INTRODUCTION
Corneal laceration is one of the leading causes of ocular morbidity(1). Preoperative evaluation of these cases requires meticulous assessment of the etiological agent and extent of the injury. Surgical management of corneal lacerations requires understanding of the wound architecture in order to use appropriate suturing technique to minimize corneal scarring and restore anatomical integrity of the globe. Postoperatively, corneal penetrating injuries have the risk of developing wound leakage, epithelial ingrowth, and excessive corneal astigmatism(2). Wound overriding is a rare but serious complication of the surgical management of ocular penetrating injuries; it is caused by unequal suturing of both sides of oblique corneal wounds.
Ultrasound biomicroscopy (UBM) is a valuable diagnostic tool and is preferred in the detailed evaluation of the anterior segment. UBM has the ability to evaluate anterior segment structures, including the structures posterior to the iris plane. The ability of UBM to completely analyze all structures of the anterior segment makes it a valuable tool in the preoperative evaluation of traumatic cases(3).
In this paper, we present the clinical properties of a case of corneal overriding that developed after surgical management of a case with corneal laceration. We used UBM in the diagnosis of corneal overriding as slit lamp examination did not demonstrate the exact structure of the corneal wound due to severe irregularity and localized corneal edema. To the best of our knowledge, our paper is the first study to demonstrate the use of UBM in the management of abnormal wound architecture of a corneal laceration.
CASE REPORT
A 28-year-old male soldier with a history of penetrating ocular injury caused by a bayonet was referred to our institution. The primary suturation was performed at another institution 2 months ago. Ocular examination of the patient’s left eye was unremarkable with a visual acuity of 20/20. Visual acuity in the right eye was light perception. Slit lamp examination demonstrated a horizontal limbus to limbus laceration between the 3 and 9 o’clock positions in the cornea (Figure 1 A). The corneal wound was sutured with multiple, single, interrupted sutures. There was a 2.5-mm difference between horizontal and vertical white-to-white measurements. There was vitreous hemorrhage and the retina was attached in B-scan ultrasonography.
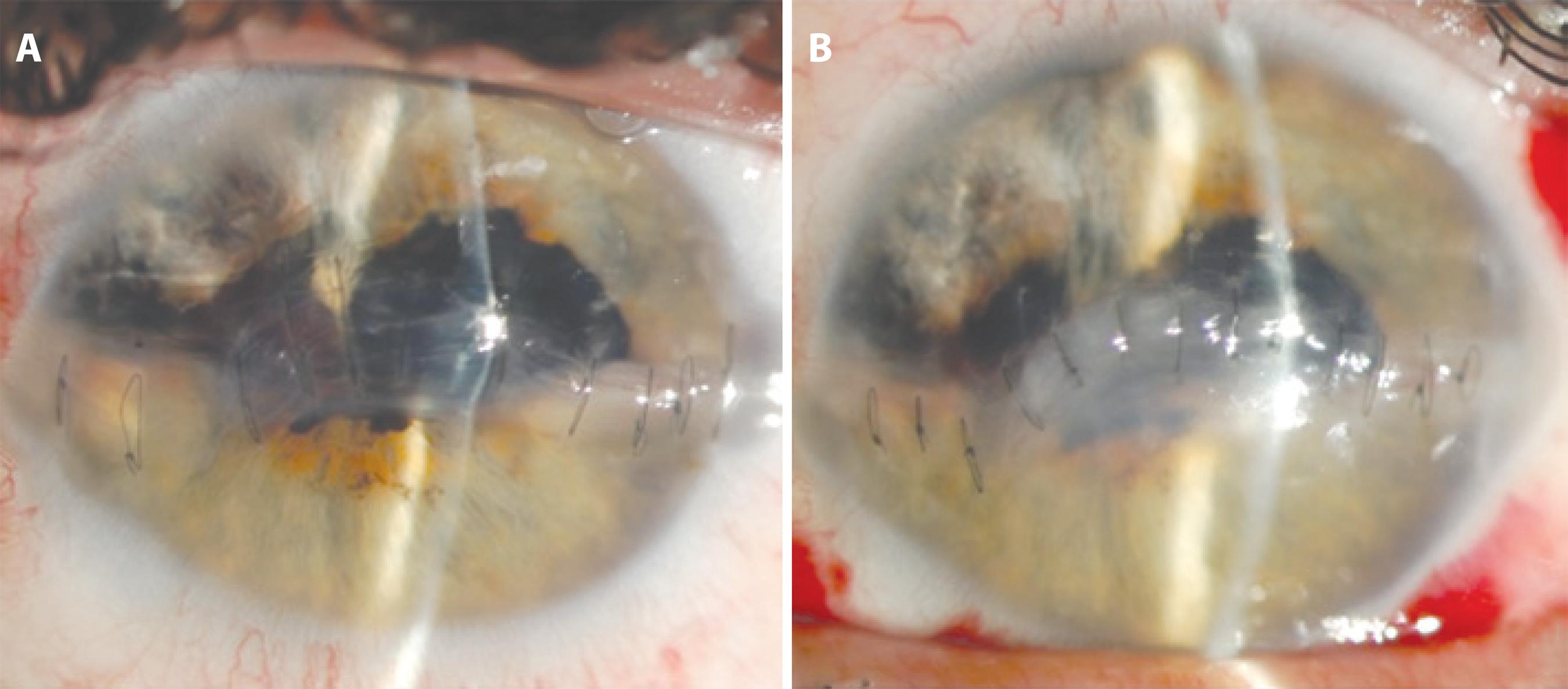
Figure 1 Slit lamp image demonstrating the horizontal laceration with an irregular wound architecture, edema and a significant difference in white-to-white measurements in the horizontal and vertical planes of the cornea (A). Slit lamp image demonstrating favorable wound architecture and substantial recovery in the shape of the cornea after suture enhancement surgery (B).
Slit lamp findings were inconclusive; we used UBM to define the wound architecture in detail. UBM was performed with the patient in the supine position after receiving topical anesthesia. A 50-MHz probe was used with an immersion technique (OTI Scan, Ophthalmic Technologies, Inc.). UBM images demonstrated significant overriding of the corneal wound edges in the central part of the cornea (Figure 2 A). We discussed surgical alternatives with the patient and suggested adjustment of the corneal sutures before starting management of the vitreous hemorrhage.
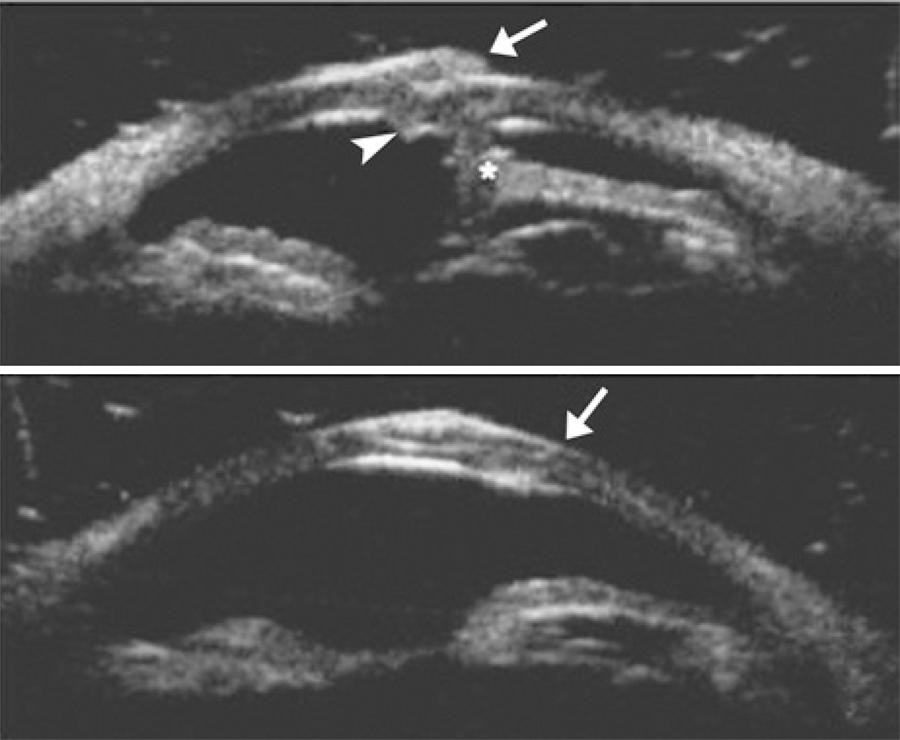
Figure 2 Preoperative ultrasound biomicroscopy of the cornea showing overriding of the wound edges (white arrow demonstrates the upper flap, white arrow head demonstrates the lower flap and asterisks demonstrate the anterior synechia) (A). Postoperative ultrasound biomicroscopy of the cornea showing correct apposition of the wound edges (white arrow indicates the start point of the oblique laceration on the anterior surface of the cornea) (B).
Surgery was performed under general anesthesia. All of the corneal sutures were cut and re-sutured according to the oblique architecture of the wound. The postoperative 6-week visit demonstrated proper alignment of the cornea (Figure 1 B). The structure of the wound edges was analyzed with UBM, demonstrating correct apposition of the corneal wound edges (Figure 2 B). The patient was managed with pars plano vitrectomy, and visual acuity was 20/200 at his last visit at 4 months after the corneal laceration.
DISCUSSION
In our case, we used UBM to demonstrate the exact architecture of the corneal wound. Our patient had a history of ocular penetrating injury with a sharp object; however, slit lamp examination demonstrated a significant difference in white-to-white measurements in the horizontal and vertical planes of the cornea. UBM images helped us exclude corneal tissue loss and changed our surgical approach. After the confirmation of inappropriate suturing of the corneal wound with UBM, we preferred to treat the patient with suture enhancement instead of penetrating keratoplasty.
Anterior segment imaging techniques have limited applications in the management of anterior segment trauma. UBM has been used in several corneal pathologies, including edema, keratoconus, dystrophies, corneal scars, and trauma(4). Anterior segment optical coherence tomography (AS-OCT) and Scheimpflug imaging are alternative imaging techniques that could have been used in our case. AS-OCT is a no-touch technique that could also have been used on our patient(5). With its higher lateral and axial resolution, AS-OCT can provide a more detailed image of the cornea. However, our facility does not have this imaging tool at present, and UBM was found to be quite satisfactory in imaging the corneal wound. Scheimpflug imaging has been used in penetrating injuries to analyze the localization and dimensions of anterior segment foreign bodies(6). However, Scheimpflug imaging has limited imaging quality in corneal opacities and edema, which rendered it unsuitable in our presented case.
The most significant disadvantages of UBM are the need for immersion, the necessity of the supine position, and the need for patient cooperation during image acquisition. UBM is a user-dependent technique and requires an experienced imaging technician. We used the classic “shell and gel technique” in our patient, which requires insertion of a hard plastic shell inside the eye(7). Furthermore, recently introduced disposable ultrasound probe covers eliminate the need for the supine position and insertion of a plastic shell during image acquisition with UBM. In open-globe injuries and uncooperative patients, UBM can be used with disposable probe covers.
Corneal lacerations must be addressed according to the pattern of the wound(8). In oblique corneal lacerations, the length of passage of the suture in the stroma should be equal to the posterior aspect of the corneal laceration. The distance between the needle entry site and the posterior edge of the oblique incision must be gauged from the posterior aspect of the cornea(9).
In conclusion, UBM can be used in preoperative surgical planning of cases with complicated corneal lacerations. It can be used to adjust and enhance wound architecture in eyes with penetrating injuries. UBM with the soft-shell technique has the potential to be used as a pre-surgical diagnostic tool to better understand wound architecture in anterior segment injuries.

