INTRODUCTION
Increasing attention is being focused on the impact of corneal parameters as potential determinants of the risk of glaucoma. Many studies have investigated the question of whether corneal thickness and/or biomechanical properties have an influence on glaucoma. The Ocular Hypertensive Treatment Study (OHTS) and the Early Manifest Glaucoma Treatment Study (EMGT) demonstrated a link between central corneal thickness (CCT) and the risk of glaucoma(1,2).
A morphological link is possible between aspects of the front of the eye and optic nerve head (ONH) parameters. Owing to the anatomic continuity of the cornea, sclera, and optic disc lamina, it can be hypothesized that corneal parameters may reflect parameters of the ONH, such as optic disc area (DA) and deformability of the lamina cribrosa. For example, in a study analyzing anterior segment structures in eyes with an optic disc pit, a significantly smaller back radius of corneal curvature was found in eyes with an optic disc pit(3). Since the corneal stroma, corneal endothelium, and optic nerve lamina cribrosa differentiate from the neural crest, they are embryologically related to one another(4).
Many reports have suggested that the risk of glaucoma is related in some way to optic disc parameters, particularly optic disc size and cup/disc ratio (C/D)(5). For example, it has been suggested that large discs may be susceptible to glaucomatous damage at low levels of intraocular pressure (IOP)(6). In support of this hypothesis, the size of the ONH has been reported to be larger in patients with normotensive glaucoma than in those with primary open angle glaucoma (POAG)(7). Although disc size was not associated with the development of POAG in OHTS participants(8), the OHTS suggested that vertical and horizontal C/D was a good predictor of the onset of POAG(1).
Although the relationships among CCT, corneal biomechanics, and ONH parameters have been examined, there is little information on the relationships between other corneal parameters (such as corneal volume and corneal refractive power) and the OHN in healthy subjects. Moreover, it is also unclear whether anterior chamber parameters (depth and volume) are significantly correlated with ONH parameters.
The aim of this study was to determine whether there is a relationship between anterior segment morphology and the dimensions and shape of the ONH. To the best of our knowledge, no study has evaluated the correlations between anterior segment parameters measured by the Scheimpflug imaging system and optic disc parameters measured by confocal scanning laser ophthalmoscopy.
METHODS
This research was carried out in accordance with the Declaration of Helsinki and after approval from the Institutional Review Board of the Ankara Numune Research and Education Hospital. All participants provided informed consent for participation in this study. The subjects were between 20 and 60 years of age and were prospectively recruited among patients presenting to the outpatient clinic of Ulucanlar Eye Research and Education Hospital.
Individuals with a history of vascular, circulatory (diabetes mellitus, hypertension, or hypotension), autoimmune, or neurological diseases (including migraine), neoplasia, or chronic medication usage were excluded. The exclusion criteria included history of glaucoma, uveitis, ocular surgery, or trauma; any corneal scarring pathology, such as infection or trauma, and any previous history of corneal or intraocular surgery. The participants were not using topical eye drops. We limited the contribution of each patient to the right eye to avoid interdependency.
The inclusion criteria were best corrected visual acuity ≥20/20, spherical equivalent between -1.0 and +1.0 diopters (D) with cylinder power <1 D, IOP<22 mmHg, open anterior chamber angle, and normal-appearing ONH. Normal-appearing ONH was defined as intact neuroretinal rim without splinter hemorrhage, notches, localized pallor, or asymmetry of the cupping <0.2 between the eyes, taking into account disc size. Participants with an optic disc abnormality (such as drusen or tilted disc) were excluded.
Eligible subjects were consecutively included and received a comprehensive ocular examination, including medical history, manifest refraction, IOP measurement by Goldmann applanation tonometry, gonioscopy, and slit lamp and fundus examination. The subjects underwent disc imaging with a confocal scanning laser ophthalmoscope (Heidelberg Retina Tomograph III (HRT III); Heidelberg Engineering, Dossenheim, Germany). Subjects whose HRT III images had a standard deviation <50 were included in the final analysis. The same examiner performed all measurements. The details of this technique have been described elsewhere(8). The parameters obtained from HRT III hardware were DA (mm2), cup area (CA) (mm2), rim area (RA) (mm2), cup volume (CV) (mm3), rim volume (RV) (mm3), cup to disc area ratio (C/D area), linear cup to disc ratio (linear C/D), and mean and maximum cup depth (CD) (mm).
Anterior segment parameters were obtained automatically by the Pentacam Scheimpflug system (Oculus Gmbh, Wetzlar, HE, Germany) with a quality score >95. Pentacam software constructs the three-dimensional image of the anterior segment and calculates the anterior chamber parameters. This imaging provides measurements of anterior chamber depth (ACD) and anterior chamber volume (ACV). Corneal thickness at the apex point (regarded as the CCT) and corneal volume values were also recorded. The amount of anterior and posterior corneal refractive power (the dioptric power of the posterior corneal surface is negative) within a span of 3.0 mm from the centre was also measured.
Axial length measurements were recorded with an 11-MHz probe of an A-mode ultrasound device (Cine Scan; Quantel Medical SA, Clermont-Ferrand, France). Measurements were performed 5 min after instillation of one drop of proparacaine hydrochloride 0.5% (Alcaine; Alcon Laboratories, Hemel Hempstead, UK).
The data were evaluated by the SPSS program version 22.0 (IBM Corp.) The data obtained with both devices were analyzed descriptively. Normality of the variables was checked by the Kolmogorov-Smirnov test. The distribution of the main variables was normal. Age and optic DA have a known impact on anterior segment and ONH parameters, respectively. We carried out a partial correlation analysis to investigate the relationship between anterior segment and optic nerve head parameters, controlling for age and optic DA. In addition, we used multiple linear regression analysis to examine the associations of the anterior segment and ONH parameters. All models were adjusted for age and optic DA.
RESULTS
This clinical observational study included 200 eyes of 200 Caucasian individuals (82 men and 118 women). The mean age was 25.8 ± 10.5 years (range, 20-60 years), and the mean refractive error was -0.14 ± 0.28 D as spherical equivalent (range, -1.50 to +1.25 D). The mean axial length was 22.85 ± 0.49 mm (range, 22.06-23.49 mm). The mean IOP was 15.6 ± 3.66 mmHg (range, 8-22 mmHg). The anterior segment and optic disc parameters are summarized in tables 1 and 2, respectively.
Table 1 Optic nerve parameters of the participants
| Parameter | Mean | Minimum | Maximum | SD |
|---|---|---|---|---|
| Disc area (mm2) | 2.20 | 1.31 | 3.60 | 0.53 |
| Cup area (mm2) | 0.47 | 0.00 | 1.74 | 0.35 |
| Rim area (mm2) | 1.72 | 0.96 | 2.58 | 0.35 |
| Cup volume (mm3) | 0.11 | 0.00 | 0.67 | 0.13 |
| Rim volume (mm3) | 0.47 | 0.18 | 1.04 | 0.15 |
| C/D area | 0.20 | 0.00 | 0.52 | 0.12 |
| Linear C/D | 0.42 | 0.00 | 0.72 | 0.15 |
| Mean cup depth (mm) | 0.20 | 0.02 | 0.51 | 0.10 |
| Maximum cup depth (mm) | 0.58 | 0.07 | 1.21 | 0.24 |
Table 2 Anterior segment parameters of the participants
| Parameter | Mean | Minimum | Maximum | SD |
|---|---|---|---|---|
| Anterior corneal refractive power (D) | 043.16 | 0-39.90 | 0-47.50 | 01.45 |
| Posterior corneal refractive power (D) | 0 -6.27 | 00-5.70 | 00-7.00 | 00.25 |
| Central corneal thickness (µm) | 555.20 | -460.00 | -671.00 | 33.10 |
| Corneal volume (mm3) | 060.85 | 0 53.10 | 0-72.20 | 03.43 |
| Anterior chamber volume (mm3) | 162.84 | 0 87.00 | -278.00 | 40.23 |
| Anterior chamber depth (mm) | 002.89 | 00-2.07 | -003.85 | 00.37 |
The study found statistically significant negative correlations between CCT and DA (p=0.002, r=-0.217) and between corneal volume and DA (p=0.001, r=-0.239). Significant negative correlations were found between ACV and DA (p=0.034, r=-0.150) and between ACD and DA (p=0.028, r=-0.156).
Partial correlation analysis to investigate the relationships among anterior segment and optic nerve head parameters, controlling for age and optic DA, showed that corneal refractive power (both anterior and posterior) correlated well with most ONH parameters except CV and CD (Table 3). Pearson’s partial correlation coefficient showed no statistically significant correlations between CCT and ONH parameters.
Table 3 Partial correlation coefficients between corneal and optic nerve head parameters after eliminating the influence of age and optic disc area of the participants
| Parameter | Cup area (mm2) | Rim area (mm2) | Cup volume (mm3) | Rim volume (mm3) | C/D area ratio | Linear C/D ratio | Mean cup depth (mm) | Max cup depth (mm) |
|---|---|---|---|---|---|---|---|---|
| Anterior corneal refractive power (D) | ||||||||
| r | -0.242 | 0.240* | -0.028 | -0.347* | <-0.238* | -0.244* | -0.035 | -0.017 |
| p | <0.001* | -0.001* | -0.690 | -<0.001* | -0.001* | <0.001* | -0.620 | -0.810 |
| Posterior corneal refractive power (D) | ||||||||
| r | -0.225 | -0.223* | *0.048 | -0.357* | -<0.222* | -0.251* | -0.034 | -0.037 |
| p | <0.001* | -0.002* | -0.500 | -<0.001* | -0.002* | <0.001* | -0.630 | -0.600 |
| Corneal thickness (µm) | ||||||||
| r | -0.049 | -0.051* | -0.036 | <--0.100* | -0.002* | --0.049* | -0.006 | -0.033 |
| p | -0.490 | -0.470* | -0.610 | -0.160* | -<0.940* | -0.490* | -0.940 | -0.640 |
| Corneal volume (mm3) | ||||||||
| r | -0.050 | 0.048* | -0.015 | <-0.074* | -0.090* | --0.112* | -0.001 | -0.054 |
| p | -0.480 | -0.500* | 0.840 | -0.300* | <-0.210* | -0.120* | -0.990 | -0.450 |
*statistically significant.
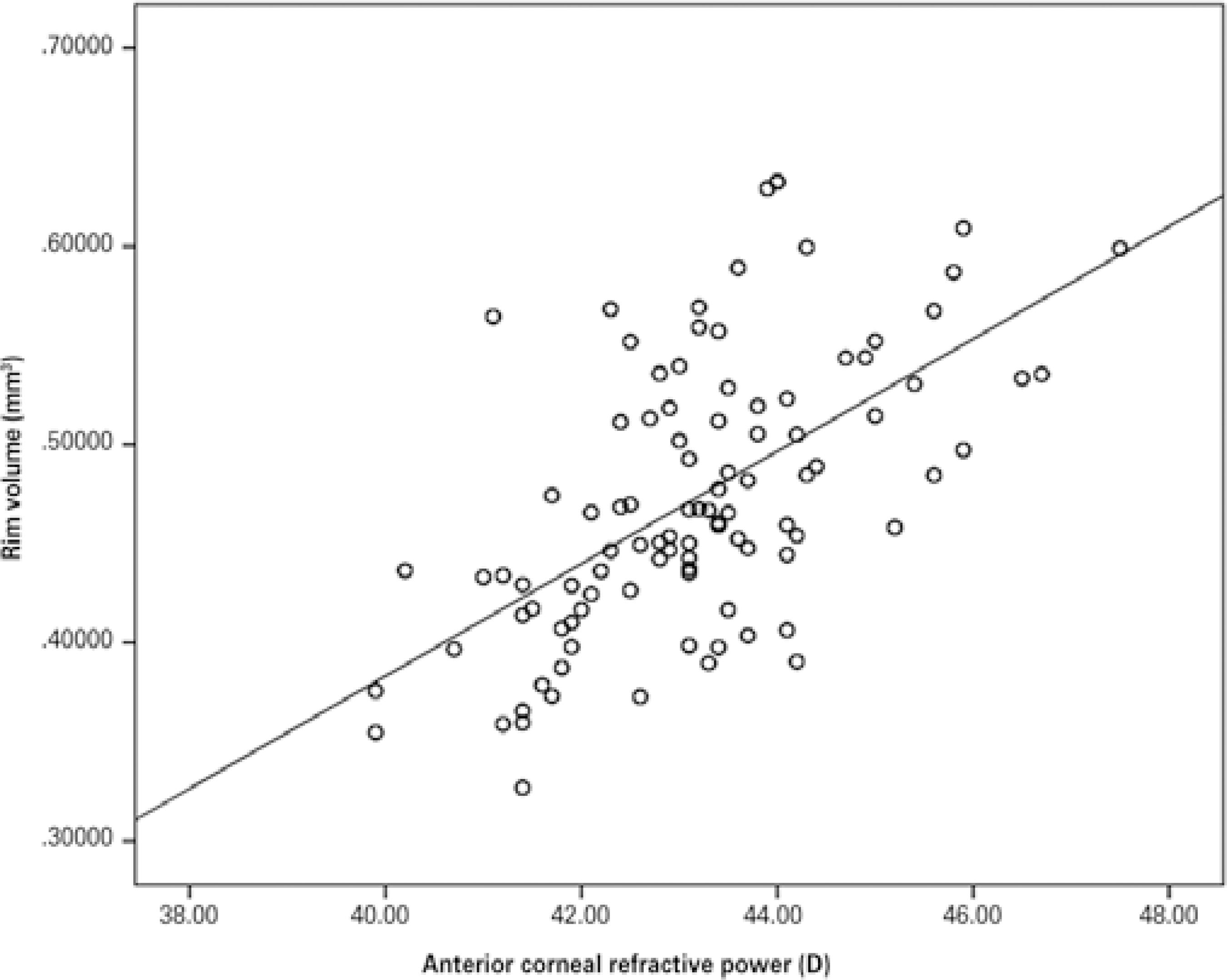
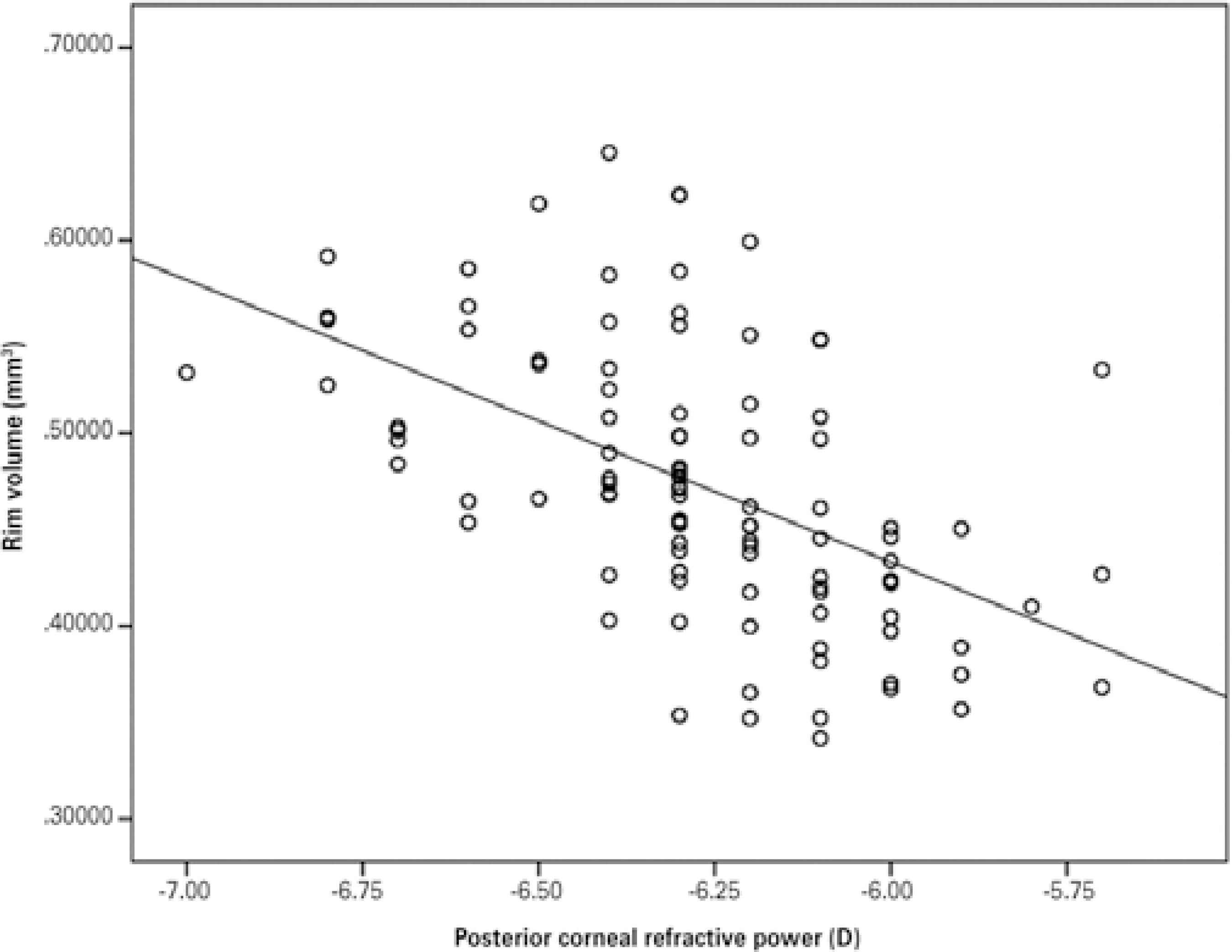
Significant correlations between anterior or posterior corneal refractive power and CA, RA, RV, C/D area, and linear C/D were also apparent after multiple regression analysis. For example, a 1-D increase in anterior corneal refractive power corresponds to a 0.034-mm3 increase in RV. Correlations between anterior and posterior corneal refractive power and RV were shown on the basis of the scatterplot distribution (Figures 1 and 2).
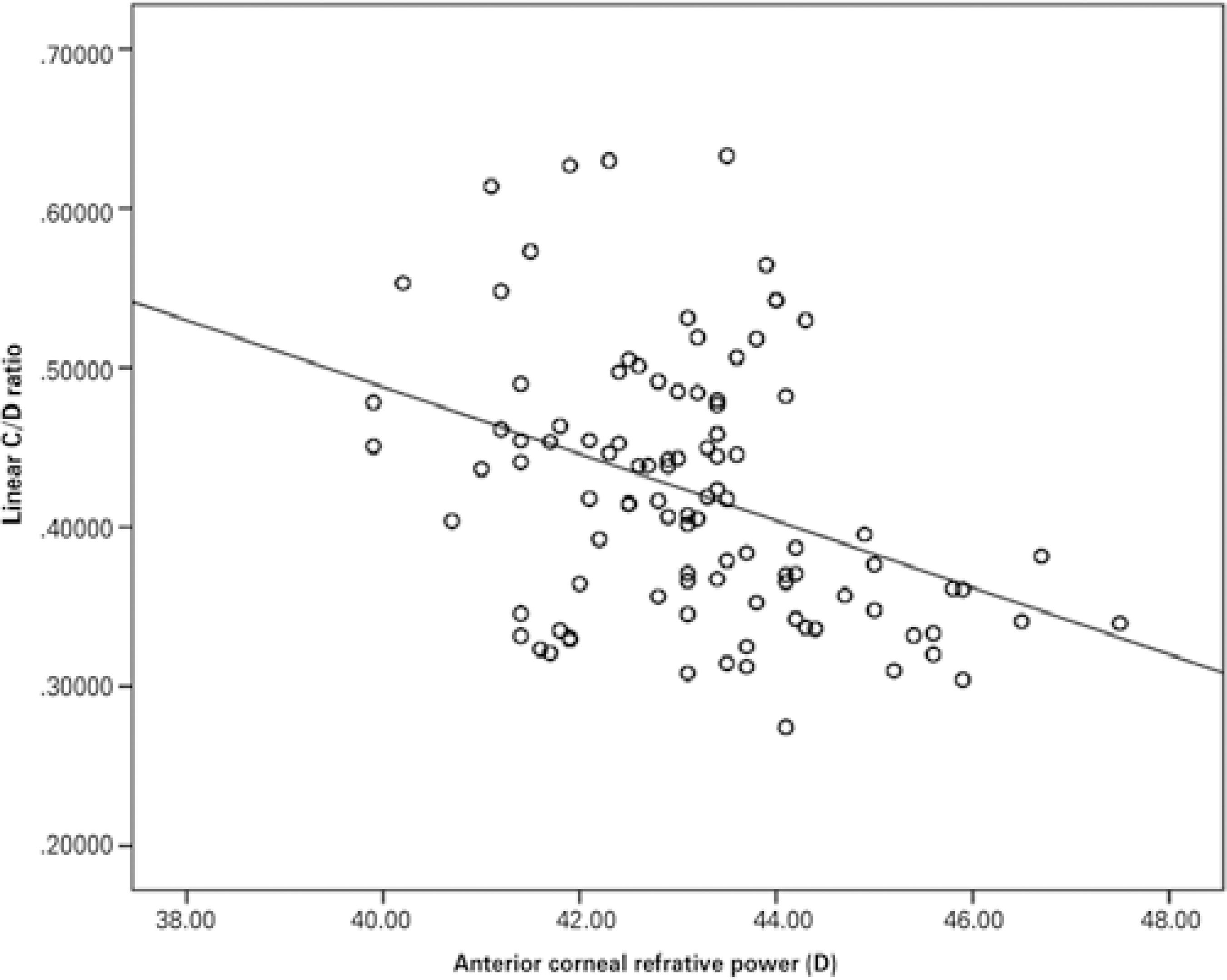
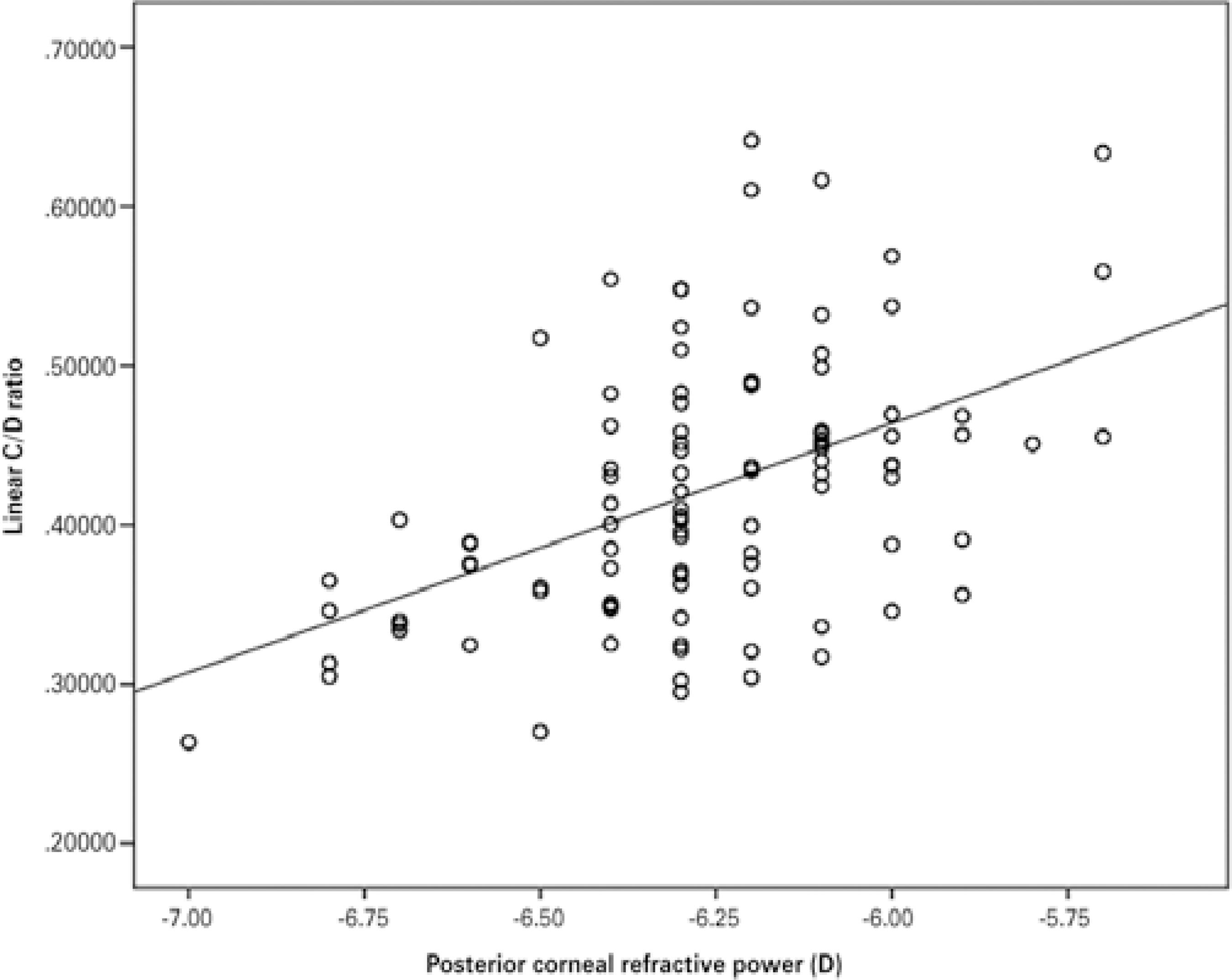
CV and CD measurements showed significant relationships with none of the corneal parameters. As seen in table 3, none of the anterior segment parameters except refractive power of the cornea (both anterior and posterior) correlated with C/D (C/D area and linear C/D). In multivariate regression models, a 1-D increase in anterior corneal refractive power was associated with a 0.022 decrease in linear C/D (Figure 3). Posterior corneal refractive power was also strongly correlated with linear C/D (Figure 4).
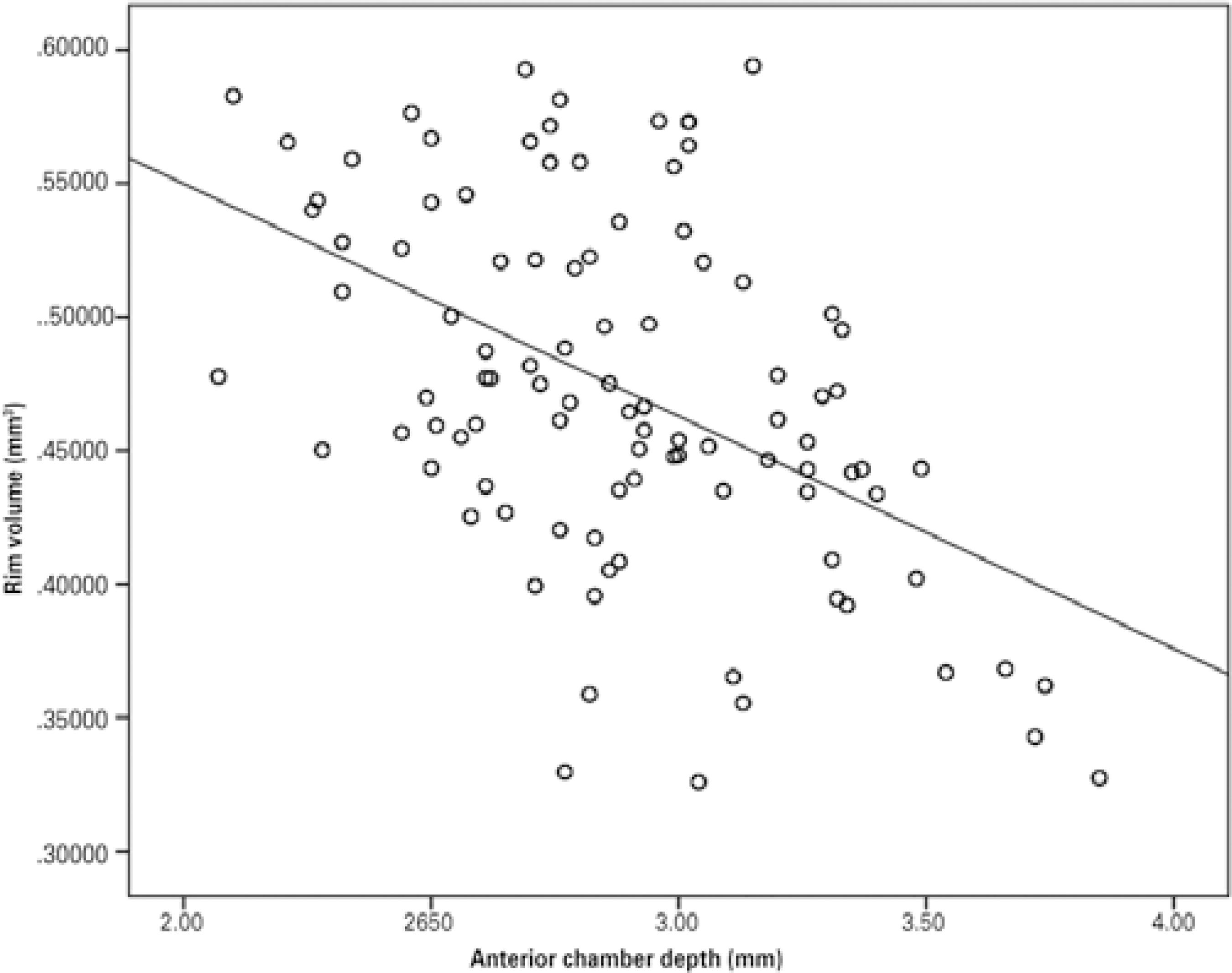
Pearson’s partial correlation coefficient showed a statistically significant negative correlation between ACD and DA (p=0.001, r=-0.228). ACV was also negatively correlated with DA (p=0.001, r=-0.230). Table 4 shows the partial correlation coefficient between ACD measurements and ONH parameters. Only RV showed significant associations with depth (p<0.001, r=-0.321) and volume (p<0.001, r=-0.324) of the anterior chamber. We also found significant negative correlations of ACV and ACD with RV in multivariable regression analysis. According to our analyses, a 0.1-mm increase in ACD corresponds to a 0.015-mm3 decrease in RV (Figure 5).
Table 4 Partial correlation coefficients between anterior chamber and optic nerve head parameters after eliminating influence of age and optic disc area of the participants
| Parameter | Cup area (mm2) | Rim area (mm2) | Cup volume (mm3) | Rim volume (mm3) | C/D area ratio | Linear C/D ratio | Mean cup depth (mm) | Max. cup depth (mm) |
|---|---|---|---|---|---|---|---|---|
| Anterior chamber depth (mm) | ||||||||
| r | 0.109 | -0.112 | 0.063 | -0.321 | -0.099 | 0.093 | -0.048 | -0.073 |
| p | 0.130 | -0.120 | 0.380 | <0.001* | -0.160 | 0.190 | -0.500 | -0.310 |
| Anterior chamber volume (mm3) | ||||||||
| r | 0.122 | -0.135 | 0.035 | -0.324 | -0.138 | 0.124 | -0.021 | -0.035 |
| p | 0.090 | -0.060 | 0.620 | <0.001* | -0.060 | 0.060 | -0.770 | -0.620 |
*statistically significant.
According to the results of multivariate analyses, CD measurements (mean and maximum) were the only ONH parameters that were not correlated with anterior segment parameters.
DISCUSSION
The thickness and biomechanical properties of the cornea have been of interest as important risk factors for the development of glaucomatous optic nerve damage(1,8-10). In view of the potential clinical importance of ONH parameters for glaucomatous optic neuropathy, we undertook the current study to assess the relationship between anterior segment and ONH parameters in healthy, nonglaucomatous subjects.
Some studies reported no correlation between optic disc parameters and corneal measurements or optic disc parameters and ACD(11). However, in the present study we have demonstrated a statistically significant negative correlation between corneal thickness and optic DA. Therefore, it can be concluded that eyes with thicker corneas have smaller discs. Moreover, DA was negatively associated with corneal volume. The association between corneal parameters and optic disc morphology can be explained by the embryologic relationship between the OHN and the cornea, since both the corneal stroma and the optic disc lamina cribrosa differentiate from the neural crest(4). Moreover, DA was negatively associated with corneal volume. We also found negative correlations among ACD, ACV, and DA and found that eyes with deeper anterior chambers had smaller ONHs.
Several studies have yielded inconsistent results on the relationship between corneal characteristics and optic disc parameters. In our previous study in which CCT was measured by ultrasonic pachymeter in healthy eyes, we noted an inverse correlation between CCT and optic DA(12). Moreover, we found negative correlations between CCT and RA as well as RV, and RNFL cross-sectional area. Pakravan et al. reported a similar negative relationship in POAG patients(13). Insull et al. also observed an inverse relationship between optic DA and corneal thickness in a combined group of glaucoma patients and healthy subjects; however, this relationship was not significant when the results were evaluated separately for the glaucoma patients and the control subjects(14). Moreover, such inverse correlations could not be confirmed in some studies. In a population-based study, no significant relationships between CCT and optic disc parameters were observed(15). Bourne et al. reported no association between DA and CCT(11). In contrast, a recent study revealed statistically significant positive correlations between CCT and DA, RA, and RV in normal subjects (16).
Optic disc size is an important parameter in the susceptibility of axonal damage in glaucoma. In the Blue Mountains Eye Study, eyes with glaucoma were found to have larger optic discs than nonglaucomatous eyes and those with ocular hypertension(17). It has been hypothesized that the strength of the lamina cribrosa might be correlated with optic DA. In large discs, a higher lamina cribrosa pore-to-disc area ratio and thinner connective tissue support provide less tissue support. Conversely, when disc size is decreased, the pore-to-disc area ratio also decreases, providing greater tissue support against glaucomatous damage(18,19).
If eyes with thin corneas have large discs that may be prone to the effects of increased IOP, eyes with increased corneal thickness may have smaller discs, which may indicate more resistant optic disc laminae. However, in previous histomorphometric studies, no association was reported between CCT and lamina cribrosa thickness(20,21). According to Wells et al., corneal hysteresis, but not CCT or other anterior segment parameters, was associated with the increased deformation of the optic nerve surface during transient elevations of IOP(22).
It has been reported that increased vertical and horizontal C/D ratio is a risk factor for the development of POAG(1). In our present study, we found a significant relationship between corneal refractive power and C/D. Statistically significant negative correlations were observed between anterior corneal refractive power and linear C/D and C/D area ratios (i.e., the flatter the cornea, the larger the C/D ratio). Posterior corneal refractive power, which is negative, was positively correlated with C/D. Among the anterior segment parameters, only corneal volume had a significant correlation with C/D.
The possibility of a correlation between optic nerve shape and corneal curvature has also been suggested. A previous study reported that an abnormally shaped optic nerve was strongly related to corneal astigmatism(23). Our results are in good agreement with the results of the study by Jonas and Königsreuther, in which large optic discs were found in eyes with flat corneas(24). Similarly, a clinical observational study noted large optic discs with low keratometric readings (diopters)(25). Kim et al. also reported that eyes with large, flat corneas had large C/D(26). Nevertheless, no study has assessed the relationship between corneal refractive power and the risk of glaucoma. Further studies are needed to clarify whether corneal refractive power is a risk factor for glaucoma.
In a population-based study in which the anterior segment OCT and optic disc photographs were used, shallow ACD was associated with a small optic disc(27). Interestingly, we found statistically significantly smaller optic discs in eyes with deep anterior chambers. Moreover, we found significant negative correlations between anterior chamber parameters and optic disc rim parameters.
Our study showed that corneal volume was significantly correlated with almost all ONH parameters except RV. Simirlaly, RV was significantly correlated with almost all anterior segment parameters (except corneal volume). However, the interpretation of these correlations is unclear.
Because this was a hospital-based study, the question arises of how much the results can be generalized. Moreover, the cross-sectional design of the study and its modest sample size may affect the validity of our conclusions and their significance. Nevertheless, our findings may be helpful in understanding the relationship between corneal and optic disc parameters.
The results of our study suggest that anterior segment parameters, especially the thickness, volume, and refractive power of the cornea, may be associated with some important ONH parameters, such as DA, RA, and C/D. These results may support the hypothesis that there is a structural relationship between the cornea and the optic disc. Our findings also show that the relationship between the cornea and glaucomatous optic neuropathy could be more complex than the role of CCT itself in glaucoma.

