Arq. Bras. Oftalmol. 2023;86 (2 )
:105-112
| DOI: 10.5935/0004-2749.20230037
Abstract
Objetivo: Avaliar os fatores que influenciam o ganho visual após vitrectomia via pars plana para hemorragia vítrea em pacientes com retinopatia diabética proliferativa.
Métodos: Foi realizado um estudo retrospectivo de 172 olhos de 143 pacientes consecutivos com diabetes mellitus entre janeiro de 2012 e janeiro de 2018. Dados demográficos, achados oftalmológicos, detalhes da cirurgia e resultados visuais foram coletados através de consulta aos prontuários dos pacientes. A principal medida de desfecho foi o aumento da melhor acuidade visual corrigida e as medidas de desfecho secundário foram a recidiva da hemorragia e a ocorrência de complicações.
Resultados: A melhor acuidade visual corrigida aumentou em 103 olhos (59,88%), diminuiu em 45 olhos (26,16%) e permaneceu inalterada em 24 olhos (13,95%). O diabetes mellitus tipo 2 foi significativamente associado a maiores valores finais da melhor acuidade visual corrigida (p=0,0244). O tratamento prévio por fotocoagulação panretiniana com laser ou bevacizumabe intravítreo determinou maiores valores da melhor acuidade visual final corrigida, mas não significativamente (p>0,05). A presença de rubeose iridiana pré-operatória ou de glaucoma neovascular não influenciou os desfechos. A ausência de proliferação fibrovascular com necessidade de dissecção foi um fator significativo para maiores valores da melhor acuidade visual final corrigida (p=0,0006). Ocorreu recidiva da hemorragia em 37,1% dos olhos e não foi influenciada por fármacos antiplaquetários (p>0,05). O glaucoma neovascular pós-operatório foi um fator prognóstico negativo (p=0,0037).
Conclusão: O resultado final da melhor acuidade visual corrigida foi influenciado positivamente pelo diabetes mellitus tipo 2 e pela ausência de proliferação fibrovascular extensa no pré-operatório, e negativamente pela ocorrência de glaucoma neovascular pós-operatório.
Keywords: Retinopatia diabética; Hemorragia vítrea; Vitrectommia; Injeção intravítrea; Acuidade visual.
Arq. Bras. Oftalmol. 2024;87 (1 )
:1-7
| DOI: 10.5935/0004-2749.2021-0328
Abstract
Objetivo: O objetivo deste estudo foi investigar o efeito protetor do cilostazol no desenvolvimento e na evolução da retinopatia diabética em ratos.
Métodos: Sessenta ratos machos foram divididos em 4 grupos: ratos não-diabéticos não-tratados, ratos diabéticos não-tratados, ratos não-diabéticos tratados com cilostazol e ratos diabéticos tratados com cilostazol. A espessura da membrana limitante interna à membrana limitante externa, a camada plexiforme interna, a camada nuclear interna e a camada nuclear externa foram medidas. Para quantificar o grau de perda de células da retina, foi contado o número de núcleos de células por 50 µm de comprimento em secções retinianas.
Resultados: O número de núcleos no GCL foi significativamente maior em Ratos não-diabéticos não-tratados com cilostazol (p<0,05). O número médio de núcleos em Ratos não-diabéticos tratados com cilostazol foi significativamente maior do que em Ratos diabéticos tratados com cilostazol (p<0,05). A contagem média de núcleos em camada nuclear interna e camada plexiforme interna de ratos não-diabéticos tratados com cilostazol foi significativamente maior do que nos outros grupos (p<0,05). A espessura retiniana média total de Ratos não-diabéticos tratados com cilostazol foi significativamente maior do que em Ratos diabéticos tratados com cilostazol e Ratos diabéticos não-tratados (p<0,05).
Conclusão: Os resultados demonstraram que o cilostazol teve um efeito protetor contra as alterações causadas pela retinopatia diabética em ratos diabéticos, diminuindo a perda de células ganglionares e reduzindo a atrofia neurossensorial nas camadas retinianas internas.
Keywords: Cilostazol; Células ganglionares; Retinopatia diabética; Retina; Ratos Wistar.
Arq. Bras. Oftalmol. 2025;88 (6 )
:1-8
| DOI: 10.5935/0004-2749.2025-0077
Abstract
PURPOSE: Standard intravitreal medication dosages are based on an assumed vitreous cavity volume of 4.0-4.5 mL. However, individual variations in vitreous cavity volume may influence both the efficacy and safety of these medications. This study proposes dosage adjustments for intravitreal medications and gases according to axial length and the corresponding vitreous cavity volume.
METHODS: This descriptive study employed reference guidelines that use axial length to estimate the Axial Length-based Volume of the Vitrectomized Space and the Vitreous Volume EXact table for determining dose adjustments across varying eye sizes. Small eyes (axial length 19-22 mm) have an average vitreous cavity volume of 3.5 mL at an axial length of 20.5 mm; standard-sized eyes (22-25 mm) have 4.8 mL at 23.5 mm; large eyes (25-28 mm) have 6.4 mL at 26.5 mm; and extra-large eyes (28-32 mm) have 8.4 mL at 29.5 mm. The medications considered included anti-infectives, anti-VEGFs, complement inhibitors, recombinant proteases, chemotherapy agents, corticosteroids, and medical gases.
RESULTS: Analysis of intravitreal drug concentrations relative to vitreous cavity volume demonstrated notable variability when a standard dose was administered. Small eyes received about 135% of the concentration intended for a standard-sized eye; large eyes received around 75%; and extra-large eyes received under 60%. The recommended dose adjustments are as follows: for small eyes, administer 70-80% of the standard dose; for large eyes, 130-140%; and for extra-large eyes, 170-180%.
CONCLUSIONS: Tailoring intravitreal drug and gas dosages according to axial length and vitreous cavity volume may enhance intraocular drug distribution, potentially improving both safety and therapeutic outcomes.
Keywords: Intravitreal injections; Axial length; Vitreous body; Drug dosage calculations; Pharmacokinetics; Anti-infective agents
Arq. Bras. Oftalmol. 2022;85 (4 )
:370-376
| DOI: 10.5935/0004-2749.20220032
Abstract
Objetivos: Investigar a incidência, fatores de risco e desfechos visuais do desenvolvimento da membrana epirretiniana após reparo do descolamento regmatogênico da retina.
Métodos: Trata-se de um estudo retrospectivo de 309 olhos submetidos à cirurgia inicial para descolamento regmatogênico da retina primário sem complicações. Os exames foram realizados no pré-operatório aos 1, 3, 6 e 12 meses pós-operatórios. Os pacientes foram divididos em dois grupos, dependendo da presença ou ausência de membrana epirretiniana.
Resultados: A incidência de membrana epirretiniana pós-operatória foi de 28,5%; 42,7% desses pacientes apresentaram desenvolvimento grave da membrana epirretiniana e, portanto, foram submetidos à remoção desta membrana. A regressão logística mostrou que as lágrimas retinianas gigantes (RC: 2,66; 95% IC: 1,045 - 6,792, p=0,040) e lágrimas em ferradura (RC: 0,534; 95% IC: 0,295-0,967, p=0,039), foram preditores significativos de membrana epirretiniana pós-operatória. A coloração com acetonida de triancinolona foi significativamente associada à prevenção da membrana epirretiniana (p=0,022). Trinta e quatro pacientes apresentaram acuidade visual melhorada, ou igual, ou acuidade visual final melhor corrigida; 4 olhos foram avaliados na consulta final de acompanhamento e apresentaram redução da acuidade visual melhor corrigida.
Conclusão: Nossa análise demonstra que as lágrimas de ferradura e as lágrimas retinianas gigantes representam fatores de risco para a membrana epirretiniana pós-operatória. A coloração com acetonida de triancinolona teve um efeito preventivo significativo na membrana epirretiniana no pós-operatório. Além disso, uma segunda rodada de vitrectomia pars plana, incluindo remoção da membrana, levou a uma melhora significativa da acuidade visual final melhor corrigida na última consulta de acompanhamento, embora a recuperação tenha sido limitada.
Keywords: Membrana epirretiniana; Descolamento da retina; Recurvamento da esclera; Acuidade visual; Vitrectomia
Arq. Bras. Oftalmol. 2025;88 (4 )
:1-7
| DOI: 10.5935/0004-2749.2024-0229
Abstract
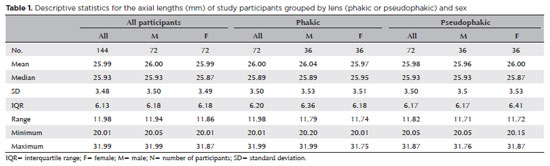
PURPOSE: The volume of the vitreous chamber varies with the size of the eye. The space created in the vitreous cavity by a vitrectomy is called the vitrectomized space. The volume of the vitrectomized space is strongly correlated with the axial length of the eye. This study aims to present guidelines for estimating the using participants stratified by axial length, sex, and history of cataract surgery.
METHODS: This retrospective, observational, cross-sectional study included 144 randomly selected participants who underwent vitrectomies between 2013 and 2023. Before surgery, the axial lengths of participants' eyes were measured using optical biometrics. The axial lengths of the eyes in our sample were between 20-32 mm. In all cases, a complete vitrectomy was performed, followed by complete fluid-air exchange and injection of a balanced saline solution. The volume infused was recorded.
RESULTS: The median (interquartile range; range) volume of the vitrectomized space was 6.1 (3.8; 3.1-11.3) mL in men and 6.1 (3.3; 3.2-11.2) mL in women (p=0.811). The median volume of the vitrectomized space was 5.9 (3.6; 3.1-11.2) mL in patients with phakic lenses and 6.25 (3.6; 3.3-11.3) mL in those with pseudophakic lenses (p=0.533). A positive correlation was found between the axial length and the volume of the vitrectomized space in this sample (r=0.968; p<0.001). In a cubic polynomial regression, the coefficient of determination was 0.948. Similar results were observed in both sexes and in both phakic and pseudophakic patients. The estimated cubic polynomial regression equation for this sample was VVS = 0.000589052857847605 × AL3 - 0.025114926401582700 × AL2 + 0.685961117595624000 × AL - 5.088226672620790000.
CONCLUSION: We developed this axial length estimation of the volume of vitrectomized space as a guideline for the determination of vitrectomized space volume using axial length.
Keywords: Cataract extraction; Retinal perforations/surgery; Epiretinal membrane/surgery; Vitreous body; Axial length, eye; Vitrectomy; Biometry/methods; Diagnostic techniques, ophthalmological; Guidelines as topic.
Arq. Bras. Oftalmol. 2025;88 (4 )
:1-8
| DOI: 10.5935/0004-2749.2024-0277
Abstract
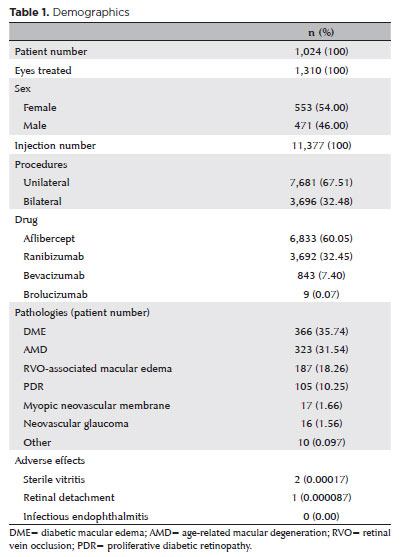
PURPOSE: This retrospective study evaluated the safety and efficacy of real-world antiangiogenic therapy for ocular conditions in the private healthcare sector in southern Brazil.
METHODS: Medical records from patients who underwent intravitreal anti-vascular endothelial growth factor injections over the past 12 years were reviewed retrospectively. Data collection included the primary diagnoses, drugs administered, injection techniques, adverse effects, and treatment efficacy. Efficacy was assessed by comparing pre- and posttreatment visual acuity and central subfield thickness in eyes with followup exceeding 2 years.
RESULTS: A total of 1,024 patients, 1,310 treated eyes, and 11,377 injections were analyzed. The injections included aflibercept (6,833), ranibizumab (3,692), bevacizumab (843), and brolucizumab (9), administered either bilaterally (3,696) or unilaterally (7,681). The most common diagnoses were diabetic macular edema, exudative age-related macular degeneration, retinal vein occlusion related macular edema, and proliferative diabetic retinopathy. No endophthalmitis cases were reported. Vitritis with transient visual acuity loss occurred in two cases following aflibercept injections. One retinal detachment case was successfully treated with vitrectomy. The median number of injections per patient was 6 (IQR [interquartile range], 3–13). Among 445 eyes from 328 patients with followup over 2 years (median, 4.05 years; IQR, 2.89–6.29), there was a significant improvement in best-corrected visual acuity from 0.3 to 0.4 (Snellen) (p<0.001) and a reduction in central subfield thickness from 361 to 267 microns (p<0.001). CST comparisons included patients with age-related macular degeneration, diabetic macular edema, and retinal vein occlusion related macular edema.
CONCLUSION: This real-world study, the largest of its kind in Brazil, confirms the safety and efficacy of antiangiogenic therapies in the southern Brazilian private healthcare system. The findings highlight a low incidence of severe adverse events and outcomes consistent with global studies, supporting the ongoing use of antiangiogenic agents as effective and well-tolerated treatments for various ocular conditions in developing countries.
Keywords: Antiangiogenic drugs; Macular edema; Age-related macular degeneration; Retinal vein occlusion; Patient safety
Arq. Bras. Oftalmol. 2026;89 (1 )
:1-8
| DOI: 10.5935/0004-2749.2025-0025
Abstract
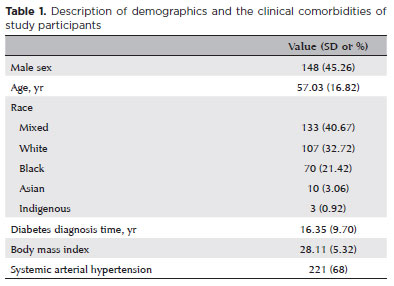
PURPOSE: Diabetic retinopathy screening in low- and middle-income countries is limited by restricted access to specialized care. Portable retinal cameras offer a practical alternative; however, image quality – affected by mydriasis – directly influences the performance of artificial intelligence models. This study evaluated the effect of mydriasis on image gradability and AI-based diabetic retinopathy detection in real-world, resource-limited settings.
METHODS: The proportions of gradable images were compared between mydriatic and non-mydriatic groups. Generalized estimating equations were used to identify factors associated with image gradability, including age, sex, race, diabetes duration, and systemic hypertension. A ResNet-200d model was trained on the mobile Brazilian Ophthalmological dataset and externally validated on both mydriatic and non-mydriatic images. Model performance was evaluated using accuracy, F1 score, area under the curve, and confusion matrix metrics. Sensitivity differences were assessed using the McNemar test, and area under the curves were compared using DeLong's test. The Youden index was used to determine optimal classification thresholds. Agreement between macula- and disc-centered images was analyzed using Cohen's κ.
RESULTS: The mydriatic group demonstrated a higher proportion of gradable images compared with the non-mydriatic group (82.1% vs. 55.6%; p<0.001). In non-mydriatic images, lower gradability was associated with systemic hypertension, older age, male sex, and longer diabetes duration. The AI model achieved better performance in mydriatic images (accuracy, 85.15%; area under the curve, 0.94) than in non-mydriatic images (accuracy, 79.68%; area under the curve, 0.93). The McNemar test showed a significant difference in sensitivity (p=0.0001), whereas DeLong's test revealed no significant difference in area under the curve (p=0.4666). The Youden index indicated that optimal classification thresholds differed based on mydriasis status. Agreement between image fields was moderate to substantial and improved with mydriasis.
CONCLUSION: Mydriasis significantly improves image gradability and enhances AI performance in diabetic retinopathy screening. Nonetheless, in low- and middle-income countries where pharmacologic dilation may be impractical, optimizing model calibration and thresholding for non-mydriatic images is essential to ensure effective AI implementation in real-world clinical environments.
Keywords: Artificial intelligence; Bias; Diabetic retinopathy; Portable camera; Retina
Arq. Bras. Oftalmol. 2025;88 (2 )
:1-9
| DOI: 10.5935/0004-2749.2023-0326
Abstract
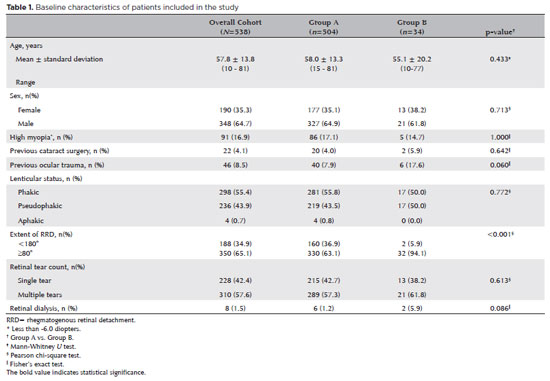
PURPOSE: To evaluate the predictive value of initial intraocular pressure difference of the detached and fellow eyes of patients with complex rhegmatogenous retinal detachment on postoperative persistent ocular hypotony.
METHODS: This retrospective observational study included 538 eyes of 538 unilateral complex rhegmatogenous retinal detachment patients with a proliferative vitreoretinopathy grade of C-1 or higher, treated with silicone oil endotamponade following pars plana vitrectomy. The patients were divided into Group A (patients having silicone oil removal without ocular hypotony; n=504) and Group B (patients with persistent ocular hypotony following silicone oil removal [n=8, 23.5%] and with retained silicone oil [n=26, 76.5%] due to the risk of persistent ocular hypotony; total n=34). Ocular hypotony was defined as an intraocular pressure of <6 mmHg on two or more occasions. Patients' demographics, including age, sex, and follow-up time, and ocular characteristics, including ocular surgical and trauma history, initial and final best-corrected visual acuity, intraocular pressure and initial intraocular pressure difference of the detached and fellow eyes, and anatomical success rates and postoperative complications, were retrospectively collected from the electronic patient files.
RESULTS: The initial intraocular pressure was significantly lower in the detached eyes of Group B than in Group A (8.3 ± 3.5 vs. 12.9 ± 3.3, p<0.001). Also, the initial intraocular pressure difference was significantly higher in Group B than in Group A (8.9 ± 3.2 vs. 2.2 ± 2.7mmHg, p<0.001). The receiver operating characteristic curve analysis showed that the cutoff value of the initial intraocular pressure difference was 7.5mmHg for the risk of persistent ocular hypotony. The most influential factors on postoperative persistent ocular hypotony in the binary logistic regression analysis were the initial intraocular pressure difference and the need for a retinectomy.
CONCLUSION: In eyes with complex rhegmatogenous retinal detachment treated with pars plana vitrectomy and silicone oil tamponade, the initial intraocular pressure difference could be of value in predicting postoperative persistent ocular hypotony and could guide surgeons on the decision of silicone oil removal.
Keywords: Hypotony; Intraocular pressure; Pars plana vitrectomy; Retinal detachment; Silicone oils; Ocular hypotension; Visual acuity
Arq. Bras. Oftalmol. 2024;87 (6 )
:1-7
| DOI: 10.5935/0004-2749.2022-0228
Abstract
OBJETIVO: Avaliar as alterações precoces após a primeira injeção de anticorpos antifator de crescimento endotelial vascular (anti-VEGF) em casos de edema macular secundário à retinopatia diabética e oclusão da veia da retina e a relação entre essas alterações e o resultado a longo prazo.
MÉTODOS: Foram incluídos no estudo pacientes que receberam uma injeção de antifator de crescimento endotelial vascular para edema macular, virgem de tratamento e devido à oclusão da veia retiniana ou a retinopatia diabética. A espessura macular central foi medida no início do tratamento e no 1º dia, 2ª semana e 1º mês após a injeção, bem como na última visita, através de tomografia de coerência óptica de domínio espectral. Definiu-se uma “boa resposta” como uma redução ≥10% na espessura macular central no 1º dia após a injeção. Os pacientes foram reavaliados na última visita com relação à resposta ao tratamento no 1º dia após a injeção, com base em um resultado anatômico favorável, definido como uma espessura macular central <350 µm.
RESULTADO: Foram registrados 26 (44,8%) pacientes com edema macular e oclusão da veia da retina e 32 (55,2%) com edema macular e retinopatia diabética. O tempo médio de acompanhamento foi de 24,0 meses (desvio-padrão de 8,5 meses). Foi observada uma diminuição estatisticamente significativa da espessura macular central após o tratamento antifator de crescimento endotelial vascular tanto em pacientes com edema macular e oclusão da veia retiniana quanto naqueles com edema macular e retinopatia diabética (p<0,001 para ambos). Todos os pacientes com edema macular e oclusão da veia retiniana responderam bem no 1º dia pós-injeção. Todos os que responderam mal no 1º dia pós-injeção pertenciam ao grupo com edema macular e retinopatia diabética (n=16,50%). A presença de manchas hiperrefletivas foi maior nos pacientes que responderam mal do que naqueles que tiveram boa resposta no grupo com edema macular e retinopatia diabética (p=0,03). Um dos 42 (2,4%) pacientes com boa resposta total teve espessura macular central >350 µm, enquanto 5 (31,2%) do total de 16 pacientes com resposta ruim apresentaram espessura macular central >350 µm na última visita (p=0,003).
CONCLUSÃO: O resultado anatômico de longo prazo do edema macular secundário à oclusão da veia retiniana e à retinopatia diabética pode ser previsto pela resposta ao tratamento no 1º dia após a injeção de antifator de crescimento endotelial vascular.
Keywords: Edema macular; Retinopatia diabética; Diabetes mellitus; Oclusão da veia retiniana; Fator A de crescimento do endotélio vascular; Inibidores da angiogênese; Resultado do tratamento
Arq. Bras. Oftalmol. 2024;87 (4 )
:1-5
| DOI: 10.5935/0004-2749.2022-0335
Abstract
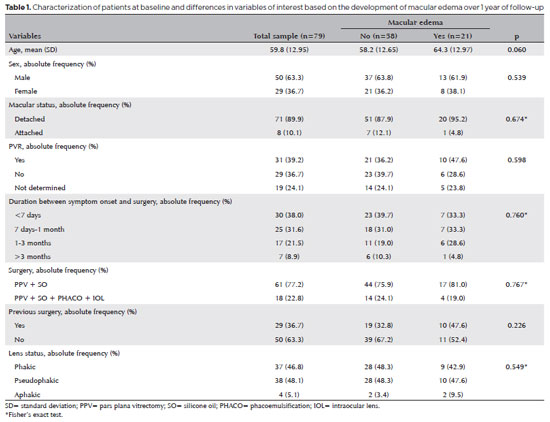
PURPOSE: To clarify the postoperative incidence of macular edema in patients undergoing surgery to repair rhegmatogenous retinal detachment and identify the associated risk factors.
METHODS: In this prospective, observational study, 79 patients who underwent surgery to correct rhegmatogenous retinal detachment using pars plana vitrectomy with silicone oil injection were analyzed. Patients were followed up postoperatively at 7, 30, 90, 180, and 365 days. At each visit, optical coherence tomography was performed to assess the presence or absence of macular edema. were analyzed as possible risk factors for macular edema: age, sex, macular status (attached or detached), presence of vitreoretinal proliferation, history of previous intraocular surgery, reported time of symptoms suggestive of rhegmatogenous retinal detachment up to the date of surgery, and the surgical modality performed.
RESULTS: The 1-year macular edema prevalence rate was 26.6%. In the adjusted analysis, older patients had a higher risk of macular edema, and each 1-year increase in age increased the risk of macular edema by 6% (95% confidence interval = 1.00-1.12). The macular status, vitreoretinal proliferation, the surgical technique used, prior intraocular surgery, and the intraocular lens status were not identified as risk factors. However, the incidence of macular edema increased up to 180 days after surgery, peaking at 10.6%, and then decreased until 365 days after surgery.
CONCLUSION: Macular edema was a common complication after surgery to treat rhegmatogenous retinal detachment, with its incidence peaking between 30 and 180 days after surgery. Age was an important risk factor for macular edema in this cohort.
Keywords: Macular edema; Retinal detachment; Vitrectomy; Tomography, optical coherence; Incidence; Risk factors
Arq. Bras. Oftalmol. 2024;87 (2 )
:1-6
| DOI: 10.5935/0004-2749.2022-0334
Abstract
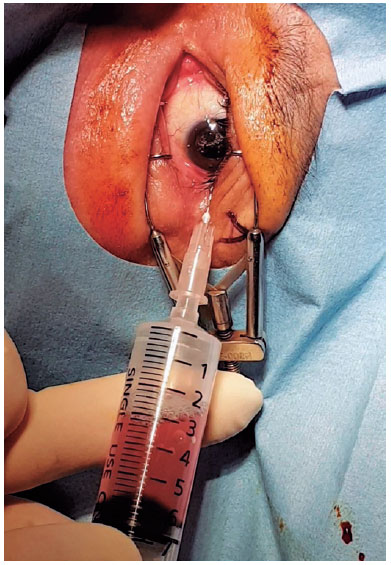
PURPOSE: This study aimed to evaluate the efficacy and clinical outcomes of a one-way fluid-air exchange procedure for the treatment of postvitrectomy diabetic vitreous hemorrhage in patients with proliferative diabetic retinopathy.
METHODS: This retrospective study included 233 patients with proliferative diabetic retinopathy, who underwent vitrectomy. A one-way fluid-air exchange procedure was performed in 24 eyes of 24 (10.30%) patients with persistent vitreous cavity rebleeding after the operation. Preprocedural and postprocedural best-corrected visual acuity values were achieved. Complications occurring during and after the procedure were analyzed.
RESULTS: Significant visual improvement was observed 1 month after the one-way fluid-air exchange procedure (2.62 ± 0.60 LogMAR at baseline vs. 0.85 ± 0.94 LogMAR at postprocedure, p<0.0001). Moreover, 19 (79.17%) eyes needed the procedure once, and 5 (20.83%) eyed had the procedure more than twice. In 3 (12.50%) eyes, reoperation was eventually required because of persistent rebleeding despite several fluid-air exchanges. No complication was observed during the follow-up.
CONCLUSIONS: The one-way fluid-air exchange procedure can be an excellent alternative to re-vitrectomy for patients with proliferative diabetic retinopathy suffering from postvitrectomy diabetic vitreous hemorrhage by removing the hemorrhagic contents directly and achieving fast recovery of visual function without apparent complications.
Keywords: Diabetic retinopathy; Vitrectomy; Vitreous body; Vitreous hemorrhage; Hemostatic techniques
Arq. Bras. Oftalmol. 2024;87 (2 )
:1-5
| DOI: 10.5935/0004-2749.2023-0001
Abstract
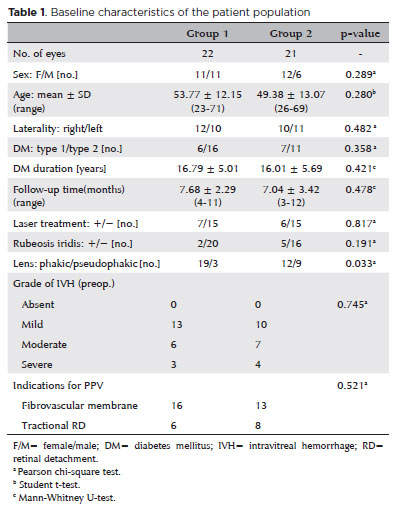
PURPOSE: To investigate the clinical benefits of the co-application of bevacizumab and tissue plasminogen activator as adjuncts in the surgical treatment of proliferative diabetic retinopathy.
METHODS: Patients who underwent vitrectomy for proliferative diabetic retinopathy complications were preoperatively given intravitreal injection with either bevacizumab and tissue plasminogen activator (Group 1) or bevacizumab alone (Group 2). Primary outcomes were surgery time and number of intraoperative iatrogenic retinal breaks. Secondary outcomes included changes in the best-corrected visual acuity and postoperative complications at 3 months postoperatively.
RESULTS: The mean surgery time in Group 1 (52.95 ± 5.90 min) was significantly shorter than that in Group 2 (79.61 ± 12.63 min) (p<0.001). The mean number of iatrogenic retinal breaks was 0.50 ± 0.59 (0-2) in Group 1 and 2.00 ± 0.83 (0-3) in Group 2 (p<0.001). The best-corrected visual acuity significantly improved in both groups (p<0.001). One eye in each group developed retinal detachment.
CONCLUSION: Preoperative co-application of bevacizumab and tissue plasminogen activator as adjuncts in the surgical treatment of proliferative diabetic retinopathy shortens the surgery time and reduces the number of intraoperative iatrogenic retinal breaks.
Keywords: Diabetic retinopathy; Bevacizumab; Plasminogen activators; Vitrectomy; Operative time
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
14-fig01.jpg)
13-tab01.jpg)

03-tab01tb.jpg)
13-tab01tb.jpg)
02-fig01.jpg)
12-fig01.jpg)
03-fig01.jpg)