Arq. Bras. Oftalmol. 2018; 81 (3): 10.5935/0004-2749.20180038
Total: 1599
Fernanda Pedreira Magalhães; Flavio Eduardo Hirai; Luciene Barbosa de Sousa; Lauro Augusto de Oliveira
DOI: 10.5935/0004-2749.20180038
ABSTRACT
Purpose: To evaluate the long-term outcomes of Boston type I keratoprosthesis (B-Kpro) in the management of patients with ocular burn injuries.
Methods: This prospective study included all patients with ocular burns who underwent B-Kpro implantation at a tertiary eye care center between February 2008 and November 2015. Twelve patients (12 eyes) were enrolled. The procedures performed for managing ocular injury were identified, and information on ocular history, surgical procedures performed, and postoperative outcomes was collected. The main outcome measures were visual acuity, prosthesis retention, postoperative complications, and required surgical procedures.
Results: Twelve eyes from 12 patients met the inclusion criteria for B-Kpro implantation, including nine eyes with alkali burns and three eyes with thermal burns. A total of 13 B-Kpro devices were implanted in the 12 eyes. The mean follow-up period was 60.8 months (range, 13-91 months). Preoperative best-corrected visual acuity ranged from counting fingers to light perception. Postoperative best-corrected visual acuity was better than 20/200 in 83.3%, 66.6%, and 57.1% of patients at 12, 48, and 60 months, respectively. The initial keratoprosthesis was retained in 10 (83.3%) eyes and was successfully replaced in one eye. The major cause of worsening of initial visual acuity was advanced glaucoma (four of 12 eyes).
Conclusion: The anatomical and functional results support the use of B-Kpro for managing bilateral limbal stem cell deficiency secondary to ocular burns. However, glaucoma should be carefully evaluated, as it is a continuous threat that may result in irreversible visual loss in this population.
Keywords: Burns, chemical; Eye injuries; Eye burns; Cornea/ surgery; Glaucoma; Prosthesis implantation
RESUMO
Objetivo: Avaliar os resultados em longo prazo do implante da ceratoprótese de Boston tipo 1 (B-Kpro) no tratamento de pacientes vítima de queimadura ocular.
Métodos: Trata-se de um estudo prospectivo envolvendo todos os casos de implante de B-Kpro 1 para queimadura ocular em um centro de oftalmologia terciário durante o período de fevereiro/2008 e novembro/2015. Doze pacientes (doze olhos) foram incluídos no estudo. Os procedimentos realizados para o manejo da queimadura ocular foram identificados, e os dados foram coletados com relação à história oftalmológica do paciente, procedimentos cirúrgicos realizados, e resultados pós-operatórios. Os principais parâmetros avaliados foram acuidade visual, retenção da prótese, complicações pós-operatórias e intervenções cirúrgicas necessárias.
Resultados: Doze pacientes preencheram os critérios de inclusão para implante da B-Kpro, incluindo 09 olhos vítimas de queimadura por álcali e 03 olhos pós queimadura térmica. Um total de 13 B-Kpro tipo 1 foram implantadas em 12 olhos de 12 pacientes. O tempo de seguimento médio foi de 60,8 meses (variando, 13-91 meses). Melhor acuidade visual corrigida pré-operatória variou de conta dedos à percepção luminosa. Melhor acuidade visual corrigida pós-operatória foi melhor que 20/200 em 83,3%, 66,6% e 57,1% dos pacientes em 12 meses, 48 meses e 60 meses, respectivamente. A ceratoprótese inicialmente implantada permaneceu retida em 10 (83,3%) dos olhos e foi re-implantada com sucesso em um olho. A principal causa de piora da acuidade visual inicialmente atingida foi glaucoma avançado (4 de 12 olhos).
Conclusão: Os resultados anatômicos e funcionais reportados neste estudo dão suporte ao uso da B-Kpro para o tratamento da deficiência límbica bilateral secundária a queimadura ocular. Glaucoma é o principal fator limitante e pode causar perda visual irreversível nesses pacientes.
Descritores: Queimaduras químicas; Traumatismos oculares; Queimaduras oculares; Córnea/cirurgia; Glaucoma; Implante de prótese
INTRODUCTION
Boston type 1 keratoprosthesis (B-Kpro) has been shown to be a viable option for visual rehabilitation in eyes with a poor prognosis for primary or repeated keratoplasty after chemical and thermal eye injuries(1-4). However, the maintenance of useful vision after keratoprosthesis surgery is challenging owing to some postoperative adverse events, especially events related to glaucoma and recurrent epithelial defects that can cause corneal sterile necrosis and B-Kpro extrusion(4-7).
Some previous B-Kpro case reports involving tertiary eye care services demonstrated significant visual acuity improvements in ocular injury patients at mean follow-up periods of 25.7(4), 35(2), and 40.7(8) months. However, the mean follow-up periods in these reports were relatively short, and thus, long-term visual outcomes and prognosis could not be assessed. These kinds of ocular injuries have been reported to more frequently affect young men of working age(2).
The purpose of this study was to evaluate the long-term outcomes of B-Kpro in the treatment of patients with severe chemical and thermal ocular burns.
METHODS
This prospective study was conducted at the External Diseases and Cornea Service of the Federal University of São Paulo. After obtaining approval from the institution’s Investigational Review Board, 12 patients (12 eyes) with a previous diagnosis of ocular burns were enrolled in this study between February 2008 and November 2015. The short-term outcomes of 10 of the 12 patients had been described previously(4). Informed consent was obtained from all subjects, and the study was performed according to the tenets of the Declaration of Helsinki.
The patients had bilateral severe corneal opacification due to ocular burns with prior ocular surface reconstruction as needed (correction of lid deformities, symblepharon, and trichiasis, and limbal stem cell transplantation). Of the 12 patients, nine were previously diagnosed with alkali burns and three had thermal burns (two had burns associated with hot oil and one had burns associated with hot plastic). The exclusion criteria were patients aged less than 18 years or those with persistent epithelial defects, end-stage glaucoma, or retinal detachment. Individuals with preserved vision in one eye were also excluded from this study.
All B-Kpro procedures were performed by a single experienced corneal surgeon (L.A.O). B-Kpro with a back plate made of polymethylmethacrylate (PMMA) was implanted in all patients. A preoperative Schirmer’s test was performed in all patients at baseline. Patients were examined one day and one week after surgery and then every month after surgery during the first six follow-up months. Visual acuity, slit-lamp examination, fundoscopy, and intraocular pressure (by digital palpation) measurements were performed at each visit. Regular visual field findings and retinography data were obtained from all patients, when transparency allowed, and data regarding complications were recorded.
Surgical technique
The B-Kpro device was placed according to a previously reported technique(9), using a donor corneal button oversized by 0.5 mm. To improve B-Kpro centration, the standard technique was slightly modified. In the modified approach, 3-mm central trephination was performed before the use of the outer diameter punch in order to minimize descentration(10).
Postoperative management
Postoperative care included the use of a disposable soft contact lens over the keratoprosthesis for an indefinite time in all patients. The lens was replaced every two months. Additionally, a prophylactic regimen of daily topical 0.5% moxifloxacin (one drop thrice a day) and 5% povidone-iodine at every regular visit (one drop every two months) was introduced. Topical prednisolone acetate (1% suspension) eye drops were prescribed according to the severity of the inflammation and were tapered until discontinuation. Serial optic nerve head photographs and visual field tests were performed in all patients, when transparency allowed.
Outcome measures
The main outcome measures were visual acuity outcomes, device retention, and postoperative complications. The collected and analyzed data were based on in situ maintenance of the initial prosthesis.
Statistical analysis
Kaplan-Meier survival analysis was performed to evaluate the anatomical retention of the device. The mean visual acuity was compared between baseline and follow-up at 3, 6, 12, 18, 24, 30, 36, 48, and 60 months postoperatively using the Wilcoxon test. Categorical data were compared using Fisher’s exact test. Analyses were performed using Stata version 10 (Stata Corp., College Park, TX, USA). A p-value <0.05 was considered statistically significant.
RESULTS
A total of 13 B-Kpro devices were implanted in 12 eyes of 12 patients (11 male patients and one female patient). The mean patient age was 41.4 years (range, 27-58 years). One patient underwent a second implantation after keratoprosthesis extrusion secondary to extensive corneal melting. The mean follow-up period was 60.8 months (range, 13-91 months). The primary causes of ocular burns were alkali (nine patients) and thermal injuries (three patients). Preoperative visual acuity ranged from counting fingers to light perception. The initial keratoprosthesis was retained in 10 (83.3%) eyes and was successfully replaced in one eye.
Previous ocular surgery
Among the study patients, five underwent limbal stem cell transplantation (LSCT), one underwent oral mucous membrane grafting (OMMG) for symblepharon correction, and two underwent both procedures. The stem cells for transplantation were generated from HLA-compatible living related donors in six eyes. In one patient, autologous stem cells were generated and expanded ex vivo using an amniotic membrane. LSCT procedures were performed at least three years before keratoprosthesis implantation. No patient was on an immunosuppression regimen at the time of B-Kpro surgery. Nine eyes had previously failed penetrating keratoplasties.
Intraoperative variables
Of the 12 patients, seven received a pseudophakic B-Kpro and five received an aphakic B-Kpro. The recipient and donor trephine sizes were 8.5 and 9.0 mm, respectively, in all patients. Concomitant procedures included cataract extraction with intraocular lens implantation in one case, cataract extraction without intraocular lens implantation in two cases, tarsorrhaphy in two cases, and tube shunt implantation associated with pars plana vitrectomy in one case.
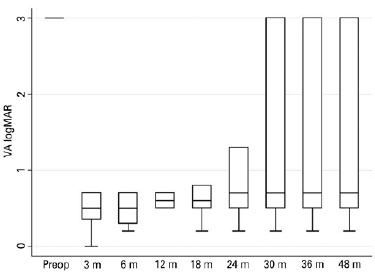
Visual acuity variables
Final postoperative vision showed improvement when compared to preoperative vision in eight of the 12 eyes. It was unchanged in three eyes (secondary to advanced glaucoma) and worsened in one eye. In the patient who showed vision worsening, vision was light perception at baseline, and it did not improve owing to end-stage glaucoma and eventually evolved to no light perception after B-Kpro extrusion. Additionally, end-stage glaucoma could not be diagnosed before B-Kpro implantation owing to an opaque cornea in the preoperative period. All patients were followed for at least one year, and at this time point, 10 eyes (83.3%) achieved a best-corrected visual acuity of 20/200 or better, with five eyes (41.7%) showing vision of 20/60 or better.
Of the 12 eyes, nine were followed up for 48 months postoperatively (Figure 1), and at this time point, six of the nine eyes (66.7%) had visual acuity better than 20/200 (p=0.0018). Seven patients were followed for at least 60 months, and at this time point, four of the seven eyes (57.1%) had visual acuity of 20/200 or better (p=0.05).
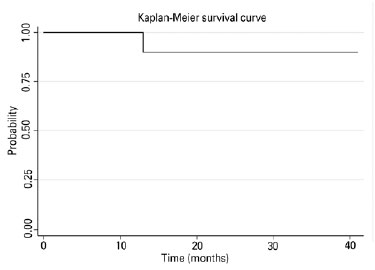
The anatomical retention rate of the initial keratoprosthesis was 83.3% (10/12) at 72 months of follow-up (Figure 2). One patient developed extensive sterile corneal melting with B-Kpro extrusion at one year of follow-up, and this patient required keratoprosthesis replacement.
Glaucoma and keratoprosthesis
Considering that all patients had opaque ocular media at baseline, the suspicion of preoperative glaucoma was based on the ocular ultrasound findings of a suggestive increase in the cup-disk ratio and an elevation in the intraocular pressure (IOP) estimated by digital palpation. Preoperatively, seven eyes (58.3%) were suspicious for glaucoma. One patient underwent transscleral Nd:yttrium-aluminum-garnet (YAG) cyclophotocoagulation before B-Kpro implantation, and two eyes had prior tube shunt implantation. Only one patient underwent concomitant B-Kpro and tube shunt implantation. After B-Kpro implantation, an elevated IOP was present in seven of the 12 eyes (58.3%), and topical hypotensive drugs were prescribed. Of the seven patients suspected with glaucoma preoperatively, six were confirmed to have glaucoma after the procedure and three (50%) showed glaucoma progression. These three patients presented cupping of the optic disc during the follow-up period. Two eyes with no suspicion of glaucoma before B-Kpro implantation developed a high IOP and cupping of the optic disc, which required glaucoma surgery.
Postoperative complications and management
One of the most common complications was retroprosthetic membrane formation, which was noted in five of the 12 eyes (41.6%). All of these eyes were successfully treated with YAG laser membranotomy, and no patient required surgical membranectomy.
The other complications noted after B-Kpro implantation were persistent corneal epithelial defect (PED) that evolved to corneal melting (four eyes, 33.3%), corneal thinning with no epithelial defect (one eye, 8.3%), newly diagnosed glaucoma (two eyes, 16.7%), and glaucoma progression (three eyes out of six, 50%). One patient (8.3%) experienced retinal detachment, and one patient (8.3%) showed infectious keratitis. There was no patient with endophthalmitis.
The other procedures performed after initial B-Kpro implantation were keratoprosthesis replacement (one eye, 8.3%), corneal patch grafting as the first treatment in the same eye that underwent B-Kpro extrusion (one eye, 8.3%), amniotic membrane transplantation (one eye, 8.3%), cyanoacrylate glue use for corneal thinning/ melting (three eyes, 25%), pars plana vitrectomy for retinal detachment (one eye, 8.33%), and tube shunt implantation (one eye, 8.3%).
The mean baseline Schirmer’s test value was 15.3 ± 9.6 mm (range, 4-30 mm). The four eyes that developed corneal melting had a mean baseline Schirmer’s test value of 10.0 ± 6.9 mm, while the remaining eight eyes that did not develop this complication had a mean value of 17.8 ± 9.9 (p=0.169). Among eight patients who underwent ocular surface procedures, such as limbal transplantation, prior to B-Kpro implantation, four patients developed corneal melting. None of the four patients who had no procedures for ocular surface reconstruction showed corneal melting (p=0.208).
DISCUSSION
This study confirmed that B-Kpro implantation is a valid option for visual rehabilitation in patients with a severely damaged ocular surface secondary to ocular burns, and this finding is in agreement with findings of relevant studies(2-4,7,8). Most patients experienced an initially significant visual acuity improvement (83.3% of patients). However, during follow-up visits, the maintenance of visual acuity better than 20/200 decreased over time, with 83.3% (p=0.0058), 66.7% (p=0.0018), and 57.1% (p=0.05%) of patients showing maintenance at 12, 48, and 60 months, respectively.
A successful procedure may rapidly restore vision in eyes without prognosis with conventional corneal surgery(6,11). The finding of this study that maintenance of initial visual acuity is challenging is consistent with the findings of previous studies(12,13). In this study, newly diagnosed glaucoma and glaucoma progression were the major causes of decreased visual acuity over time.
Glaucoma is a potential vision-threatening complication in patients who have received a keratoprosthesis, and it presents the greatest challenge after successful B-Kpro implantation(14,15). It has been reported to be the primary reason for visual acuity loss after B-Kpro implantation(16). Furthermore, patients with severe chemical and thermal injuries intrinsically have a high prevalence of glaucoma(17,18). The management of glaucoma in these patients is problematic, as there is no accurate approach to measure IOP and no standardized protocol with regard to management(19). In addition, the optic nerves of alkali-injured eyes appear to be more vulnerable to glaucomatous damage even at normal IOP(13), as alkali burns appear to be associated with retinal ganglion cell apoptosis secondary to inflammatory cytokines that are induced by anterior segment injury(20). It has been postulated that patients with glaucoma before B-Kpro implantation should be considered for glaucoma surgery before B-Kpro implantation or simultaneously with implantation(21). Additionally, in previous studies, a high number of eyes with disc pallor after B-Kpro implantation suggested that additional mechanisms other than elevated IOP might play a role in the type of optic neuropathy(5,22). The absence of progressive end-stage glaucoma cases in the study on aniridia by Rixen et al.(23) suggested that simultaneous empiric glaucoma shunt procedures and B-Kpro implantation might improve outcomes. However, serious complications have been reported in patients who have undergone B-Kpro implantation with preexisting glaucoma drainage devices, including hypotony, choroidal detachment, and suprachoroidal hemorrhage(23).
PED evolving to corneal melting was another significant complication, and it was noted in 33% of patients. Ocular surface complications due to suboptimal limbal stem cell function associated with incomplete bio-integration of B-Kpro donor cornea can pose a continuous threat to the retention of the prosthesis and maintenance of long-term visual acuity(8). Although there is a possibility of sterile corneal ulceration in all indications of B-Kpro, the risk is greater in eyes with limbal stem cell dysfunction(8). Treatment of ocular surface dysfunction before B-Kpro implantation is important, and it might be related to a low rate of corneal melting in ocular burn patients. We could not identify any statistical correlation between previous procedures for rehabilitating the ocular surface before B-Kpro surgery and the incidence of corneal melting (p=0.208), probably because of the small sample size. Patients who showed corneal thinning/melting had lower Schirmer’s test values; however, the finding was not statistically significant (p=0.169).
Postoperative infection is a concern, and it has been reported to occur in about 3.2-17% of patients(24-26). Microbial keratitis increases the risk of B-Kpro retention, and bacterial endophthalmitis is considered as the greatest vision threat for any type of Kpro, which has devastating consequences(27). Although the recommended prophylaxis routine involves the daily use of topical vancomycin and fluoroquinolone drops(28), the high cost of topical 1.4% vancomycin and handling difficulties are barriers for use in Brazil. Thus, we support the use of topical 0.03% moxifloxacin thrice a day along with povidone iodine 5% one drop at every visit(23), and the overall infection rate in this series was 8.3%. Considering B-Kpro in ocular burn patients, Phillips et al.(8) reported a high incidence of infectious complications (44%), although a standard international antibacterial prophylactic scheme was used for high-risk patients(26), with topical vancomycin and a fourth-generation fluoroquinolone. However, all cases of microbial keratitis/endophthalmitis in that study occurred before the addition of quarterly povidone-iodine rinses and the topical amphotericin B antimicrobial prophylactic regimen.
Retroprosthetic membrane formation is one of the most common complications, and it has been reported in 25-65% of patients(15,29). The etiology of retroprosthetic membrane is unknown, and some authors from the Boston type 1 Keratoprosthesis Study Group have suggested that it is related with inflammatory conditions, such as infectious keratitis and aniridia, and that chemical burns might have a protective effect(29). The rate of retroprosthetic membrane formation in our ocular burn patients was 41.6%, which is comparable to the rate reported in previous studies(6,25,30,31). A retro-backplate membrane identified on anterior segment optical coherence tomography (AS-OCT) imaging might be correlated with an increased risk of sterile keratolysis, possibly because of impedance of nutritional support from the aqueous humor(32). In the present study, four of five patients (80%) who developed a retroprosthetic membrane showed corneal melting. This observation should be assessed in further studies.
In summary, the anatomical and functional results in this study indicated the capability of B-Kpro for visual rehabilitation in patients with thermal or chemical ocular burns, who have experienced unsuccessful treatment for vision loss. However, the maintenance of successfully initial results with B-Kpro implantation remains a challenge. A close and rigorous follow-up with a multidisciplinary ophthalmologic team should be considered mandatory to avoid complications that can limit long-term outcomes, and there should be special focus on diagnosing and controlling glaucoma, as well as dealing with any sign of corneal sterile necrosis, which is a major sight-threatening complication in this population.
REFERENCES
1. Yaghouti F, Nouri M, Abad JC, Power WJ, Doane MG, Dohlman CH. Keratoprosthesis: preoperative prognostic categories. Cornea. 2001; 20(1):19-23.
2. Harissi-Dagher M, Dohlman CH. The Boston Keratoprosthesis in severe ocular trauma. Can J Ophthalmol. 2008;43(2):165-9.
3. Sejpal K, Yu Fei, Aldave AJ. The Boston Keratoprosthesis in the management of corneal limbal stem cell deficiency. Cornea. 2011; 30(11):1187-94.
4. Magalhães FP, Hirai FE, Sousa LB, Oliveira LA. Boston Type 1 keratoprosthesis outcomes in ocular burns. Acta Ophthalmol. 2013; 91(6):432-6.
5. Kamyar R, Weizer JS, de Paula FH, Stein JD, Moroi SE, John D, et al. Glaucoma associated with Boston type I Keratoprosthesis. Cornea. 2012;31(2):134-9.
6. Greiner MA, Li JY, Mannis MJ. Longer-term vision outcomes and complications with the Boston type 1 keratoprosthesis at the University of California, Davis. Ophthalmology. 2011;118(8):1543-50. Comment in: Ophthalmology. 2012;119(1):202-3; author reply 203.
7. de la Paz MF, Stoiber J, de Rezende Couto Nascimento V, de Toledo JA, Seyeddain O, Hitzl W, et al. Anatomical survival and visual prognosis of Boston type 1 keratoprosthesis in challenging cases. Graefes Arch Exp Ophthalmol. 2014;252(1):83-90.
8. Phillips DL, Hager JL, Goins KM, Kitzmann AS, Greiner MA, Cohen AW, et al. Boston Type 1 keratoprosthesis for chemical and thermal injury. Cornea. 2014;33(9):905-9.
9. Dohlman CH, Abad JC, Dudenhoefer EJ. Keratoprosthesis: beyond corneal graft failure. In: Spaeth GL, editor. Ophthalmic surgery: principles and practice. 3rd ed. Philadelphia: W.B. Saunders; 2002. p.199-207.
10. Khalifa YM, Moshirfar M. Improved centration of the type 1 Boston Keratoprosthesis in donor carrier tissue. Clin Ophthalmol. 2010; 4:931-3.
11. Dunlap K, Chak G, Aquavella JV, Myrowitz E, Utine CA, Akpek E. Short-term visual outcomes of Boston type 1 keratoprosthesis implantation. Ophthalmology. 2010;117(4):687-92.
12. 12. Gu J, Zhai J, Zhou S, Chen J. Boston keratoprosthesis outcomes in severe ocular chemical burns in southern china: a retrospective study. Adv Ther. 2016;33:760-73.
13. Cade F, Grosskreutz CL, Tauber A, Dohlman CH. Glaucoma in eyes with severe chemical burn, before and after keratoprosthesis. Cornea. 2011;30(12):1322-7.
14. Li JY, Greiner MA, Brandt JD, Lim MC, Mannis MJ. Long-term complications associated with glaucoma drainage devices and Boston keratoprosthesis. Am J Ophthalmol. 2011;152(2):209-18. Comment in: Am J Ophthalmol. 2011;152(6):1078-9; Am J Ophthalmol. 2012;154(1):207-8; author reply 208-9.
15. Chew HF, Ayres BD, Hammersmith KM, Rapuano CJ, Laibson PR, Myers JS, et al. Boston keratoprosthesis outcomes and complications. Cornea. 2009;28(9):989-96.
16. Ahmad S, Akpek EK, Gehlbach PL, Dunlap K, Ramulu PY. Predictors of visual outcomes following Boston type 1 keratoprosthesis implantation. Am J Ophthalmol. 2015;159(4):739-47.
17. Tseng SC, Chen JJ, Huang AJ. Classification of conjunctival surgeries for corneal diseases based on stem cell concept. Ophthalmol Clin North Am. 1990;3(4):595-610.
18. Tsai JH, Derby E, Holland EJ, Khatana AK. Incidence and prevalence of glaucoma in severe ocular surface disease. Cornea. 2006; 25(5):530-2.
19. Nguyen P, Chopra V. Glaucoma management in Boston keratoprosthesis type I recipients. Curr Opin Ophthalmol. 2014;25(2):134-40.
20. Cade F, Paschalis EI, Regatieri CV, Vavvas D, Dana MR, Dohlman CH. Alkali burn to the eye: protection using TNF-α inhibition. Cornea. 2014;33(4):382-9.
21. Aldave AJ, Kamal KM, Vo RC, Yu F. The Boston type I keratoprosthesis: improving outcomes and expanding indications. Ophthalmology. 2009;116(4):640-51.
22. Crnej A, Paschalis EI, Salvador-Culla B, Tauber A, Drnovsek-Opup B, Shen LQ, et al. Glaucoma progression and role of glaucoma surgery in patients with Boston keratoprosthesis. Cornea. 2014; 33(4):349-54.
23. Rixen JJ, Cohen AW, Kitzmann AS, Wagoner MD, Goins KM. Treatment of aniridia with Boston Type I Keratoprosthesis. Cornea. 2013; 32(7):947-50.
24. Magalhães FP, do Nascimento HM, Ecker DJ, Sannes-Lowery KA, Sampath R, Rosenblatt MI, et al. Microbiota evaluation of patients with a Boston type I keratoprosthesis treated with topical 0.5% moxifloxacin and 5% povidone iodine. Cornea. 2013;32(4):407-11.
25. Bradley JC, Hernandez EG, Schawb IR, Mannis MJ. Boston type I keratoprosthesis: the University of California Davis experience. Cornea. 2009;28(3):321-7.
26. Kim MJ, Yu F, Aldave AJ. Microbial keratitis after Boston type I keratoprosthesis implantation: incidence, organisms, risk factors, and outcomes. Ophthalmology. 2013;120(11):2209-16.
27. Durand ML, Dohlman CH. Successful prevention of bacterial endophthalmitis in eyes with the Boston keratoprosthesis. Cornea. 2009;28(8):896-901.
28. Khan BF, Harissi-Dagher M, Khan DM, Dohlman CH. Advances in Boston keratoprosthesis: enhancing retention and prevention of infection and inflammation. Int Ophthalmol Clin. 2007;47(2):61-71.
29. Zerbe BL, Belin MW, Ciolino JB; Boston Type 1 Keratoprosthesis Study Group. Results from the multicenter Boston Type 1 Keratoprosthesis Study. Ophthalmology. 2006;113(10):1779-84.
30. Rudnisky CJ, Belin MW, Todani A, Al-Arfai K, Ament JD, Zerbe BJ, Ciolino JB; Boston Type 1 Keratoprosthesis Study Group. Risk factors for the development of retroprosthetic membranes with Boston keratoprosthesis type 1: multicenter study results. Ophthalmology. 2012;119(5):951-5.
31. de Oliveira LA, Pedreira Magalhães F, Hirai FE, de Souza LB. Experience with Boston keratoprosthesis type 1 in the developing world. Can J Ophthalmol. 2014;49(4):351-7.
32. Sivaraman KR, Hou JH, Allemann N, de la Cruz J, Cortina MS. Retroprosthetic membrane and risk of sterile keratolysis in patients with type I Boston Keratoprosthesis. Am J Ophthalmol. 2013; 155(5): 814-22.
Submitted for publication:
July 27, 2017.
Accepted for publication:
November 15, 2017.
Approved by the following research ethics committee: Universidade Federal de São Paulo (# 1179/07)
Funding: No specific financial support was available for this study
Disclosure of potential conflicts of interest: None of the authors have any potential conflict of interest to disclose

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.