Arq. Bras. Oftalmol. 2023;86 (4 )
:359-364
| DOI: 10.5935/0004-2749.20230056
Abstract
Objetivo: Comparar as características radiológicas e clínicas do adenoma pleomórfico primário e do carcinoma adenoide cístico da glândula lacrimal.
Métodos: Este estudo revisou retrospectivamente os achados de imagem e os prontuários médicos de casos de adenoma pleomórfico e carcinoma adenoide cístico da glândula lacrimal.
Resultados: Foram avaliados 11 pacientes com adenoma pleomórfico e 16 pacientes com carcinoma adenoide cístico. Não houve diferenças estatisticamente significativas em relação à idade e sexo. Proptose foi o sintoma de apresentação mais comum em ambos os grupos. Os carcinomas adenoides císticos foram mais propensos que os adenomas pleomórficos a apresentarem massas palpáveis, diplopia, dor e perda sensorial, mas essa diferença entre os grupos não foi estatisticamente significativa. Não houve diferenças estatísticas em termos de homogeneidade e indentação do globo ocular entre os dois tipos de tumores em imagens de tomografia computadorizada (p>0,05). Também à tomografia computadorizada, a invasão óssea, a calcificação do tumor e o sinal em cunha foram mais frequentes nos carcinomas adenoides císticos, enquanto a remodelação óssea foi mais frequente nos adenomas pleomórficos, com significância estatística para todas essas manifestações (p<0,05). À ressonância magnética, os adenomas pleomórficos foram significativamente mais propensos a terem margens bem definidas, contornos lobulados, realce heterogêneo pelo contraste e hiperintensidade na ressonância magnética ponderada em T2 (p<0,05).
Conclusão: Ao se diferenciar o adenoma pleomórfico e o carcinoma adenoide cístico da glândula lacrimal, é muito importante avaliar as características radiológicas juntamente com as características clínicas. Os contornos lobulados podem ser uma característica radiológica significativamente distinta em favor do adenoma pleomórfico.
Keywords: Aparelho lacrimal/patologia; Adenoma pleomorfo; Carcinoma adenoide cístico; Tomografia computadorizada por raios x; Imagem por ressonância magnética.
Arq. Bras. Oftalmol. 2025;88 (6 )
:1-9
| DOI: 10.5935/0004-2749.2024-0411
Abstract
PURPOSE: This study evaluated macular thickness using spectral-domain optical coherence tomography in healthy participants from a population-based eye survey.
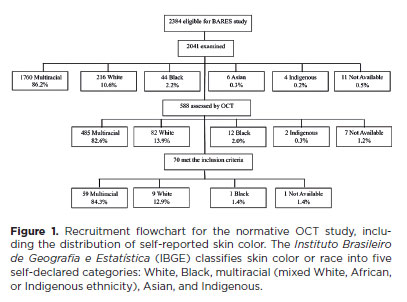
METHODS: The Brazilian Amazon Region Eye Survey was a population-based study assessing the prevalence and causes of visual impairment, blindness, and ocular diseases in adults aged ≥45 years from urban and rural areas of Parintins. A subgroup was selected based on inclusion criteria for both eyes: best-corrected visual acuity ≥20/32, normal eye examination results, and no prior ocular surgery. Scans were performed using the iVue optical coherence tomography device. Measurements were taken from the nine subfields defined by the Early Treatment Diabetic Retinopathy Study, examining the full retina as well as the inner and outer retinal layers. Associations of retinal thickness with age and sex were also analyzed. Statistical significance was set at p≤0.05.
RESULTS: In total, 70 healthy participants (25 males), aged 45–65 years (mean=52 ± 5), were included. Mean central foveal thickness was 248.71 ± 18.73 μm. A significant age-related reduction in macular thickness was observed, particularly in the inner superior parafovea (p=0.036), nasal perifovea (p=0.001), superior perifovea (p=0.028), outer layer of inferior parafovea (p=0.049), and the inferior perifovea of the full retina (p=0.029). Males showed significantly greater thickness in the outer layer, especially in the outer parafovea (p=0.004) and perifovea (p<0.0001).
CONCLUSIONS: This study established normative macular thickness values for healthy older adults in the Brazilian Amazon region using spectral-domain optical coherence tomography. Age and sex were found to significantly influence macular thickness and should be considered when interpreting measurements. These data will support future studies of retinal diseases in this population.
Keywords: Retinal diseases/diagnosis; Macula lutea/pathology; Macular degeneration/diagnosis; Diabetic retinopathy/diagnosis; Vision, low; Vision tests; Tomography, optical coherence/methods; Young adult; Cross-sectional studies; Brazil/epidemiology
Arq. Bras. Oftalmol. 2025;88 (2 )
:1-9
| DOI: 10.5935/0004-2749.2023-0326
Abstract
PURPOSE: To evaluate the predictive value of initial intraocular pressure difference of the detached and fellow eyes of patients with complex rhegmatogenous retinal detachment on postoperative persistent ocular hypotony.
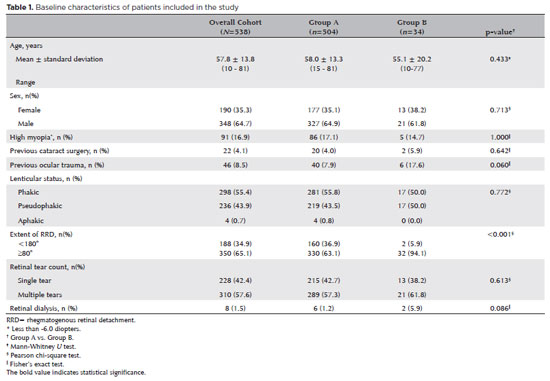
METHODS: This retrospective observational study included 538 eyes of 538 unilateral complex rhegmatogenous retinal detachment patients with a proliferative vitreoretinopathy grade of C-1 or higher, treated with silicone oil endotamponade following pars plana vitrectomy. The patients were divided into Group A (patients having silicone oil removal without ocular hypotony; n=504) and Group B (patients with persistent ocular hypotony following silicone oil removal [n=8, 23.5%] and with retained silicone oil [n=26, 76.5%] due to the risk of persistent ocular hypotony; total n=34). Ocular hypotony was defined as an intraocular pressure of <6 mmHg on two or more occasions. Patients' demographics, including age, sex, and follow-up time, and ocular characteristics, including ocular surgical and trauma history, initial and final best-corrected visual acuity, intraocular pressure and initial intraocular pressure difference of the detached and fellow eyes, and anatomical success rates and postoperative complications, were retrospectively collected from the electronic patient files.
RESULTS: The initial intraocular pressure was significantly lower in the detached eyes of Group B than in Group A (8.3 ± 3.5 vs. 12.9 ± 3.3, p<0.001). Also, the initial intraocular pressure difference was significantly higher in Group B than in Group A (8.9 ± 3.2 vs. 2.2 ± 2.7mmHg, p<0.001). The receiver operating characteristic curve analysis showed that the cutoff value of the initial intraocular pressure difference was 7.5mmHg for the risk of persistent ocular hypotony. The most influential factors on postoperative persistent ocular hypotony in the binary logistic regression analysis were the initial intraocular pressure difference and the need for a retinectomy.
CONCLUSION: In eyes with complex rhegmatogenous retinal detachment treated with pars plana vitrectomy and silicone oil tamponade, the initial intraocular pressure difference could be of value in predicting postoperative persistent ocular hypotony and could guide surgeons on the decision of silicone oil removal.
Keywords: Hypotony; Intraocular pressure; Pars plana vitrectomy; Retinal detachment; Silicone oils; Ocular hypotension; Visual acuity
Arq. Bras. Oftalmol. 2025;88 (2 )
:1-5
| DOI: 10.5935/0004-2749.2024-0113
Abstract
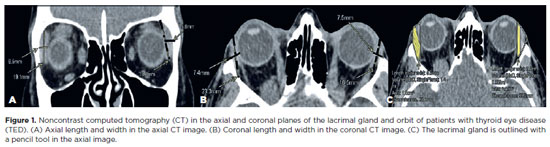
This study aimed to evaluate the morphometric and volumetric dimensions of the lacrimal gland in patients with inactive thyroid eye disease and compare them with the values reported in the literature. This case series evaluated consecutive patients with inactive thyroid eye disease treated at a tertiary eye hospital from 2015 to 2020. The patients' baseline demographics and clinical characteristics were obtained. The axial and coronal length, width, and volume of the lacrimal gland were measured on computed tomography scan images, and the results were statistically analyzed. A total of 21 patients (42 orbits) with inactive thyroid eye disease were evaluated. Their mean age was 49.0 ± 14.6 years, and 12 (57.1%) of them were men. The main complaint was dryness, and the majority of the patients had good vision and mild proptosis. The mean axial length and width of the lacrimal gland were 19.3 ± 3.9 mm and 7.5 ± 2.1 mm, respectively; coronal length and width, 20.4 ± 4.5 mm and 7.5 ± 2.1 mm, respectively; and lacrimal gland volume, 0.825 ± 0.326 mm3. Age, sex, or laterality were not found to be determinants of lacrimal gland enlargement. Patients with thyroid eye disease have enlarged lacrimal gland even in the nonactive phase of the disease multifactorial aspects influence the lacrimal gland in thyroid eye disease, making it difficult to establish a clear correlation with predisposing factors. Further studies are warranted to better understand the association between thyroid eye disease and the lacrimal gland.
Keywords: Graves' ophthalmology; Graves' disease; Lacrimal apparatus; Lacrimal apparatus diseases; X-ray computed tomography
Arq. Bras. Oftalmol. 2024;87 (4 )
:1-5
| DOI: 10.5935/0004-2749.2022-0335
Abstract
PURPOSE: To clarify the postoperative incidence of macular edema in patients undergoing surgery to repair rhegmatogenous retinal detachment and identify the associated risk factors.
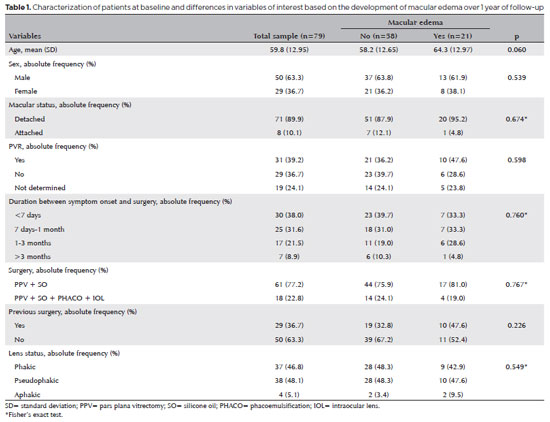
METHODS: In this prospective, observational study, 79 patients who underwent surgery to correct rhegmatogenous retinal detachment using pars plana vitrectomy with silicone oil injection were analyzed. Patients were followed up postoperatively at 7, 30, 90, 180, and 365 days. At each visit, optical coherence tomography was performed to assess the presence or absence of macular edema. were analyzed as possible risk factors for macular edema: age, sex, macular status (attached or detached), presence of vitreoretinal proliferation, history of previous intraocular surgery, reported time of symptoms suggestive of rhegmatogenous retinal detachment up to the date of surgery, and the surgical modality performed.
RESULTS: The 1-year macular edema prevalence rate was 26.6%. In the adjusted analysis, older patients had a higher risk of macular edema, and each 1-year increase in age increased the risk of macular edema by 6% (95% confidence interval = 1.00-1.12). The macular status, vitreoretinal proliferation, the surgical technique used, prior intraocular surgery, and the intraocular lens status were not identified as risk factors. However, the incidence of macular edema increased up to 180 days after surgery, peaking at 10.6%, and then decreased until 365 days after surgery.
CONCLUSION: Macular edema was a common complication after surgery to treat rhegmatogenous retinal detachment, with its incidence peaking between 30 and 180 days after surgery. Age was an important risk factor for macular edema in this cohort.
Keywords: Macular edema; Retinal detachment; Vitrectomy; Tomography, optical coherence; Incidence; Risk factors
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
11-tab01.jpg)
02-fig01.jpg)
02-fig01.jpg)
13-fig01.jpg)
09-fig01.jpg)
08-fig01.jpg)
04-fig01.jpg)
14-fig01.jpg)