INTRODUCTION
A 28-year-old female was referred to the Universidade Federal de São Paulo (UNIFESP), Department of Refractive Surgery in 2010 for refractive surgery. Her refraction was -3.25 D -0.75 D 160º (OD) and -3.25 D -0.75 D 180º (OS). Corneal topography revealed an asymmetry of less than 0.5 diopters in the left eye (Figure 1). Corneal thickness of right eye was 590 µm and the left eye was 591 µm. We performed wavefront-guided laser-assisted in situ keratomileusis (LASIK) surgery in both the eyes using a Moria M2 microkeratome and LADARVision excimer laser with an ablation depth of 63.8 µm in the right eye and 70.5 µm in the left eye. There were no immediate postoperative complications and the uncorrected visual acuity was 20/20 bilaterally.
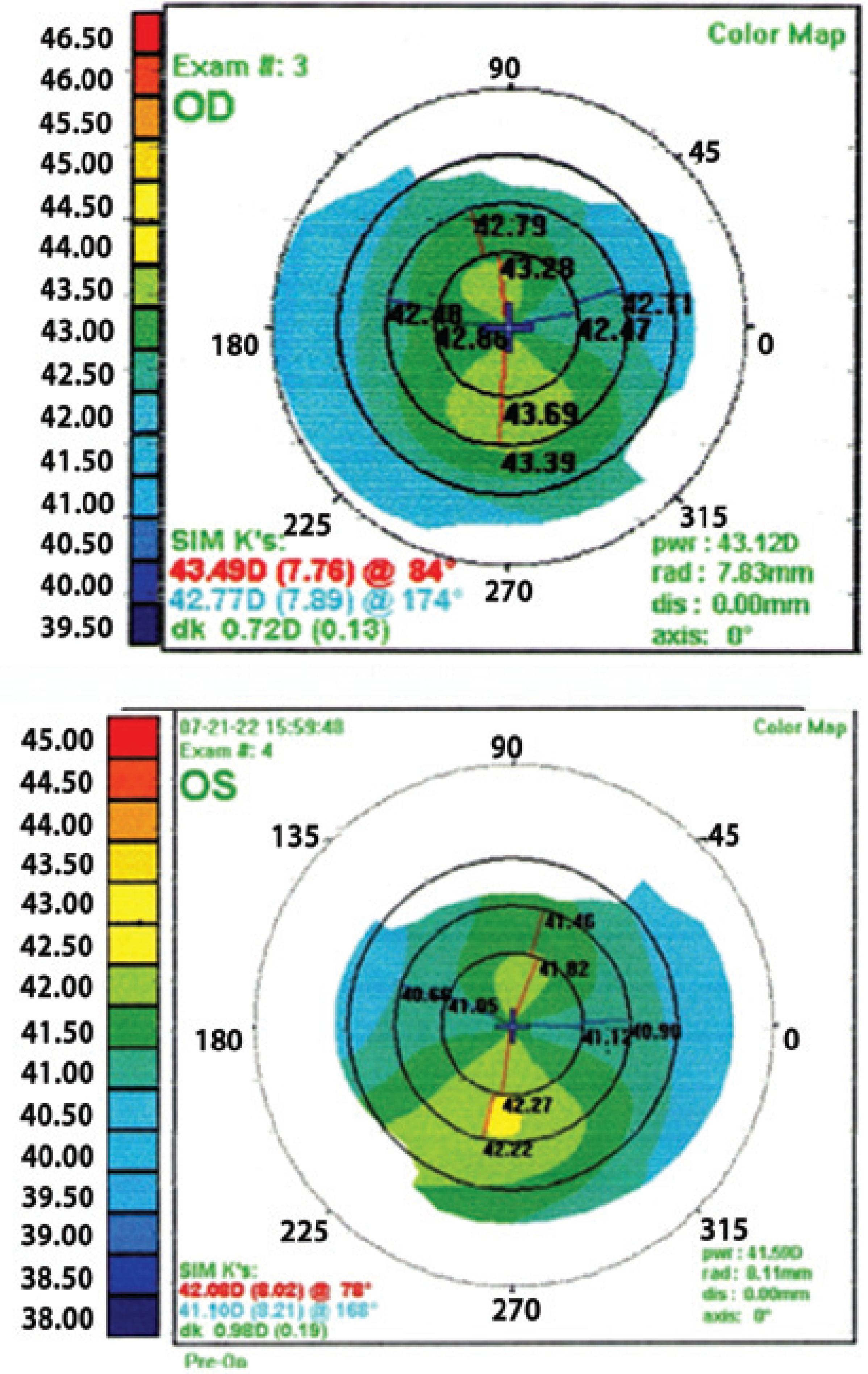
Figure 1 Preoperative corneal topography showing an asymmetry of less than 0.5 diopters in the left eye.
Four months after the procedure, the patient returned with a complaint of decreased visual quality in the right eye. Visual acuity was 20/25 uncorrected and 20/20 with -0.25 D -0.50 D 15º lenses. A comparison of corneal topography findings between postoperative months 1 and 4 (Figure 2) showed inferior corneal steepening (>1 diopter) in the right eye and a diffuse increase in corneal curvature (<1 diopter) in the left eye. Corneal optical coherence tomography (OCT, Figure 3) showed an abnormally thick flap (200-220 µm), whereas aberrometry showed a high RMS (0.84) and an increase in the negative vertical coma. As the patient was scheduled to leave the country within a week for her doctoral studies in Barcelona, we chose to perform under-the-flap intrastromal corneal crosslinking.
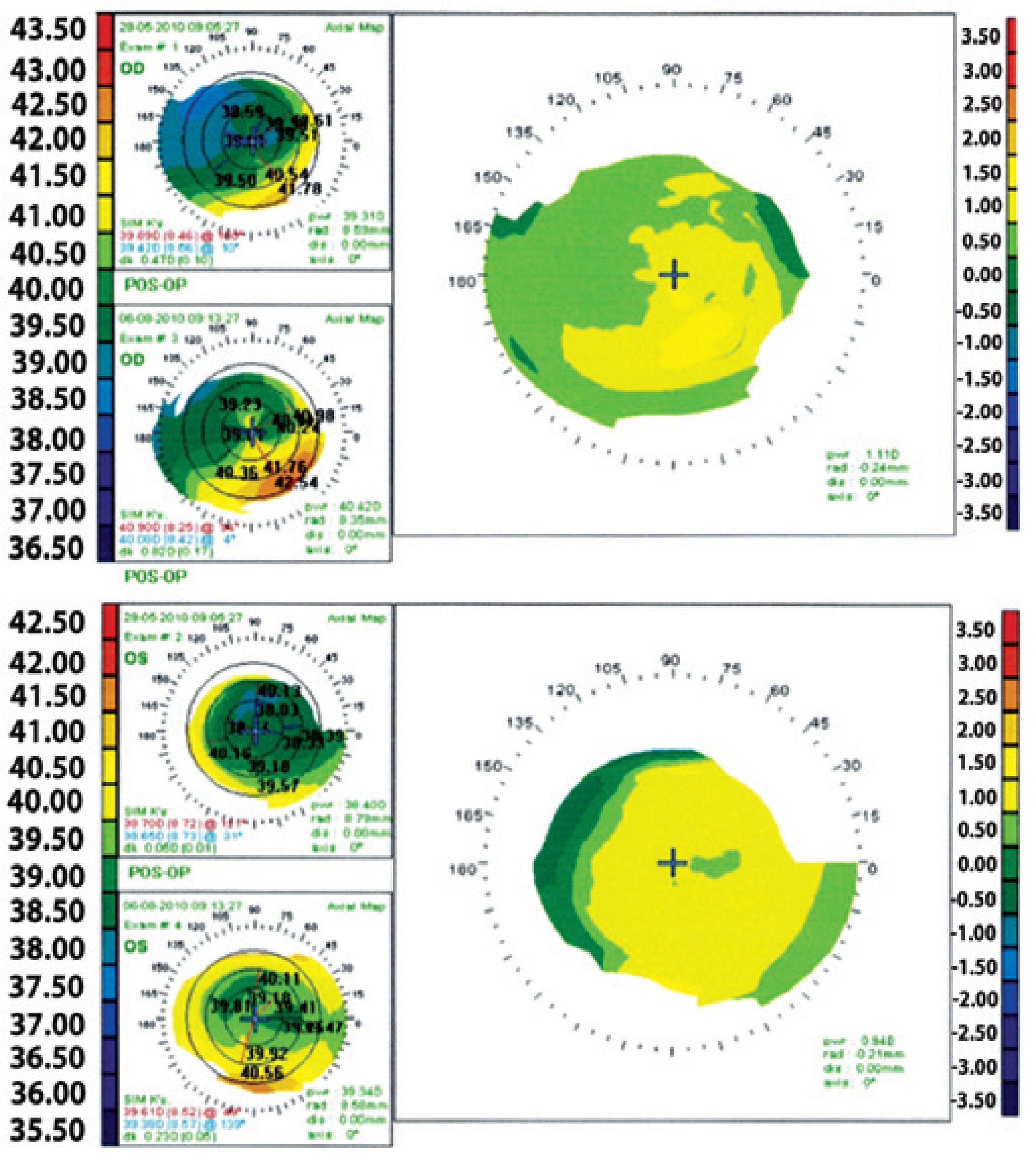
Figure 2 Differential corneal topography between first and fourth month postoperative, showing a steepening in both eyes, more evident in the right eye.

Figure 3 Postoperative optical coherence tomography of the cornea measuring the LASIK flap, showing an abnormally thick flap.
Operative technique
The flap was partially lifted with a corneal spatula so as to enable separation of the stroma above and under the flap, but without lifting the entire flap (Figure 4). A 0.1% riboflavin solution was injected into the stroma at 15-minute intervals for 30 minutes. Crosslinking was performed by standard technique by irradiating with 365 nm UV-A light of intensity 3.0 mW/cm2.
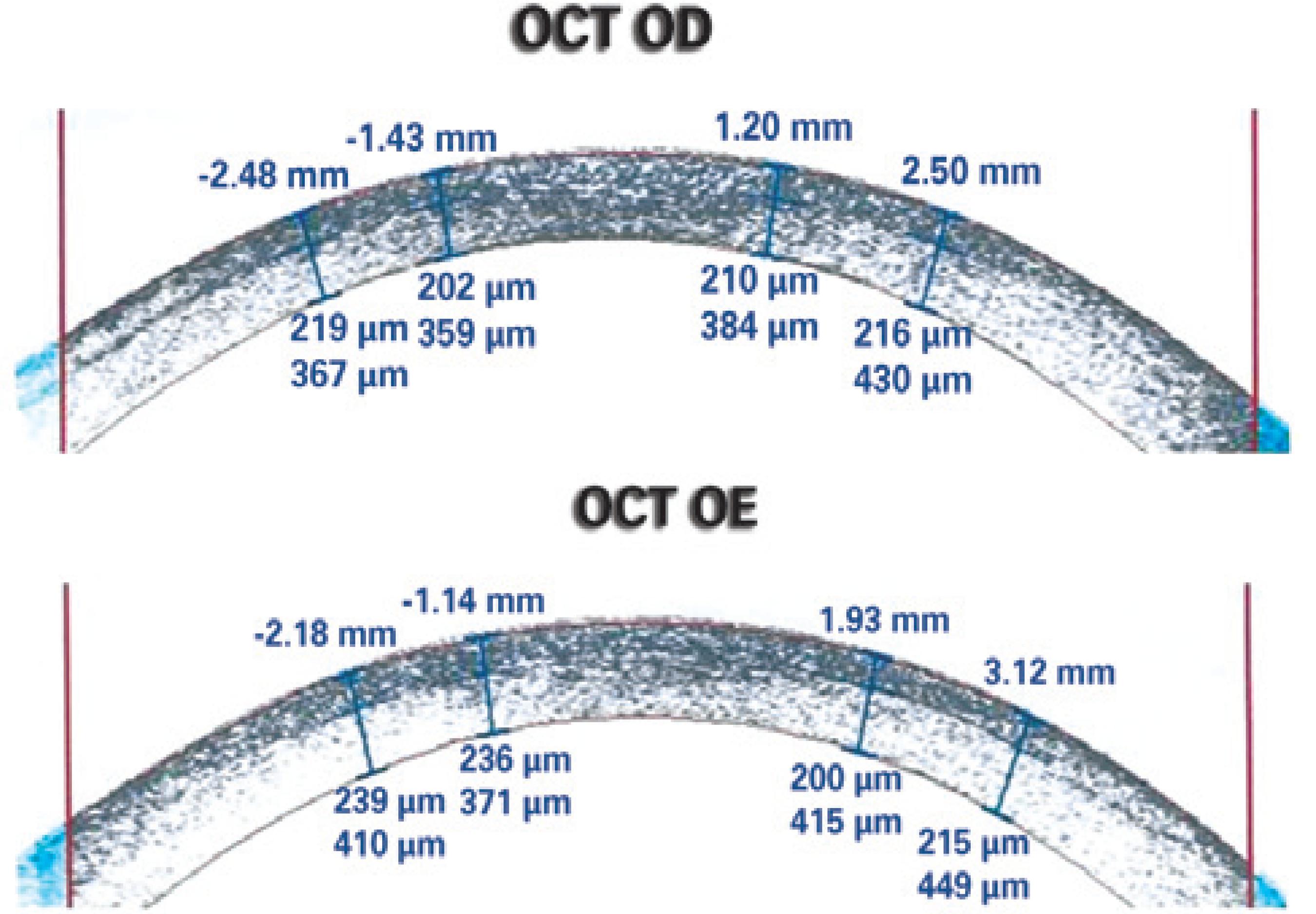
Figure 4 Illustration of the new technique: The flap was partially elevated with a corneal spatula to enable separation of the stroma above and under the flap, but without lifting the entire flap. A 0.1% riboflavin solution was injected into the stroma at 15-minute intervals for 30 minutes and after the crosslinking was performed.
Following surgery, the patient was prescribed with a 3-week course of low-dose corticosteroids (topical fluorometholone), a 1-week course of a fourth-generation quinolone (topical gatifloxacin), and artificial tears for every 6 hours. Three days after the procedure, the uncorrected visual acuity in the treated eye was 20/25, with the typical corneal haze commonly observed in the early postoperative period of crosslinking in the flap area. The patient traveled as originally scheduled with instructions for eye care and under guidance to seek ophthalmologic evaluation in Barcelona.
RESULTS
The patient returned to our service for 1-year follow-up and was asymptomatic. The visual acuity was 20/20 in both eyes (OD: -0.75 D cyl 180º, OS: -0.25 D cyl 140º), and corneal topography showed absence of disease progression bilaterally.
DISCUSSION
Post-LASIK corneal ectasia is a non-inflammatory process that results in deformation of the cornea along with thinning and biomechanical weakening(1-10).
Crosslinking is the gold-standard treatment for progressive corneal ectasia. However, it is often difficult to convince post-LASIK patients with early-stage ectasia to undergo this procedure because of slow and painful recovery periods(1-6).
Some researchers have focused on preventing corneal de-epithelialization so as to achieve efficient and recovery from corneal crosslinking. In one such study, femtosecond laser was used to create a pocket, and riboflavin was administered for only 2 minutes before UV-A irradiation(6). We propose a new technique in which riboflavin is injected under the flap. As a preexisting flap is used, no decrease in biomechanical power of the cornea should occur. The only disadvantage of this technique over the usual procedure is the possibility of epithelial ingrowth, which can be easily avoided if the procedure is performed with care.
Double-blind, randomized, case-control studies are required to provide more reliable data, but this procedure appears simple, safe, and effective technique for management of post-LASIK ectasia.

