Arq. Bras. Oftalmol. 2026; 89 (4): 10.5935/0004-2749.2025-0225
Total: 444
Plínio Augusto Trindade Abreu1; Juan Silva Locks Camargo2; Lais Bomediano de Souza3; José Paulo Cabral de Vasconcelos1, Osias Francisco de Souza1
DOI: 10.5935/0004-2749.2025-0225
ABSTRACT
PURPOSE: To compare the impact of pro re nata and treat-and-extend regimens on quality of life in patients with neovascular age-related macular degeneration.
METHODS: This cross-sectional study included 81 patients with neovascular age-related macular degeneration who completed the National Eye Institute Visual Function Questionnaire-25.
RESULTS: No statistically significant differences were observed between pro re nata and treat-and-extend regimens across quality-of-life domains measured by National Eye Institute Visual Function Questionnaire-25.
CONCLUSIONS: Pro re nata and treat-and-extend regimens demonstrated comparable effects on quality of life in patients with neovascular age-related macular degeneration. Further studies are warranted to determine optimal standardized treatment strategies.
Keywords: Macular degeneration/diagnosis; Fluorescein angiography/methods; Tomography, optical coherence/methods; Macular degeneration/drug therapy; Drug administration schedule; Angiogenesis inhibitors/therapeutic use; Intravitreal Injections; Surveys and question
INTRODUCTION
Age-related macular degeneration (AMD) is a degenerative disorder of the macula that primarily affects the elderly. It is characterized by progressive loss of central vision and is a leading cause of irreversible blindness in developed countries(1,2).
The etiology of AMD is multifactorial, involving both genetic and environmental factors. Major risk factors include advanced age, family history, smoking, prior cataract surgery, and comorbid conditions such as systemic arterial hypertension, cardiovascular disease, and obesity, as well as elevated plasma levels of inflammatory markers(3).
Common symptoms of AMD include reduced visual acuity, metamorphopsia, and paracentral scotomas(4,5). Diagnosis is based on patient history and multimodal imaging, including fluorescein angiography, optical coherence tomography (OCT), and, when indicated, indocyanine green angiography(4,5).
The prevalence of AMD is estimated at approximately 18 million individuals in North America and 67 million in Europe. These numbers are expected to increase further due to demographic shifts and the growing elderly population(6,7).
AMD is a serious condition with significant potential to impair vision-related quality of life (VRQoL)(8). It adversely affects daily activities, mobility, access to health care, work capacity, and participation in cultural and leisure activities such as reading and social interaction. Moreover, it may lead to reduced independence, increased reliance on caregivers, higher healthcare costs, and psychological consequences, including anxiety and depression(9-12).
The standard treatment for the exudative form of AMD —neovascular AMD (nAMD)—is intravitreal injection of antiangiogenic agents(1,2,4). Advances in therapy, particularly the development of anti-vascular endothelial growth factor (anti-VEGF) agents, have significantly improved the prognosis of nAMD, enabling many patients to maintain or even improve visual acuity. Consequently, early diagnosis and adherence to treatment protocols are essential components of patient management. Current efforts focus not only on improving efficacy but also on reducing treatment burden through extended dosing intervals, novel drug delivery systems, and enhanced patient support(2,5).
The most commonly used treatment regimens include fixed monthly dosing, pro re nata (PRN), and treat-and-extend (T&E) strategies(13). Each regimen has distinct advantages and limitations. Monthly dosing provides consistent efficacy but imposes a substantial burden due to frequent clinic visits. The PRN approach reduces the number of injections by administering treatment based on disease activity; however, it requires close monitoring and may increase the risk of undertreatment. In contrast, the T&E regimen individualizes treatment intervals based on patient response, thereby balancing efficacy and convenience. Clinical studies suggest that T&E achieves visual outcomes comparable with monthly dosing while reducing the number of injections and visits, making it a practical and patient-centered approach(14-22).
In recent decades, the number of patients receiving treatment for AMD has increased markedly, driven by improved outcomes and greater awareness of available therapies. Although treatment imposes a considerable burden on patients, their families, and healthcare systems, the clinical benefits generally outweigh these challenges(23-25).
Despite extensive research, most comparisons of treatment regimens focus on clinical outcomes and healthcare perspectives, with limited emphasis on patient-reported outcomes. It remains unclear whether one regimen offers a superior quality of life from the patient’s perspective. This question motivated the present study.
The objective of this study was to compare the impact of PRN and T&E treatment regimens on the quality of life of patients with nAMD using the NEI VFQ-25 questionnaire.
METHODS
A cross-sectional study was conducted to compare the impact of different treatment types on quality of life in patients with nAMD treated at a private clinic, evaluating whether there is a difference in quality of life between patients with exudative AMD managed using PRN and T&E regimens.
A cross-sectional design was chosen because, although the NEI VFQ-25 is sensitive to changes over time, the primary objective was to assess whether the treatment regimen influences quality of life during ongoing anti-VEGF therapy rather than to evaluate temporal changes. A longitudinal design would have required baseline and multiple follow-up assessments, which were not feasible due to resource and time constraints.
Eighty-one patients from a private clinic were selected to participate in the study between September 2022 and February 2023. Individuals diagnosed with nAMD who had received at least 9 months of intravitreal injection treatment were included. Patient inclusion was based on a clinical diagnosis of nAMD, established by an experienced retina specialist using clinical examination and multimodal imaging, including spectral-domain OCT and, when available, fluorescein angiography and/or OCT angiography.
Patients were not allowed to choose their treatment regimen (PRN or T&E), as all were covered by health insurance with different contractual clauses. Therefore, some individuals could only receive injections on a PRN basis, whereas others had access to continuous treatment under the T&E protocol. This restriction resulted in a natural allocation of patients.
Patients with visual acuity worse than finger counting in both eyes and those with significant comorbidities were excluded, including:
• Type I or II diabetes mellitus requiring insulin
• Subarachnoid hemorrhage with associated heart disease
• Renal failure requiring dialysis
• Ongoing cancer treatment
• Other ophthalmic diseases (moderate or severe cataract according to LOCS III criteria, glaucoma or other optic nerve disease, uveitis, corneal disease, other retinal diseases, and strabismus)
Quality of life was assessed using the NEI VFQ-25 questionnaire. This instrument consists of 25 questions covering 11 vision-related domains (general vision, near and distance activities, eye pain, social functioning, functional activities, mental health, dependence, driving difficulties, color vision, and peripheral vision), plus one additional item addressing general health. Each domain includes between one and four items. Scores range from 0 to 100, with higher values indicating better visual function and well-being. The questionnaire can be administered either by an interviewer or self-administered by the patient; in this study, it was self-administered at two time points: before and after treatment procedures(26-30).
In this format, values represent a percentage of the total possible score; for example, a score of 50 corresponds to 50% of the maximum score. Vision-related quality of life was considered abnormal when the score was below 50 in any of the 10 vision-related domains, excluding the ocular pain domain. This threshold corresponds to approximately two standard deviations below values reported for the normal population(26-28).
Statistical analysis was performed using R version 4.2.0 (R Foundation for Statistical Computing, 2022). Exploratory data analysis included summary measures (mean, standard deviation, first quartile, median, third quartile, frequency, and percentage). Groups were compared using the Mann–Whitney test for numerical variables and the chi-square test for categorical variables. Spearman’s correlation coefficient was used to assess correlations between numerical variables. Multiple linear regression models, with dependent variables transformed into ranks, were used to identify factors that best explain variability in quality-of-life domains. A significance level of 5% was adopted.
Missing responses in NEI VFQ-25 domains were handled using available-case analysis. Each domain was analyzed using only patients who responded to that domain. The ocular pain, distance activities, and driving domains had substantial missing data and were therefore excluded from the regression analysis.
RESULTS
Eighty-one patients participated in the study: 43 (53%) were treated with PRN and 38 (47%) with T&E.
Tables 1 and 2 show that the two groups were homogeneous with respect to demographic and clinical characteristics.
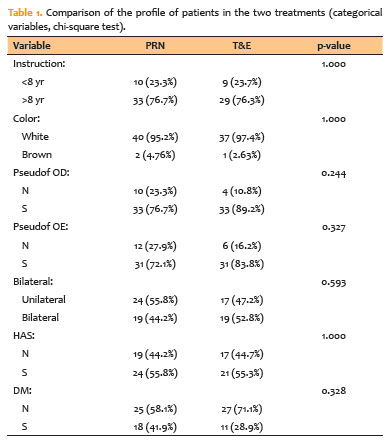
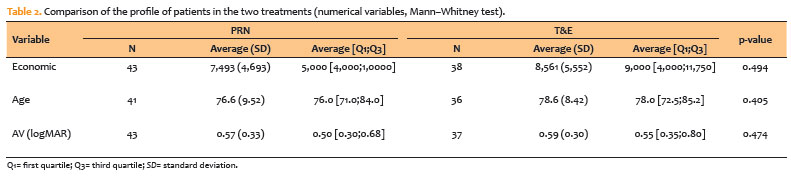
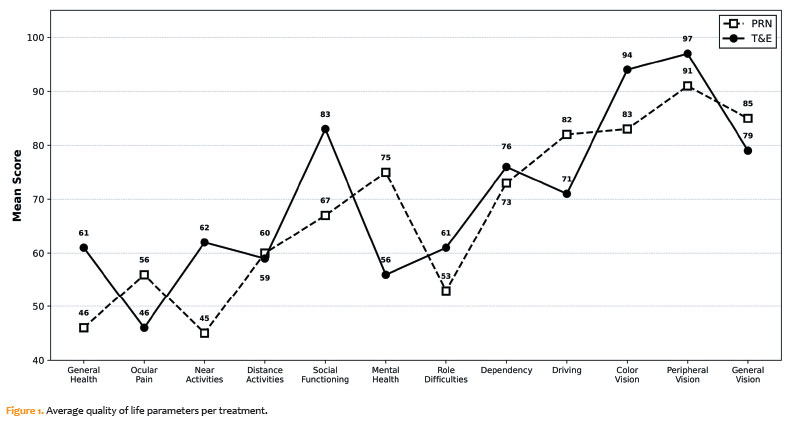
Table 3 shows that no statistically significant differences were observed between the treatment groups in terms of quality-of-life parameters measured by the NEI VFQ-25. However, Figure 1 suggests that PRN treatment tended to yield higher scores than T&E treatment.
As no statistically significant differences were observed between the two groups regarding clinical and demographic characteristics, the relationship between these variables and quality of life was analyzed for the entire cohort without stratification by treatment regimen.
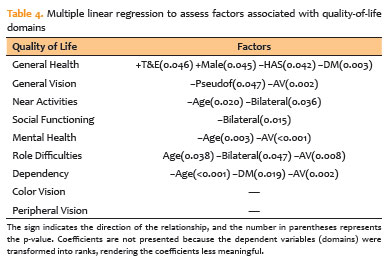
To identify factors that best explain variation in quality-of-life domains, multiple linear regression analysis was performed (Table 4). Due to the non-normality of residuals in the standard regression model, the dependent variables (domains) were transformed into ranks, resulting in a nonparametric version of linear regression.
DISCUSSION
The PRN regimen consists of three intravitreal injections administered at 1-month intervals (loading doses). After this phase, patients attend monthly follow-up visits, during which disease activity is assessed using complementary examinations. Based on this evaluation, additional injections may or may not be indicated according to pre-established criteria. This approach requires frequent visits, and patients are not informed in advance whether an injection will be needed. Therefore, PRN is considered a reactive regimen, as treatment is administered only in the presence of disease activity(13,22).
In contrast, the more recently proposed T&E regimen involves variable intervals between visits, but intravitreal injections are administered at every scheduled appointment. Similar to PRN, it begins with loading doses; thereafter, treatment intervals are adjusted according to disease control. In the absence of disease activity, intervals are progressively extended, whereas evidence of activity shortens intervals to regain control. This strategy allows greater individualization of treatment and reduces the number of clinic visits. In addition, patients are aware that injections will be performed at each visit. Thus, T&E is considered a proactive regimen, aiming to prevent disease recurrence(13,21).
Several studies have compared these regimens, evaluating visual outcomes, number of visits, number of injections, physician preference, and the impact on patients’ quality of life and that of their caregivers. Some recent studies have reported better final visual acuity and lower macular thickness in patients treated with T&E compared with PRN, although at the cost of a higher number of injections(17-20). From the physician’s perspective, PRN offers the advantage of fewer injections and simpler patient communication, as treatment is administered only when disease activity is present. In contrast, T&E may allow shorter consultation times and more efficient scheduling of intravitreal procedures(23).
Regarding the patient perspective and quality of life, Iida et al. reported differing advantages between the regimens. PRN is associated with fewer injections, reduced costs, and potentially fewer adverse effects. However, patients may experience uncertainty or frustration due to the unpredictability of treatment. Conversely, the T&E regimen may promote a more proactive approach, reduce anxiety, and facilitate planning, but it may increase the financial burden and exposure to procedure-related risks due to more frequent injections(23). Similar considerations apply to the social, emotional, and economic impact on family members or caregivers accompanying patients to appointments(24).
Although previous studies have suggested the superiority of T&E over PRN in terms of visual outcomes and treatment burden, our study did not demonstrate significant differences in vision-related quality of life between the two regimens. This finding may indicate that improvements in visual acuity or reductions in visit frequency do not necessarily translate into perceptible differences in quality of life when both regimens achieve adequate disease control(17-20,23,24).
In this study, we aimed to evaluate the impact of treatment regimens on patients’ quality of life and, consequently, their potential preference for one approach over the other. Adherence to long-term therapy for nAMD requires that patients feel comfortable and satisfied with their treatment, as interruptions in therapy may lead to significant visual deterioration. Therefore, identifying a regimen that maintains treatment efficacy while aligning with patients’ daily routines and expectations is an important consideration.
Despite extensive research, a universally preferred therapeutic regimen has not yet been established. One possible approach is to better inform patients and caregivers about the chronic nature of the disease and available treatment strategies, enabling them to make more informed decisions and choose care that best fits their circumstances(25). As no significant differences in quality of life were observed between regimens in this study, further research is needed to determine which approach best aligns with patient preferences and lifestyles.
According to Picoto et al.(8), worse visual acuity in the poorer-seeing eye is associated with higher NEI VFQ-25 scores, suggesting that this parameter may be useful in future studies comparing different regimens. Furthermore, Müller et al.(25) reported that many patients have limited knowledge about AMD, including its chronic nature, which may influence self-reported outcomes and symptom perception.
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships between treatment regimen and quality of life. Second, the study population was drawn from a private practice setting, which may limit generalizability, particularly to public healthcare systems. In addition, insurance-related restrictions influenced treatment allocation. Unmeasured socioeconomic factors may also have introduced bias. Missing responses in certain domains (such as ocular pain, distance activities, and driving) limited the comprehensive evaluation of NEI VFQ-25 scores. Finally, reliance on patient-reported outcomes introduces the possibility of recall bias.
Future studies, including larger and more diverse populations, are needed to better understand the advantages and limitations of each regimen. Such research may contribute to the development of standardized, evidence-based protocols that optimize both clinical outcomes and patients’ vision-related quality of life.
AUTHORS´ CONTRIBUTIONS:
Significant contribution to conception and design: Plínio Augusto Trindade Abreu, Osias Francisco de Souza. Data Acquisition: Plínio Augusto Trindade Abreu, Juan Silva Locks Camargo, Lais Bomediano de Souza, Osias Francisco de Souza. Data Analysis and Interpretation: Plínio Augusto Trindade Abreu, Osias Francisco de Souza. Manuscript Drafting: Plínio Augusto Trindade Abreu, Osias Francisco de Souza. Significant intellectual content revision of the manuscript: Plínio Augusto Trindade Abreu, Osias Francisco de Souza. Final approval of the submitted manuscript: Plínio Augusto Trindade Abreu, Juan Silva Locks Camargo, Lais Bomediano de Souza, José Paulo Cabral de Vasconcelos, Osias Francisco de Souza. Statistical analysis: Plínio Augusto Trindade Abreu, Osias Francisco de Souza. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Osias Francisco de Souza, José Paulo Cabral de Vasconcelos. Research group leadership: Osias Francisco de Souza, José Paulo Cabral de Vasconcelos.
REFERENCES
1. Jager RD, Miller WF, Miller JW. Age-related macular degeneration. N Engl J Med. 2008;358(24):2606-17. Erratum in: N Engl J Med. 2008;359(16):1736.Comment in: N Engl J Med. 2008;359(16):1735; author reply 1736.
2. Mitchell P, Liew G, Gopinath B, Wong TY. Age-related macular degeneration. Lancet. 2018;392(10153):1147-59.
3. Chakravarthy U, Wong TY, Fletcher A, Piault E, Evans C, Zlateva G, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10(1):31.
4. Lim LS, Mitchell P, Seddon JM, Holz FG, Wong TY. Age-related macular degeneration. Lancet. 2012;379(9827):1728-38.
5. Al-Zamil WM, Yassin SA. Recent developments in age-related macular degeneration: a review. Clin Interv Aging. 2017;12:1313-30.
6. Li JQ, Welchowski T, Schmid M, Mauschitz MM, Holz FG, Finger RP. Prevalence and incidence of age-related macular degeneration in Europe: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(8):1077-84. Comment in: Br J Ophthalmol. 2020;104(4):449-50.
7. Rein DB, Wittenborn JS, Burke-Conte Z, Gulia R, Robalik T, Ehrlich JR, et al. Prevalence of age-related macular degeneration in the US in 2019. JAMA Ophthalmol. 2022;140(12):1202–8.
8. Picoto M, Galveia J, Patrício S, Rodrigues A, Vaz F. Qualidade de vida relacionada com a visão em pacientes com degeneração macular relacionada à idade neovascular. Rev Bras Oftalmol. 2015;74(4):216-21.
9. Williams RA, Brody BL, Thomas RG, Kaplan RM, Brown SI. The psychosocial impact of macular degeneration. Arch Ophthalmol. 1998;116(4):514-20.
10. Brody BL, Gamst AC, Williams RA, Smith AR, Lau PW, Dolnak D, et al. Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology. 2001;108(10):1893-900.
11. Servat JJ, Risco M, Nakasato YR, Bernardino CR. Visual impairment in the elderly: impact on functional ability and quality of life. Clin Geriatr. 2011;19(7):49-56.
12. Gopinath B, Liew G, Burlutsky G, Mitchell P. Age-related macular degeneration and 5-year incidence of impaired activities of daily living. Maturitas. 2014;77(3):263-6.
13. Astakhov YS, Nechiporenko PA. Dosing regimens of angiogenesis inhibitors in the treatment of neovascular age-related macular degeneration patients. Ophthalmol J. 2019;12(2):47-56.
14. Wykoff CC, Ou WC, Croft DE, Payne JF, Brown DM, Clark WL, Abdelfattah NS, Sadda SR; TREX-AMD Study Group. Neovascular age-related macular degeneration management in the third year: final results from the TREX-AMD randomised trial. Br J Ophthalmol. 2018;102(4):460-4.
15. Rufai SR, Almuhtaseb H, Paul RM, Stuart BL, Kendrick T, Lee H, et al. A systematic review to assess the ‘treat-and-extend’ dosing regimen for neovascular age-related macular degeneration using ranibizumab. Eye (Lond). 2017;31(9):1337-44.
16. Wykoff CC, Ou WC, Brown DM, Croft DE, Wang R, Payne JF, Clark WL, Abdelfattah NS, Sadda SR; TREX-AMD Study Group. Randomized trial of treat-and-extend versus monthly dosing for neovascular age-related macular degeneration. Ophthalmol Retina. 2017;1(4):314-21.
17. Chin-Yee D, Eck T, Fowler S, Hardi A, Apte RS. A systematic review of as-needed versus treat and extend ranibizumab or bevacizumab treatment regimens for neovascular age-related macular degeneration. Br J Ophthalmol. 2016;100(7):914-7.
18. Augsburger M, Sarra GM, Imesch P. Treat and extend versus preventive regimens of ranibizumab and aflibercept in neovascular age-related macular degeneration: a comparative study. Graefes Arch Clin Exp Ophthalmol. 2019;257(9):1889-95.
19. Aurell S, Sjövall, Paul A, Morén A, Granstam E. Better visual outcome at 1 year with antivascular endothelial growth factor treatment according to treat-and-extend compared with pro re nata in eyes with neovascular age-related macular degeneration. Acta Ophthalmol. 2019;97(5):519-24.
20. Meira J, Carneiro J, Madeira C, Falcão M, Beato J, Correia S, et al. Effectiveness of treat-and-extend versus pro re nata regimens in the treatment of neovascular age macular degeneration: a real-world comparison. Arch Soc Esp Ophthalmol. 2020;95(6):263-70.
21. Silva R, Berta A, Larsen M, Macfadden W, Feller C, Monés J; TREND Study Group. Treat-and-extend versus monthly regimen in neovascular age-related macular degeneration: results with ranibizumab from the TREND Study. Ophthalmology. 2018;125(1):57-65. Comment in: Ophthalmology. 2018;125(1):2-3.
22. Lalwani GA, Rosenfeld PJ, Fung AE, Dubovy SR, Michels S, Feuer W, et al. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO Study. Am J Ophthalmol. 2009;148(1):43-58.
23. Iida T, Ishii K. Physician, patient, and caregiver experience of different wet age-related macular degeneration anti-VEGF treatment regimens in Japan: a qualitative assessment. Clin Ophthalmol. 2016;10:2505-13.
24. Hanemoto T, Hikichi Y, Kikuchi N, Kozawa T. The impact of different anti-vascular endothelial growth factor treatment regimens on reducing burden for caregivers and patients with wet age-related macular degeneration in a single-center real-world Japanese setting. PLoS One. 2017;12(12):e0189035.
25. Müller S, Ehlken C, Bauer-Steinhusen U, Lechtenfeld W, Hasanbasic Z, Agostini H, et al. Treatment of age-related neovascular macular degeneration: the patient’s perspective. Graefes Arch Clin Exp Ophtalmol. 2017;255(11):2237-46.
26. Mangione CM, Lee PP, Pitts J, Gutierrez P, Berry S, Hays RD. Psychometric properties of the National Eye Institute Visual Function Questionnaire (NEI-VFQ). Arch Ophthalmol. 1998;116(11):1496-504.
27. Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, Hays RD; National Eye Institute Visual Function Questionnaire Field Test Investigators. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 2001;119(7):1050-8.
28. Simão LM, Lana-Peixoto MA, Araújo CR, Moreira MA, Teixeira AL. The Brazilian version of the 25-Item National Eye Institute Visual Function Questionnaire: translation, reliability, and validity. Arq Bras Oftalmol. 2008;71(4):540-6.
29. Marback RF, Maia OO Jr, Morais FB, Takahashi WY. Quality of life in patients with age-related macular degeneration with monocular and binocular legal blindness. Clinics. 2007;62(5):573-8.
30. Puhan MA, Ahuja A, Van Natta ML, Ackatz LE, Meinert C; Studies of ocular complications of AIDS research group. Interviewer versus self-administered health-related quality of life questionnaires: does it matter?. Health Qual Life Outcomes. 2011;9:30.
Submitted for publication:
September 11, 2025.
Accepted for publication:
March 26, 2026.
Approved by the following research ethics committee: UNICAMP – Campus Campinas (CAAE: 59284721.5.0000.5404).
Data Availability Statement: The datasets generated and/or analyzed during the current study are included in the manuscript.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Carlos Augusto Moreira Neto
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.