INTRODUCTION
Bilateral acute depigmentation of the iris (BADI) is a rare disorder with unknown etiology. It was described for the first time in Turkey in 2006(1). It occurs more frequently in middle-aged women and is characterized by asymptomatic, bilateral, symmetrical, and simultaneous iris depigmentation with focal or diffuse stromal atrophy(2,3).
Although BADI is not usually associated with atrophy of the iris pigmented epithelium, pigment dispersion in the anterior chamber and pigment deposition in the trabecular meshwork have been reported. The prognosis is generally good and repigmentation can occur spontaneously(3-5).
Here we describe a case of BADI and discuss its main clinical aspects and differential diagnosis.
CASE REPORT
A 26-year-old emmetropic woman presented to our clinic after noticing spontaneous iris color change over the past 2 months. Her personal and family medical histories were negative for eye diseases.
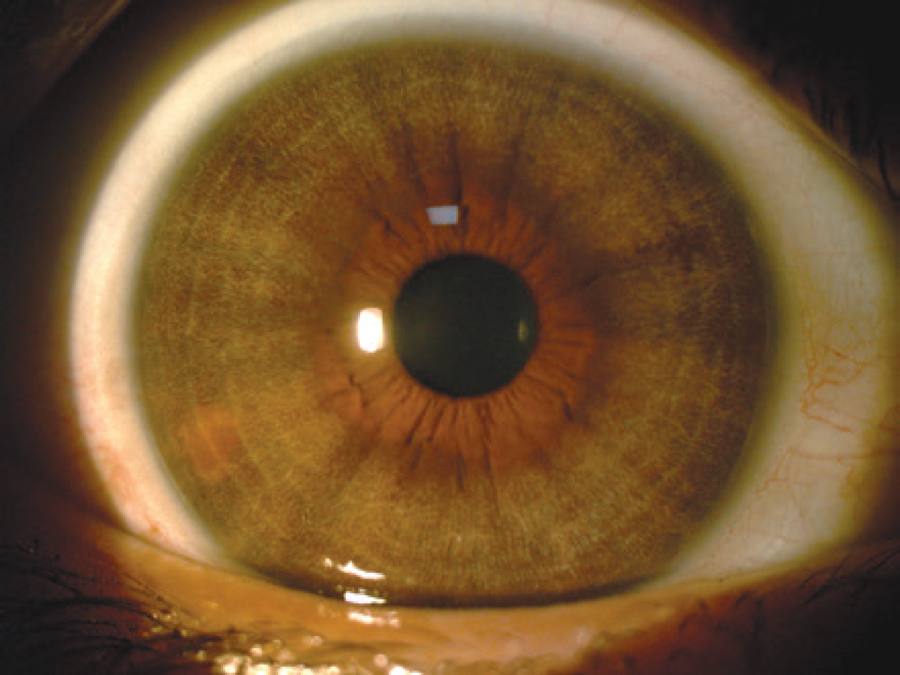
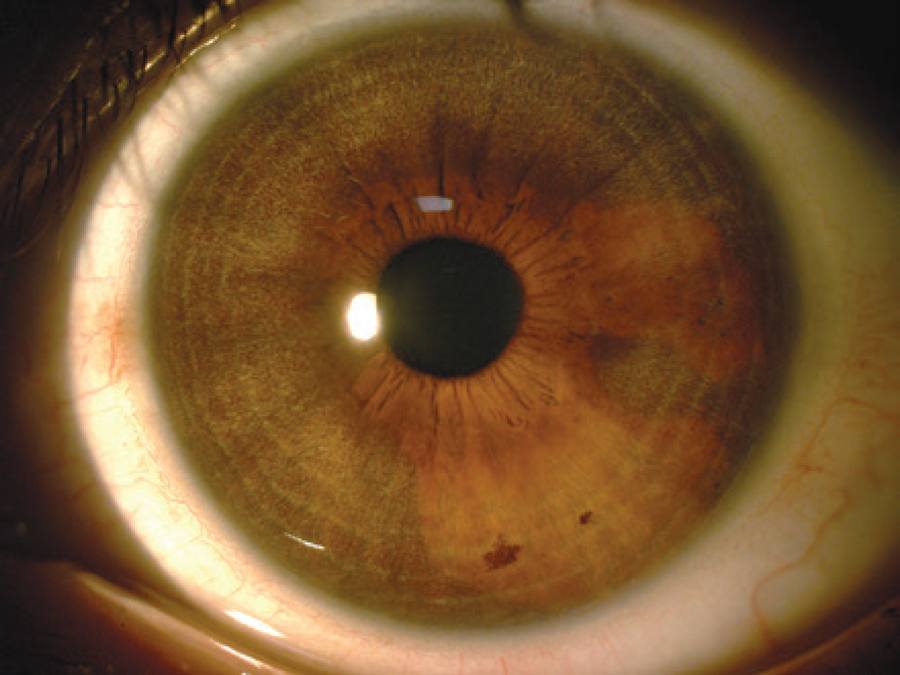
Visual acuity was 20/20 and intraocular pressure was 12 mmHg (at 10:00 am) in both eyes. Biomicroscopy revealed extensive bilateral stromal iris atrophy (Figures 1 and 2). The transillumination test was negative and the lens showed no abnormalities. Gonioscopy showed an open iridocorneal angle with a heavily pigmented trabecular meshwork. The dilated fundus examination was unremarkable in both eyes.
Her serology tests were negative for herpes simplex IgM (herpes simplex IgG positive), hepatitis B and C, and toxoplasmosis. The tuberculin sensitivity test was non-reactive (0 mm).
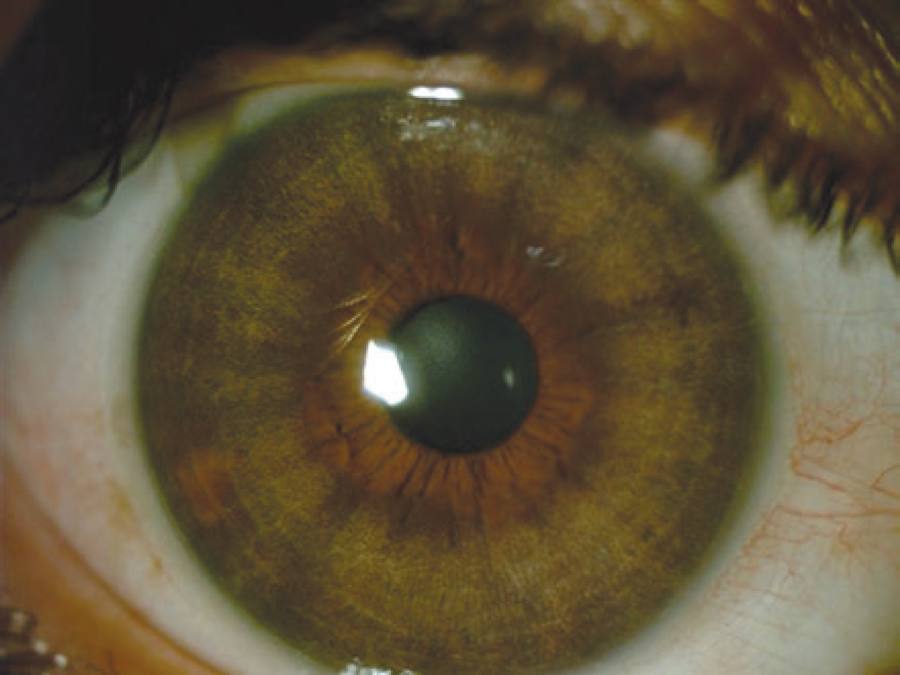
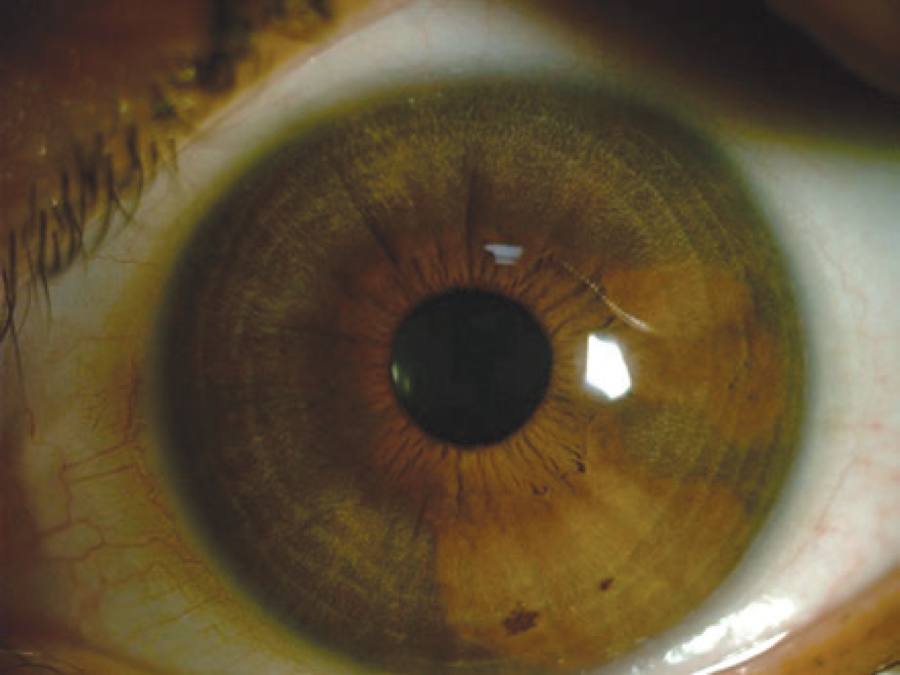
There was no detectable change in the clinical examination after 10 months of follow-up, with maintenance of the pattern of bilateral stromal iris atrophy without any transillumination defects (Figures 3 and 4).
DISCUSSION
BADI is a rare disease with unknown etiology and pathophysiology. The largest published case series of BADI enrolled 26 patients and revealed a previous history of upper respiratory tract infection in 35.8%(5). The authors also suggested an association of BADI with cytomegalovirus infection(5). Another study suggested a possible relationship with the herpes simplex virus and varicella zoster virus(1). Non-infectious etiologies like iris ischemia and neurotrophic mechanisms have also been proposed(3); however, no causative agents have been confirmed yet.
Despite the lack of clinical change after 10 months of follow-up in the case described in this report, other studies have shown that there could be spontaneous resolution over time(3,5).
The differential diagnosis of BADI includes Fuchs heterochromic uveitis, herpetic iridocyclitis, pigment dispersion syndrome, and pseudoexfoliation syndrome(6).
Fuchs heterochromic uveitis is bilateral only in 5%-10% of cases and generally presents with stellate keratic precipitates, mild intraocular inflammation, and cataract(5). Herpetic iridocyclitis generally manifests as a unilateral hypertensive acute anterior uveitis in patients with decreased corneal sensitivity. A subsequent positive transillumination test may be observed as a sequela of the posterior iris pigment epithelium atrophy(7).
The pigment dispersion and pseudoexfoliation syndromes exhibit typical bilateral, irreversible, posterior iris pigment epithelium defects and a positive transillumination test on slit lamp examination(8).
The diagnosis of BADI is based on clinical features and may be challenging due to its rarity and the paucity of noted signs and symptoms. Nonetheless, the clinical findings described in this case were different from those observed in all the entities mentioned above. We believe that the prevalence of this disease may be higher than previously thought and that documenting periodical iris images may help in the diagnosis of suspected cases.
Maestrini et al.(2) described the first Brazilian case of this disease; however, as pointed by experts in this pathology in a letter to the editor(9), deeper analysis of the case demonstrated that the characteristics were closer to another pathological condition called bilateral acute iris transillumination (BAIT). This disorder usually shows atonic dilated pupils and diffuse iris transillumination defects and has a higher incidence of IOP elevation(10). Thus, we believe that our report is the first described case of BADI in Brazil.

