Arq. Bras. Oftalmol. 2010; 73 (5): 10.1590/S0004-27492010000500017
Total: 1437
Daniel Hardy Melo1; Paulo de Tarso Ponte Pierre Filho2; Paulo Rogers Parente Gomes2; Andréa Gifoni Siebra de Holanda2; Larissa Pereira da Ponte Amadei3
DOI: 10.1590/S0004-27492010000500017
ABSTRACT
To describe a patient with unilateral metastatic choroidal gastric adenocarcinoma as a first sign of systemic dissemination. A 54-year-old woman presented with a 7-month history of progressive pain and decrease in vision in her left eye. She had undergone total gastrectomy due to gastric adenocarcinoma two years previously. Examination of the left eye revealed an elevated creamy yellow choroidal tumor infiltrating the macular area and extending around the optic nerve head, suggesting metastasis. Treatment was enucleation of the affected eye. There was orbital recurrence of the tumor, leading to exenteration. Orbital and intraocular metastasis are generally associated with a bad prognosis. This patient represents a rare occurrence of metastatic gastric adenocarcinoma to the choroid, developing as a first sign of systemic recurrence.
Keywords: Stomach neoplasms; Adenocarcinoma; Choroid neoplasms; Neoplasm metastasis; Neoplasm recurrence, local; Orbit evisceration; Humans; Female; Middle aged; Case reports
RESUMO
Descrever um paciente com metástase coroidal de um adenocarcinoma gástrico como primeira manifestação de disseminação sistêmica. Uma mulher de 54 anos apresentou história de dor e diminuição progressiva da visão no olho esquerdo há sete meses. Ela havia sido submetida a uma gastrectomia total há dois anos devido a um adenocarcinoma gástrico. Exame do olho esquerdo revelou uma massa coroidal de coloração amarelada infiltrando a área macular e estendendo-se ao redor do disco óptico, sugerindo metástase. Foi realizada enucleação do olho afetado. Posteriormente, houve recorrência orbitária do tumor, levando à exenteração. Metástases orbitárias e intraoculares estão geralmente associadas a um grave prognóstico. Esta paciente representa uma rara ocorrência de adenocarcinoma gástrico metastático para a coróide, apresentando-se como um primeiro sinal de recorrência sistêmica.
Descritores: Neoplasias gástricas; Adenocarcinoma; Neoplasias da coróide; Metástase neoplásica; Recidiva local de neoplasia; Exenteração orbitária; Humanos; Feminino; Meia-idade; Relatos de casos
RELATOS DE CASOS CASE REPORTS
Choroidal metastasis of gastric adenocarcinoma as a first sign of systemic disease recurrence: case report
Metástase de adenocarcinoma gástrico para a coróide como um primeiro sinal de recorrência de doença sistêmica: relato de caso
Daniel Hardy MeloI; Paulo de Tarso Ponte Pierre FilhoII; Paulo Rogers Parente GomesII; Andréa Gifoni Siebra de HolandaII; Larissa Pereira da Ponte AmadeiIII
IPhysician, Otorhinolaryngology and Head and Neck Surgery Department, Santa Casa of Sobral, Sobral (CE), Brazil
IIPhysician, Ophthalmology Department, Santa Casa of Sobral, Sobral (CE), Brazil
IIIPhysician, Oncology Department, Santa Casa of Sobral, Sobral (CE), Brazil
ABSTRACT
To describe a patient with unilateral metastatic choroidal gastric adenocarcinoma as a first sign of systemic dissemination. A 54-year-old woman presented with a 7-month history of progressive pain and decrease in vision in her left eye. She had undergone total gastrectomy due to gastric adenocarcinoma two years previously. Examination of the left eye revealed an elevated creamy yellow choroidal tumor infiltrating the macular area and extending around the optic nerve head, suggesting metastasis. Treatment was enucleation of the affected eye. There was orbital recurrence of the tumor, leading to exenteration. Orbital and intraocular metastasis are generally associated with a bad prognosis. This patient represents a rare occurrence of metastatic gastric adenocarcinoma to the choroid, developing as a first sign of systemic recurrence.
Keywords: Stomach neoplasms; Adenocarcinoma; Choroid neoplasms/secondary; Neoplasm metastasis; Neoplasm recurrence, local; Orbit evisceration; Humans; Female; Middle aged; Case reports.
RESUMO
Descrever um paciente com metástase coroidal de um adenocarcinoma gástrico como primeira manifestação de disseminação sistêmica. Uma mulher de 54 anos apresentou história de dor e diminuição progressiva da visão no olho esquerdo há sete meses. Ela havia sido submetida a uma gastrectomia total há dois anos devido a um adenocarcinoma gástrico. Exame do olho esquerdo revelou uma massa coroidal de coloração amarelada infiltrando a área macular e estendendo-se ao redor do disco óptico, sugerindo metástase. Foi realizada enucleação do olho afetado. Posteriormente, houve recorrência orbitária do tumor, levando à exenteração. Metástases orbitárias e intraoculares estão geralmente associadas a um grave prognóstico. Esta paciente representa uma rara ocorrência de adenocarcinoma gástrico metastático para a coróide, apresentando-se como um primeiro sinal de recorrência sistêmica.
Descritores: Neoplasias gástricas; Adenocarcinoma; Neoplasias da coróide/secundária; Metástase neoplásica; Recidiva local de neoplasia; Exenteração orbitária; Humanos; Feminino; Meia-idade; Relatos de casos.
INTRODUCTION
Metastatic disease is the most frequent intraocular malignancy in adults. Metastatic carcinomas originated from gastro-intestinal tract are rare, occurring in only 4% of cases(1). Intraocular metastasis of gastric adenocarcinoma have been reported in only a few cases in the literature(2-6). A patient with unilateral metastatic choroidal gastric adenocarcinoma that also showed optic nerve invasion is reported. This isolated ocular metastasis was the first manifestation of systemic dissemination of the disease.
CASE REPORT
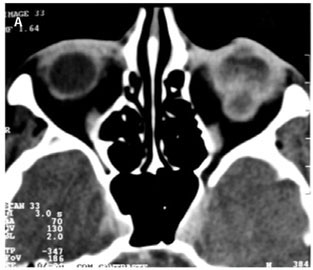
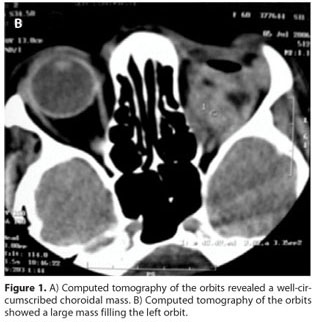
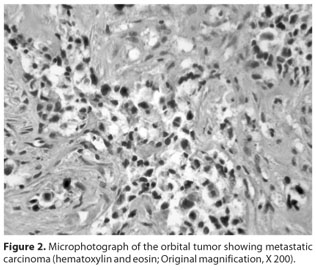
A 54-year-old woman presented to the outpatient ophthalmology department of our hospital in December 2005 with a 7-month history of progressive pain and decrease in vision in her left eye. She had been diagnosed with gastric adenocarcinoma 2 years previously and had undergone total gastrectomy. On presentation, her visual acuity was 20/25 in the right eye and light perception in the left eye. The intraocular pressure was within normal limits in both eyes. There was a relative afferent pupillary defect in the left eye. Anterior segment examination did not reveal any other abnormalities. Fundoscopic examination of the left eye revealed an elevated creamy yellow choroidal tumor infiltrating the macular area and extended around the optic nerve head causing swelling. The vitreous was clear. There was an exudative retinal detachment involving the macula. Ecography disclosed a mass with strong internal echoes in the same region, suggestive of a subretinal tumor. Computed tomography of the orbits demonstrated a large well-circumscribed subretinal mass (Figure 1A). The diagnostic impression on clinical and radiological findings was of a probable metastatic neoplasm. The right eye was unremarkable. Since investigations did not reveal metastasis at any other site, enucleation of the left eye was performed. The histopathological findings of the choroidal metastasis resembled the patient's primary tumor and were consistent with a moderately well-differentiated gastric adenocarcinoma. The patient refused radiation therapy or adjuvant systemic chemotherapy. Eight months after the enucleation, the patient was admitted with intense pain and edema in the left orbit. Computed tomography scan showed a diffuse irregular soft tissue mass involving in the left orbit (Figure 1B). An exenteration of the left orbit was performed without complications and the specimen was submitted to histological evaluation. Histopathological evaluation showed a highly cellular lesion (Figure 2). The cells were predominantly arranged in glands, follicles, and in small clusters and infiltrating tissue planes and vascular structures. On periodic-acid Schiff (PAS) staining, a PAS-positive mucinous secretory material was seen within the gland-like structures. These features were suggestive of a metastatic adenocarcinoma. A systemic work-up revealed multiple retroperitoneal lymph node metastasis and endoscopy showed an irregular narrowing of the esophagojejunal anastomosis, and recurrence of gastric cancer was diagnosed pathologically by biopsy. She was referred to the oncologist for possible palliative therapy. However, she elected not to pursue any form of treatment. The patient subsequently lost follow-up.
DISCUSSION
Malignant tumors from other parts of the body can spread in and around the eye. Breast and lung carcinomas for women and lung and gastrointestinal carcinomas for men most commonly metastasize to the eye and orbit(1). Metastatic disease is usually intraocular, with choroid being the commonest site, though extraocular or orbital cases have been reported(1,7). In others cases similar to our patient, choroidal metastasis were the first sign of a disseminated disease(4-5).
The most common presenting symptoms and signs of ocular metastasis are ocular pain, exophthalmos, retinal detachment, mass lesion, uveitis, secondary glaucoma, and decreased vision(1). The diagnosis can be suggested by prior medical history, ocular evaluation, orbital imaging studies, and systemic evaluation and confirmed with a biopsy and histopathology.
The recognition of metastatic disease and early treatment are important in maximizing the quality of life in these patients. Management of ocular metastasis should take into account the patient's systemic status. Chemotherapy, hormonal therapy, external beam radiotherapy, or plaque radiotherapy may be therapeutic options. Enucleation is reserved for large tumors and relief of pain in blind eyes as a palliative therapy(1).
Orbital and intraocular metastasis are generally associated with a bad prognosis, and most patients succumb to widespread systemic disease within months(2-5). Metastatic involvement of the optic nerve has been shown to have a poor visual prognosis. It is also a rare presentation of systemic carcinoma and in most cases there appears to be a tendency for a direct extension and invasion from a neighbouring peripapillary metastatic tumor(2). The usual presentation in these cases was optic disc swelling. This clinical sign was present in our case.
In conclusion, intraocular metastasis is a significant and under-recognized clinical problem for the practicing ophthalmologist and oncologist. The rare case described in this report highlights the follow-up of a patient who underwent enucleation for a choroidal metastasis with extension into the optic nerve head from gastric adenocarcinoma. In addition, there was orbital recurrence of the tumor, leading to exenteration.
ACKNOWLEDGEMENTS
The authors thank Dr. Rui Celso Mamede for his assistance in the preparation of the manuscript and Dr. José Jackson A. Soares for his comments on histological evaluation.
REFERENCES
1. Shields CL, Shields JA, Gross NE, Schwartz GP, Lally SE. Survey of 520 eyes with choroidal metastases. Ophthalmology. 1997;104(8):1265-76.
2. Imamura Y, Suzuki M, Nakajima KI, Murata H. Gastric signet ring cell adenocarcinoma metastatic to the iris. Am J Ophthalmol. 2001;131(3):379-81.
3. Sung JU, Lam BL, Curtin VT, Tse DT. Metastatic gastric carcinoma to the optic nerve. Arch Ophthalmol. 1998;116(5):692-3.
4. Liszauer AD, Wiens JJ, Brownstein S, Deschenes J. Gastric linitis plastica metastatic to the uvea. Can J Ophthalmol. 1991;26(6):325-7.
5. Sahin A, Kiratli H. Choroidal metastasis as a first sign of recurrence in a patient with gastric adenocarcinoma. Can J Ophthalmol. 2007;42(2):331-2.
6. Saornil MA, Blanco G, Sarasa JL, Gonzalez-Sansegundo C, Rabano G. Isolated metastasis of gastric adenocarcinoma to the retina: first presentation of systemic disease. Acta Ophthalmol Scand. 2004;82(1):86-8.
7. Shields CL, Shields JA, Peggs M. Tumors metastatic to the orbit. Ophthalmol Plast Reconstruct Surg. 1988;4(2):73-80.
 Correspondence address:
Correspondence address:
Paulo Pierre Filho
Av. Gerardo Rangel 801/1001
Sobral (CE) - CEP 62041-380
E-mail: [email protected]
Recebido para publicação em 06.07.2008
Última versão recebida em 21.12.2009
Aprovação em 25.12.2009
The authors have no financial conflict of interest regarding this manuscript.
Work carried out at the Instituto da Visão, Santa Casa de Sobral, Sobral (CE) - Brazil.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.