira Faria, Eliane Chaves Jorge. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Mitsuo Hashimoto, Eliane Chaves Jorge. Research group leadership supervision: Alisson Lima Andrade, Eliane Chaves Jorge.
REFERENCES
1. Kendall-Taylor P, Perros P. Clinical presentation of thyroid associated orbitopathy. Thyroid. 1998;8(5):427-8.
2. Patel A, Yang H, Douglas RS. A new era in the treatment of thyroid eye disease. Am J Ophthalmol. 2019;208:281-8.
3. Fallahi P, Ferrari SM, Elia G, Ragusa F, Paparo SR, Patrizio A, et al. Cytokines as targets of novel therapies for Graves’ ophthalmopathy. Front Endocrinol (Lausanne). 2021;12:654473.
4. Dolman PJ. Grading Severity and Activity in Thyroid Eye Disease. Ophthalmic Plast Reconstr Surg. 2018;34(4S Suppl 1):S34-40.
5. Dolman PJ. Dysthyroid optic neuropathy: evaluation and management. J Endocrinol Invest. 2021;44(3):421-9.
6. Ehlers M, Schott M, Allelein S. Graves’ disease in clinical perspective. Front Biosci (Landmark Ed). 2019;24(1):35-47.
7. Forte R, Bonavolontà P, Vassallo P. Evaluation of retinal nerve fiber layer with optic nerve tracking optical coherence tomography in thyroid-associated orbitopathy. Ophthalmologica. 2010; 224(2):116-21.
8. Sayjn O, Yeter V, ArJtürk N. Optic disc, macula and retinal nerve fiber layer measurements obtained by OCT in thyroid-associated ophthalmopathy. J Ophthalmol. 2016; e9452687,1-7.
9. Guo J, Li X, Ma R, Gan L, Qian J. The changes of retinal nerve fibre layer and ganglion cell layer with different severity of thyroid eye disease. Eye (Lond). 2022;36(1):129-34.
10. Blum Meirovitch S, Leibovitch I, Kesler A, Varssano D, Rosenblatt A, Neudorfer M. Retina and nerve fiber layer thickness in eyes with thyroid-associated ophthalmopathy. Isr Med Assoc J. 2017;19(5):277-81.
11. Özkan B, Koçer ÇA, Altintaş Ö, Karabaş L, Acar AZ, Yüksel N; Medscape. Choroidal changes observed with enhanced depth imaging optical coherence tomography in patients with mild Graves orbitopathy. Eye (Lond). 2016;30(7):917-24.
12. Yu N, Zhang Y, Kang L, Gao Y, Zhang J, Wu Y. Analysis in Choroidal Thickness in Patients with Graves’ Ophthalmopathy Using Spectral-Domain Optical Coherence Tomography. J Ophthalmol. 2018 Dec 23;2018:3529395.
13. Kurt MM, Akpolat C, Evliyaoglu F, Yilmaz M, Ordulu F. [Evaluation of retinal neurodegeneration and choroidal thickness in patients with inactive Graves’ Ophthalmopathy]. Klin Monbl Augenheilkd. 2021;238(7):797-802. German.
14. Mugdha K, Kaur A, Sinha N, Saxena S. Evaluation of retinal nerve fiber layer thickness profile in thyroid ophthalmopathy without optic nerve dysfunction. Int J Ophthalmol. 2016;9(11):1634-7.
15. Bartalena L, Kahaly GJ, Baldeschi L, Dayan CM, Eckstein A, Marcocci C, et al.; EUGOGO. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185(4):G43-67.
16. Del Noce C, Vagge A, Nicolò M, Traverso CE. Evaluation of choroidal thickness and choroidal vascular blood flow in patients with thyroid-associated orbitopathy (TAO) using SD-OCT and Angio-OCT. Graefes Arch Clin Exp Ophthalmol. 2020;258(5):1103-7.
17. Luo L, Li D, Gao L, Wang W. Retinal nerve fiber layer and ganglion cell complex thickness as a diagnostic tool in early stage dysthyroid optic neuropathy. Eur J Ophthalmol. 2021;32(5):3082-91.
18. Park KA, Kim YD, In Woo K, Kee C, Han JC. Optical coherence tomography measurements in compressive optic neuropathy associated with dysthyroid orbitopathy. Graefes Arch Clin Exp Ophthalmol. 2016;254(8):1617-24.
19. Casini G, Marinò M, Rubino M, Licari S, Covello G, Mazzi B, et al. Retinal, choroidal and optic disc analysis in patients with Graves’ disease with or without orbitopathy. Int Ophthalmol. 2020;40(9):2129-37.
20. McKeag D, Lane C, Lazarus JH, Baldeschi L, Boboridis K, Dickinson AJ, et al.; European Group on Graves’ Orbitopathy (EUGOGO). Clinical features of dysthyroid optic neuropathy: a European Group on Graves’ Orbitopathy (EUGOGO) survey. Br J Ophthalmol. 2007;91(4):455-8.
21. Dave TV, Laghmisetty S, Krishnamurthy G, Bejjanki K, Ganguly A, Jonnadula GB, et al. Retinal vascularity, nerve fiber, and ganglion cell layer thickness in thyroid eye disease on optical coherence tomography angiography. Orbit. 2022;41(2):170-7.
22. Zhang T, Xiao W, Ye H, Chen R, Mao Y, Yang H. Peripapillary and Macular Vessel Density in Dysthyroid Optic Neuropathy: An Optical Coherence Tomography Angiography Study. Invest Ophthalmol Vis Sci.2019;60(6):1863-69.
23. Chien L, Go CC, Luna GM, Briceño CA. Changes in retinal nerve fiber layer, ganglion cell complex, and ganglion cell layer thickness in thyroid eye disease: A systematic review. Taiwan J Ophthalmol. 2023;14(2):217-24.
Submitted for publication:
May 28, 2024.
Accepted for publication:
March 21, 2025.
Approved by the following research ethics committee: UNESP – Faculdade de Medicina de Botucatu (CAAE: 18551819.0.0000.5411).
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Jayter de Paula
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.