INTRODUCTION
Dengue fever is a viral disease transmitted by a mosquito bite. It is considered the most important of the viral diseases transmitted by mosquitos, with more than 100 million cases reported per year, and poses a risk to more than 2.5 billion people worldwide. Since dengue fever is endemic in most tropical and subtropical areas, it is considered a global public health problem1,2.
Dengue virus (DENV) is a single-stranded RNA-enveloped virus. It belongs to the Flavivirus genus of the family Flaviviridae, and there are four serotypes (DENV 1-4). The virus is transmitted to humans through the bite of infected female mosquitoes. The Aedes aegypti mosquito is the primary vector of this virus1.
Dengue infection presents a usually self-limiting clinical picture characterized by fever, malaise, cephalea, mioarthralgias, and rash. Thrombocytopenia, leukopenia, and hepatitis are frequently found in the laboratory workup for infected patients. In a small percentage of cases, the host's excessive inflammatory response leads to a cascade of cytokine production that results in an increased vascular permeability, with plasma extravasation, hemoconcentration, and in severe cases, shock. The infection caused by one DENV serotype induces long-lasting immunity to the same serotype only and a short-term protection from infection with other serotypes, which, in the long-term, increases the risk of severe reinfection by a different serotype3.
In the last 20 years, an increased number of cases associated with eye conditions have been reported. The more frequent symptom was blurred vision. Maculopathy, macular edema, vasculitis, and optic neu ropathy are the most commonly reported complications4. In 2008, the only report of bilateral acute angle closure associated with den gue fever was published in this journal5. We present a second case of this condition during the course of dengue fever.
CASE REPORT
A 46-year-old female arrived at the emergency ward, suffering from ocular pain and a reduction in visual acuity in both eyes of 3 days of evolution.
The patient had hyperthyroidism, and was being treated with methimazole. The patient reported fever within 24 h of the onset of visual symptoms. Blood analysis revealed mild leukopenia and mo derate thrombocytopenia as the only important pathological findings. Dengue fever was suspected by epidemiological linkage; hence, the patient received supportive treatment with metoclopramide and antifebrile drugs.
Ophthalmological examination revealed a visual acuity in both eyes of 20/800, a narrow chamber, moderate corneal edema, and intermediate nonreactive mydriasis in both eyes. Tyndall effect, flare, and posterior synechiae were absent. The intraocular pressure (IOP) was 40 mmHg in the right eye and 36 mmHg in the left eye. Further, fundus examination showed 0.8x0.8 glaucomatous exca vation in each disc. No signs of maculopathy, macular edema, vasculitis, or optic neuropathy were observed, and the patient did not report a history of previous ocular symptoms or pathologies.
A diagnosis of acute angle closure by clinically occludable angle was made. The patient was treated with a combination of 2% dorzolamide/0.5% timolol b.i.d., 0.2% brimonidine b.i.d., and 1% predni solone acetate q.i.d. Bilateral peripheral iridotomy was performed.
Because the patient did not respond to the treatment, ultrasound biomicroscopy images (Sonomed VuMAX™ II UBM; Sonomed Escalon, Stoneham, MA, USA) were requested, which showed a narrow chamber caused by plateau iris configuration (Figures 1 and 2). Be cause of the relatively narrow anterior chamber, the iris-cornea proximity excluded the possibility of performing laser iridoplasty.
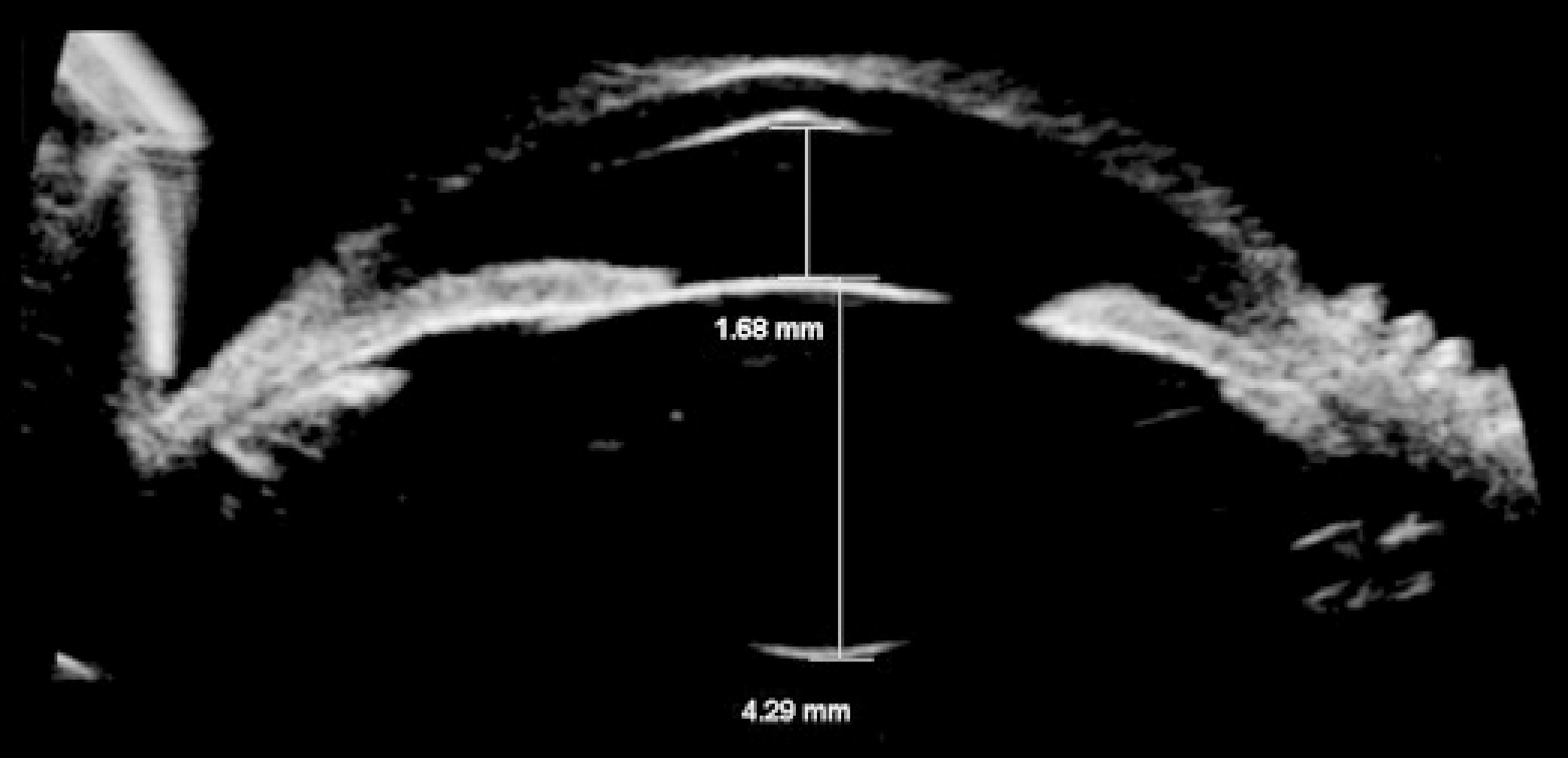
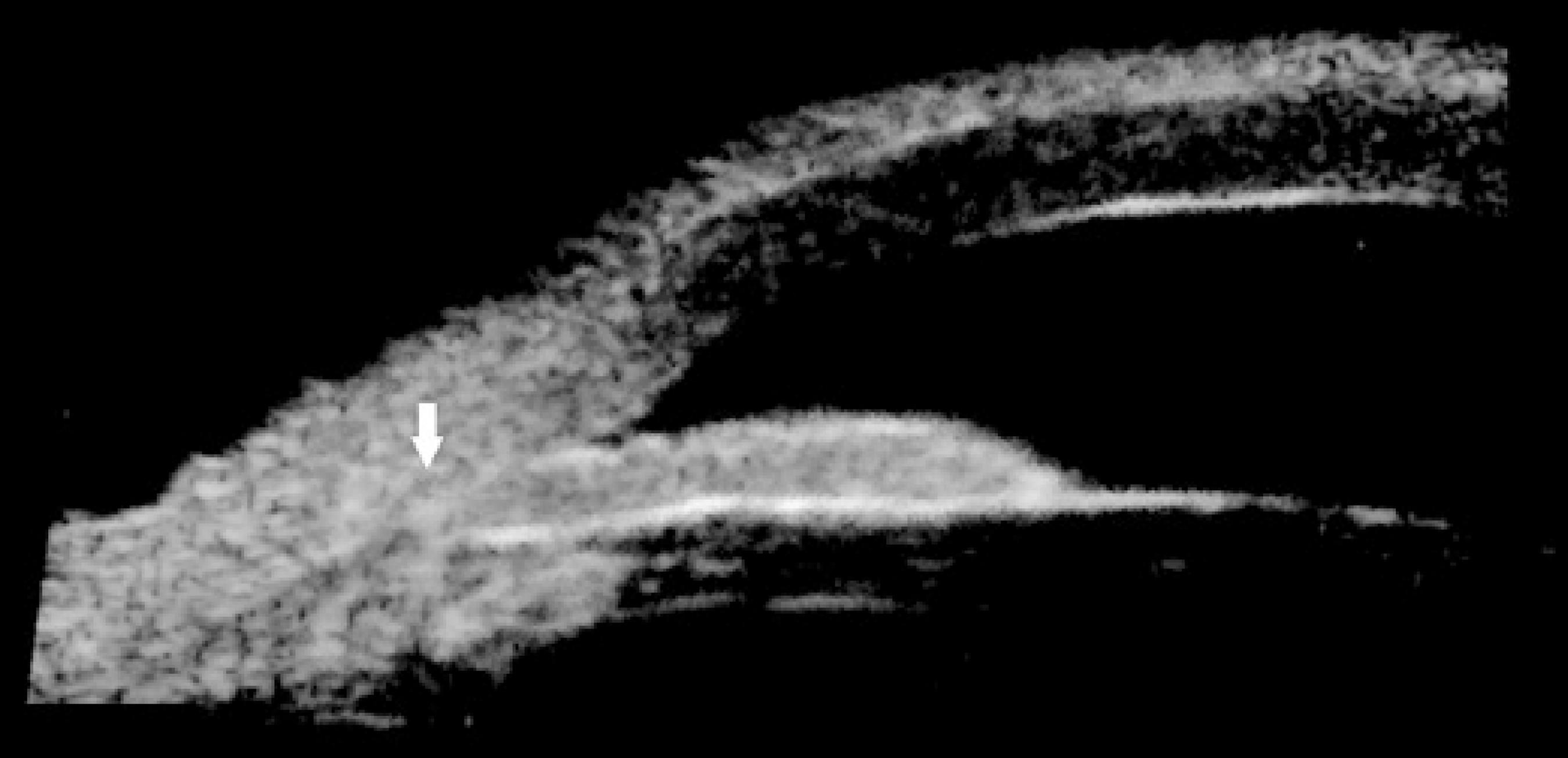
Figure 2 Right eye. Plateau iris configuration: narrow angle (arrow), flat iris, ciliary processes situated anteriorly, and absence of ciliary sulcus.
Serological tests confirmed the presumed diagnosis of dengue infection (positive IgM antibodies for DENV as determined by ELISA). Elective surgery was contraindicated until the thrombocytopenia resolved.
The patient's ocular condition did not improve (IOP of 25 mmHg in both eyes with maximum glaucoma treatment), and she developed chronic angle closure glaucoma in both eyes. The transient thrombocytopenia caused by the DENV infection resolved approximately 20 days after the onset of symptoms, and trabeculectomies were then performed in both eyes, with a delay of 1 month between the surgeries.
Currently, her IOP ranges between 8 and 11 mmHg in both eyes, and she has a visual acuity of 20/20 in OD and 20/30 in OS. Her glaucomatous excavation is 0.8 × 0.8 on the right eye and 0.9 × 0.9 on the left eye.
DISCUSSION
To the best of our knowledge, there has been only one reported case of bilateral angle closure associated with dengue fever5. In both the previously reported case and the present case, the patients presented ocular symptoms within the first 72 h of fever.
Bilateral acute angle closure is an uncommon condition, and has been associated with other conditions such as the use of psychotropic drugs6, general anesthesia7, and snake bites8. Neither the drugs used for the treatment of dysthyroid nor the treatment indicated during the episode of dengue fever were believed to be related to the acute blockage. We believe that the mechanisms of action of these drugs did not provoke this condition6,9.
Capillary leak syndrome occurs in a small percentage of those infected with DENV, and is the leading cause of morbidity and mortality associated with this infection. The plasma levels of vasoactive and proinflammatory cytokines increase in patients with the severe forms of dengue fever, and as a result, vascular permeability increases3.
Several cases of bilateral acute angle closure associated with snake bites have been reported, and all such patients presented symptoms of capillary leak syndrome8. It has been postulated that this syndrome causes ciliary body edema, which triggers acute angle closure. Although the ultrasound biomicroscopy did not confirm the presence of ciliary edema in our case, it is important to note that the biomicroscopy was performed after starting medical treatment and not at the point of diagnosis.
In the previous report on bilateral acute angle closure in a pa tient with dengue fever, an ultrasound biomicroscopy was not per formed5. The presence of plateau iris configuration in our case could provide information on the pathophysiology of this condition. Plateau iris configuration is likely to cause acute angle closure if ciliary body edema occurs.
An anterior chamber tap for polymerase chain reaction detection of DENV was not performed in our study. Assessment of the presence of the virus in the aqueous humor could potentially result in a better understanding of the pathophysiology of this condition.
CONCLUSION
Acute angle closure is a severe clinical picture of primary or se condary etiology. Bilateral cases are rarely associated with dengue fever, and plateau iris configuration may be related to this association. We believe that capillary leak syndrome may be a potential me chanism in this case. However, there is no evidence that edema of the ciliary body is related to dengue fever in this clinical situation.

