Arq. Bras. Oftalmol. 2024;87 (1 )
:1-7
| DOI: 10.5935/0004-2749.2021-0061
Abstract
Objetivo: Avaliar o efeito do tabagismo nos desfechos da trabeculectomia.
Métodos: Uma revisão retrospectiva do gráfico de pacientes com glaucoma submetidos à trabeculectomia foi realizada por um único cirurgião entre 2007 e 2016. Os gráficos foram examinados para uma história documentada de condição de fumante antes da cirurgia. Variáveis pré-operatórias clínicas e demográficas e clínicas foram registradas. Os pacientes foram divididos em dois grupos de acordo com sua história de tabagismo em fumantes e não fumantes. Quaisquer Intervenções relacionadas à bolha, por exemplo, injeções de 5-fluorouracil + lise de sutura com laser, ou revisão da bolha realizada durante o período pós-operatório foram observadas. O sucesso foi definido como pressão intraocular > 5 mmHg e < 21 mm Hg sem (sucesso completo) ou com (sucesso qualificado) medicamentos hipotensores oculares. A falha foi identificada como violação dos critérios mencionados acima.
Resultados: O estudo incluiu 98 olhos de 83 pacientes com idade média de 70,7 ± 11,09 anos, sendo 53% (44/83) dos pacientes do sexo feminino. O diagnóstico mais comum foi o glaucoma de ângulo aberto primário com 47 casos (47,9%). O Grupo de fumantes incluiu 30 olhos de 30 pacientes. Os fumantes, quando comparados aos não fumantes, apresentaram uma melhor acuidade visual pré-operatória significativamente pior (p=0,038), maior espessura central da córnea (p=0,047) e maior pressão intraocular pré-operatória (p=0,011). A taxa de sucesso de um ano para a cirurgia de trabeculectomia foi de 56,7% no Grupo de fumantes contra 79,4% no Grupo de não fumantes (p=0,020). O tabagismo apresentou razão de chances para falha de 2,95 95% de IC (1,6-7,84).
Conclusão: Os fumantes demonstraram uma taxa de sucesso significativamente menor em um ano após a trabeculectomia em comparação com os não fumantes e uma maior necessidade de intervenções relacionadas à bolha.
Keywords: Glaucoma de ângulo aberto; Trabeculectomia; Pressão intraocular; Tabagismo; Tabaco/efeitos adversos; Acuidade visual
Arq. Bras. Oftalmol. 2025;88 (2 )
:1-9
| DOI: 10.5935/0004-2749.2023-0326
Abstract
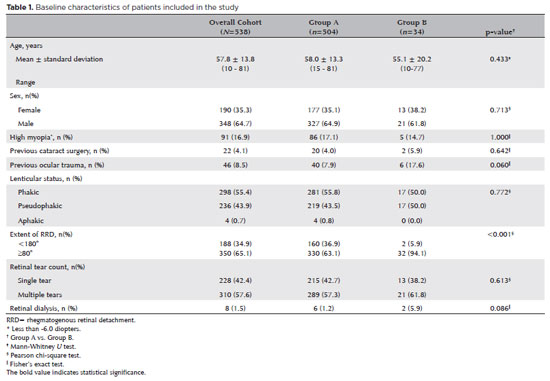
PURPOSE: To evaluate the predictive value of initial intraocular pressure difference of the detached and fellow eyes of patients with complex rhegmatogenous retinal detachment on postoperative persistent ocular hypotony.
METHODS: This retrospective observational study included 538 eyes of 538 unilateral complex rhegmatogenous retinal detachment patients with a proliferative vitreoretinopathy grade of C-1 or higher, treated with silicone oil endotamponade following pars plana vitrectomy. The patients were divided into Group A (patients having silicone oil removal without ocular hypotony; n=504) and Group B (patients with persistent ocular hypotony following silicone oil removal [n=8, 23.5%] and with retained silicone oil [n=26, 76.5%] due to the risk of persistent ocular hypotony; total n=34). Ocular hypotony was defined as an intraocular pressure of <6 mmHg on two or more occasions. Patients' demographics, including age, sex, and follow-up time, and ocular characteristics, including ocular surgical and trauma history, initial and final best-corrected visual acuity, intraocular pressure and initial intraocular pressure difference of the detached and fellow eyes, and anatomical success rates and postoperative complications, were retrospectively collected from the electronic patient files.
RESULTS: The initial intraocular pressure was significantly lower in the detached eyes of Group B than in Group A (8.3 ± 3.5 vs. 12.9 ± 3.3, p<0.001). Also, the initial intraocular pressure difference was significantly higher in Group B than in Group A (8.9 ± 3.2 vs. 2.2 ± 2.7mmHg, p<0.001). The receiver operating characteristic curve analysis showed that the cutoff value of the initial intraocular pressure difference was 7.5mmHg for the risk of persistent ocular hypotony. The most influential factors on postoperative persistent ocular hypotony in the binary logistic regression analysis were the initial intraocular pressure difference and the need for a retinectomy.
CONCLUSION: In eyes with complex rhegmatogenous retinal detachment treated with pars plana vitrectomy and silicone oil tamponade, the initial intraocular pressure difference could be of value in predicting postoperative persistent ocular hypotony and could guide surgeons on the decision of silicone oil removal.
Keywords: Hypotony; Intraocular pressure; Pars plana vitrectomy; Retinal detachment; Silicone oils; Ocular hypotension; Visual acuity
Arq. Bras. Oftalmol. 2025;88 (5 )
:1-8
| DOI: 10.5935/0004-2749.2024-0098
Abstract
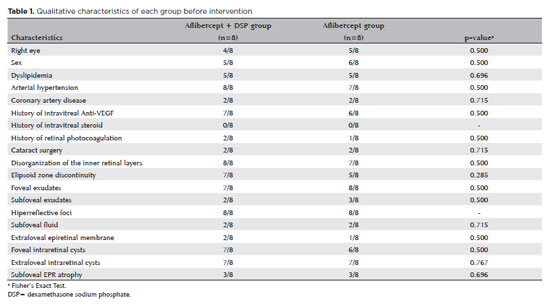
PURPOSE: To compare the short-term (3-month) outcomes of intravitreal aflibercept injections versus intravitreal aflibercept combined with dexamethasone sodium phosphate in treating diabetic macular edema.
METHODS: In this Phase-2 clinical trial, 16 eyes of 16 participants with diabetic macular edema were randomly assigned to one of 2 groups. Participants in the aflibercept monotherapy group received 2 mg of intravitreal aflibercept (0.05 mL), while those in the combination therapy group received 2 mg of intravitreal aflibercept (0.05 mL) plus 0.04 mg dexamethasone sodium phosphate (0.01 mL). Identical injections were repeated after 30 and 60 days. The primary outcome was the change in central macular thickness, as measured by optical coherence tomography, from baseline to 1 month after the last injection. Secondary outcomes included changes in best-corrected visual acuity and intraocular pressure over the same period.
RESULTS: The mean baseline central macular thickness was 444 ± 86 μm in the combination therapy group and 394 ± 96 μm in the aflibercept monotherapy group (p=0.293). By day 90, the mean reduction in central macular thickness was significantly greater in the combination therapy group (176 ± 129 μm) compared to the aflibercept monotherapy group (54 ± 49 μm; p=0.034). Best-corrected visual acuity also improved significantly more in the combination therapy group, with a median gain of 0.31 ± 0.16 LogMAR, whereas the aflibercept monotherapy group experienced a minimal change (−0.06 ± 0.13 LogMAR; p=0.020). Intraocular pressure remained stable in both groups, with no significant difference (p=0.855). None of the participants developed elevated intraocular pressure (>21 mmHg) or required ocular hypotensive medications. No significant ocular or systemic adverse events were reported.
CONCLUSION: The addition of dexamethasone sodium phosphate to the standard intravitreal aflibercept regimen for diabetic macular edema can improve short-term structural and functional outcomes.
Trial registration: Brazilian Clinical Trials Registry (RBR-7468j4q)
Keywords: Diabetic macular edema; Aflibercept; Dexamethasone sodium phosphate; Intravitreal injection; Visual acuity; Central macular thickness; Intraocular pressure
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
10-tab01.jpg)
01-fig01.jpg)
02-fig01.jpg)
03-fig01.jpg)
02-fig01.jpg)

08-fig01.jpg)
13-fig01.jpg)
12-fig01.jpg)
01-fig01tb.jpg)