Arq. Bras. Oftalmol. 2026; 89 (3): 10.5935/0004-2749.2025-0043
Total: 406
Hakan Öztürk1; Bediz Özen2
DOI: 10.5935/0004-2749.2025-0043
ABSTRACT
PURPOSE: To evaluate the effect of single-session transscleral diode laser cyclophotocoagulation on intraocular pressure in refractory glaucoma and to determine structural changes using ultrasound biomicroscopy.
METHODS: Forty-three eyes were evaluated. Intraocular pressures at baseline and at the first, third, and sixth months after transscleral diode laser cyclophotocoagulation were compared. Ciliary body thickness, ciliary muscle thickness, ciliary process thickness, iris root thickness, and scleral thickness were assessed at baseline and at the third and sixth months post-treatment.
RESULTS: Reductions in intraocular pressure were significant between baseline and the first month (p=0.018), third month (p<0.001), and sixth month (p<0.001) as well as between the first and third months (p=0.034) and the first and sixth months (p=0.036). Compared with baseline, intraocular pressure reduction rates at the first, third, and sixth months were 34.6%, 56.5%, and 55.3%, respectively, while success rates were 30.2%, 62.8%, and 55.8%, respectively. Decreases in ciliary body thickness, ciliary muscle thickness, and ciliary process thickness were significant between baseline and the third month (p<0.05) and between baseline and the sixth month (p<0.05), whereas changes between the third and sixth months were not significant (p>0.05). Iris root and scleral thicknesses did not change after treatment (p>0.05). At the third and sixth months, significant positive correlations were observed between changes in intraocular pressure and changes in ciliary body thickness and ciliary process thickness (p<0.05).
CONCLUSIONS: To the best of our knowledge, this is one of the few studies comprehensively investigating structural changes after transscleral diode laser cyclophotocoagulation using ultrasound biomicroscopy. Moreover, the relationships between intraocular pressure changes and variations in the ciliary body, ciliary muscle, ciliary process, iris root, and scleral thicknesses were examined in detail. Single-session treatment did not affect iris root or scleral thickness but significantly reduced ciliary body, ciliary muscle, and ciliary process thicknesses. Greater reductions in ciliary body and ciliary process thickness may contribute to more pronounced intraocular pressure reduction.
Keywords: Intraocular pressure; Laser coagulation/methods; Lasers, semiconductor; Microscopy, acoustic; Glaucoma; Ciliary body
INTRODUCTION
Glaucoma is a major cause of irreversible blindness worldwide(1,2). The primary goal of glaucoma treatment is to control intraocular pressure (IOP) and slow or halt disease progression as much as possible. Medical, surgical, and/or laser therapies may be used to achieve IOP control(1). Refractory glaucoma is defined as uncontrolled IOP despite maximally tolerated medical therapy and/or prior surgical interventions(3,4). In such cases, cyclodestructive procedures may be beneficial(2,4-8).
Laser cyclophotocoagulation has been reported to be better tolerated, more effective, and associated with fewer complications than cyclocryotherapy(4,9). Due to their efficiency and cost-effectiveness, diode lasers are preferred over Nd:YAG and argon lasers for cyclophotocoagulation(3,4,9). Additionally, the transscleral approach is more commonly used than transpupillary and endoscopic methods because of its ease of application(9). Transscleral diode laser cyclophotocoagulation (TDLC) is typically performed using a contact probe(4,9). In this procedure, 810-nm diode laser energy passes through the sclera and is absorbed by melanin in the ciliary body epithelium(2,3). This absorption results in coagulative necrosis of the ciliary body, reducing aqueous humor production and thereby lowering IOP(2,3,9,10).
The ciliary body and adjacent anatomical structures cannot be directly visualized using slit-lamp biomicroscopy(11). Ultrasound biomicroscopy (UBM), due to its high resolution, is an effective imaging modality for evaluating deep ocular structures, including the ciliary body and ciliary processes(11-14). UBM has demonstrated high intraobserver reliability and interobserver agreement(11,12).
Although previous studies have investigated the effect of single-session TDLC on IOP in patients with refractory glaucoma(15-19), only a limited number have partially examined associated structural changes(16,19). Liu et al.(20) evaluated ocular structural changes after TDLC using UBM in cases of refractory acute primary angle closure. However, correlations between structural changes and IOP reduction have not been thoroughly investigated. Furthermore, the effects of TDLC on iris root thickness (IRT) and scleral thickness (ST) have not been comprehensively studied.
Therefore, the present study aimed to evaluate the effect of single-session TDLC on IOP in refractory glaucoma and to determine associated structural changes using UBM. Additionally, we aimed to investigate the relationships between changes in IOP and alterations in ciliary body thickness (CBT), ciliary muscle thickness (CMT), ciliary process thickness (CPT), IRT, and ST.
METHODS
This study was conducted with approval from our hospital’s ethics committee (Approval No. 2020/12-44) and in accordance with the ethical principles of the Declaration of Helsinki. Detailed information about the study was provided to all participants and/or their families, and potential risks were explained. Written informed consent was obtained from all participants and/or their families.
A total of 43 eyes from 43 patients with refractory glaucoma were evaluated. All patients had undergone UBM examinations before and after TDLC, received a single-session treatment, and attended regular follow-up visits. These patients presented with painful eyes and uncontrolled high IOP despite maximally tolerated medical therapy before TDLC, and all had no light perception in the affected eye. The underlying diagnosis in all cases was primary open-angle glaucoma. All patients had a history of uncomplicated phacoemulsification and failed filtration surgery.
Patients who had previously undergone cyclodestructive therapy, had a history of ocular trauma, had narrow or closed anterior chamber angles, central corneal scars, bilateral refractory glaucoma, or axial lengths <22 or >25 mm were excluded. Demographic characteristics (age and sex), medical history, anterior and posterior segment findings, gonioscopic examination results, IOP measurements obtained using a Goldmann applanation tonometer, and UBM findings were recorded.
Laser treatment was performed by a single surgeon (B.Ö.) in the operating room under peribulbar, retrobulbar, or general anesthesia. An Iris OcuLight SLx diode laser photocoagulation system (Iris Medical Instruments, Mountain View, California) was used for TDLC. In this system, a continuous-wave semiconductor diode laser (810 nm) was applied 1.5 mm posterior to the limbus using a contact G-probe. The laser power was adjusted according to the audible “pop” sound and ranged between 1,500 and 2,000 mW, with a duration of 2 s per application. A total of 16–20 laser spots were applied over 360°, avoiding the 3 and 9 o’clock positions (corresponding to the long ciliary nerves), areas of previous filtration surgery, and regions of thin sclera.
Postoperatively, topical dexamethasone 0.1% was administered four times daily and topical cycloplegic (cyclopentolate hydrochloride 1%) three times daily for 2 weeks. UBM imaging was performed 1 h after the instillation of three drops of cyclopentolate hydrochloride 1%.
UBM scans were obtained by a single researcher (B.Ö.) using a 50-MHz B-mode UBM device (Aviso, Quantel Medical, Cournon-d’Auvergne, France). Measurements were consistently performed in the same regions before and after TDLC to detect anatomical changes related to cyclophotocoagulation. Superotemporal and inferotemporal quadrants were selected because TDLC was applied in these regions in all cases and because these areas allowed easier probe movement without obstruction from orbital structures. Specifically, measurements were taken at the 7 and 11 o’clock positions in the right eye and at the 1 and 5 o’clock positions in the left eye.
UBM images from these positions were evaluated by another researcher (H.Ö.) who was blinded to the clinical data. For each parameter, the mean of three measurements obtained from each area was used for analysis. The scleral spur served as the reference point in UBM imaging(13). Measurements were performed according to previously described methods(13,14,21,22).
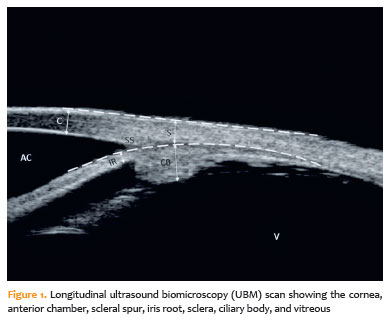
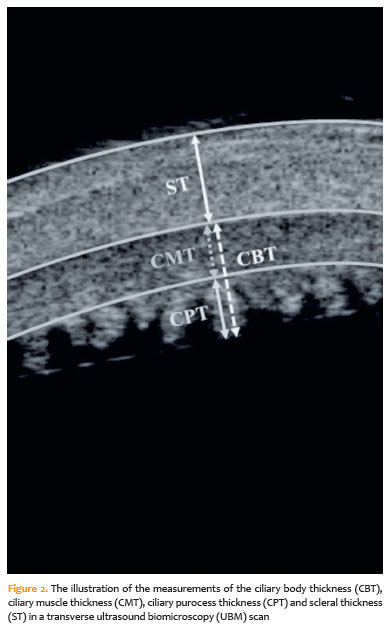
CBT was defined as the vertical distance between the tip of the ciliary process and the inner scleral wall at a point 1 mm posterior to the scleral spur. CMT was measured as the vertical distance between the base of the ciliary process and the inner scleral wall at the same location. CPT was defined as the vertical distance between the tip and base of the ciliary process. ST was measured as the perpendicular distance from the inner scleral wall to the episcleral surface at 1 mm posterior to the scleral spur. IRT was measured at a point 250 μm from the scleral spur. A longitudinal UBM scan showing relevant ocular structures is presented in figure 1, and a schematic illustration of CBT, CMT, CPT, and ST measurements is shown in figure 2.
IOP values at baseline (pre-TDLC) and at the first, third, and sixth months after TDLC were compared. IOP reduction and success rates were calculated at each follow-up time point relative to baseline. IOP reduction (%) was calculated as the difference between baseline and post-TDLC IOP divided by baseline IOP, multiplied by 100. Treatment success was defined as an IOP reduction of ≥20% and a post-TDLC IOP between 8 and 21 mmHg without an increase in preexisting antiglaucoma medications. The success rate (%) was calculated as the proportion of successful cases relative to the total number of cases.
Because early postoperative changes such as bleeding, inflammation, and tissue edema may affect thickness measurements, UBM evaluations were performed at the third and sixth months after TDLC. CBT, CMT, CPT, IRT, and ST values at baseline were compared with those at the third and sixth months. Differences between baseline and post-TDLC measurements were calculated. Correlations between changes in IOP and changes in CBT, CMT, CPT, IRT, and ST at 3 and 6 months were analyzed.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 20.0 (IBM Corp., Armonk, New York). A post hoc power analysis indicated that a minimum sample size of 24 was required to detect statistically significant differences among the main variables with 80% power and an α level of 0.05. Intraobserver repeatability of UBM measurements was assessed using the coefficient of variation (CV) and intraclass correlation coefficient (ICC), based on three consecutive measurements per parameter. Low variability (CV=6%; 95% confidence interval [95% CI], 4.6–7.2) and high repeatability (ICC=0.90; 95% CI, 0.84–0.94) were observed.
Continuous variables are presented as mean±standard deviation (minimum–maximum), while categorical variables are expressed as counts and percentages. Normality was assessed using the Kolmogorov–Smirnov test. Comparisons were performed using the chi-square test for categorical variables, repeated-measures analysis of variance for normally distributed variables, and the Friedman test for non-normally distributed variables, followed by post hoc analysis. Correlations were evaluated using Spearman’s correlation analysis. A p-value <0.05 was considered statistically significant.
RESULTS
The mean age of the cases was 67.8 ± 9.4 (54–82) yr. There were 24 (55.8%) men and 19 (44.2%) women in the study.
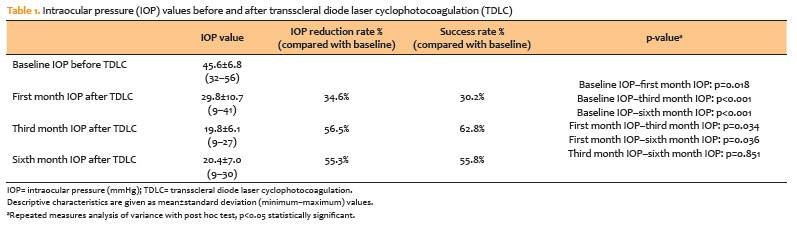
Significant reductions in IOP were found between baseline and the first month (p=0.018), baseline and the third month (p<0.001), baseline and the sixth month (p<0.001), the first and third months (p=0.034), and the first and sixth months (p=0.036). IOP values at the third and sixth months were similar (p=0.851).
Compared with baseline, IOP reduction rates at the first, third, and sixth months were 34.6%, 56.5%, and 55.3%, while success rates were 30.2% (13/43), 62.8% (27/43), and 55.8% (24/43), respectively. IOP values before and after TDLC are presented in table 1.
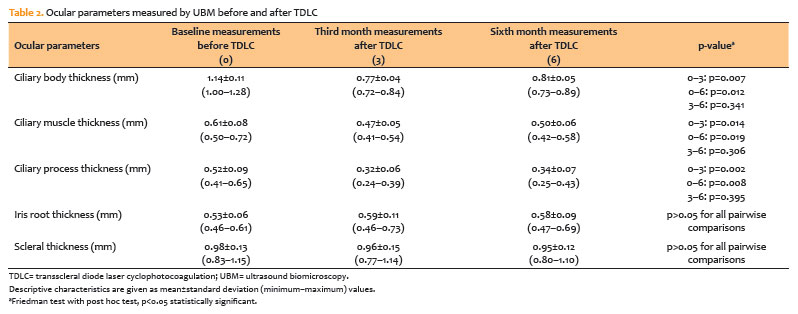
Decreases in CBT, CMT, and CPT were significant between baseline and the third month (p=0.007, p=0.014, and p=0.002, respectively) and between baseline and the sixth month (p=0.012, p=0.019, and p=0.008, respectively), whereas changes between the third and sixth months were not significant (p>0.05). IRT and ST values did not change after TDLC (p>0.05). Ocular parameters measured by UBM before and after TDLC are shown in table 2.
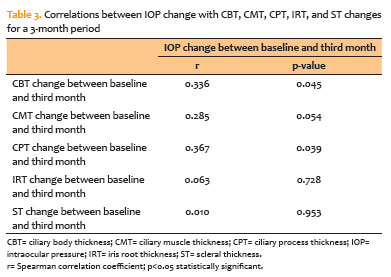
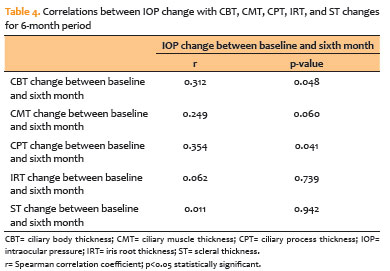
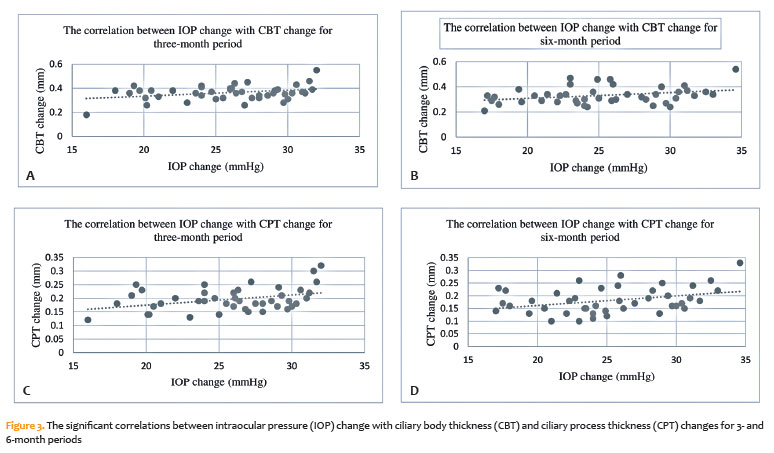
At both the third and sixth months compared to baseline, there were significant positive correlations between IOP change and CBT change (r=0.336, p=0.045 at third month; r=0.312, p=0.048 at sixth month) and CPT change (r=0.367, p=0.039 at third month; r=0.354, p=0.041 at sixth month). As CBT and CPT changes increased, the IOP change also increased. In other words, greater reductions in IOP were associated with greater shortening of CBT and CPT.
On the other hand, CMT, IRT, and ST changes were not significantly correlated with IOP change for the three- and six-month periods (p>0.05). Correlations between IOP change and CBT, CMT, CPT, IRT, and ST changes are presented in tables 3 and 4. The significant correlations are also shown in figures 3A–3D.
The mean number of antiglaucoma medications before and after TDLC was similar (3.45 ± 0.40 vs. 3.40 ± 0.40, p=0.872). A temporary increase in IOP (mean 6.5 mmHg above baseline) occurred in 7 (16.3%) cases, and anterior chamber reaction was observed in 16 (37.2%) patients within the first week after TDLC. These resolved with local and/or systemic treatment within 2 weeks. Conjunctival and/or scleral burns, hyphema, pupillary distortion, hypotony, and phthisis bulbi did not occur in any case.
DISCUSSION
In refractory glaucoma cases, diode laser cyclophotocoagulation is a commonly preferred cyclodestructive method because it is less invasive than older procedures such as cyclocryotherapy and cyclodiathermy(2,4,7,9). In the literature, the IOP reduction rate after single-session TDLC has been reported as 30.9%–66%(15-19), and the success rate as 40%–69%(15-17).
Graber et al.(15) reported IOP reductions of 46.9% at the first month and 50.1% at the third month, while Safwat et al.(16) reported reductions of 38.7% and 53.2% at the same time points. Bezci et al.(17) reported a 30.9% reduction at the third month, whereas Miljković et al.(18) reported reductions of 56% at the first month and 43% at the sixth month.
In our study, IOP decreased significantly at the first, third, and sixth months compared to baseline, and the IOP-lowering effect of single-session TDLC continued up to the sixth month in many cases. Our IOP reduction rates (34.6%, 56.5%, and 55.3%) and success rates (30.2%, 62.8%, and 55.8%) are consistent with the literature. The reduction in IOP after TDLC may be due to decreased aqueous humor production resulting from destruction of the ciliary body by the laser(2,4,7). Another reason may be the increase in uveoscleral outflow due to increased permeability of the ciliary body and sclera to aqueous humor(4,7).
Until our study, very few publications had partially examined the effect of single-session TDLC on some ocular structures in refractory glaucoma cases using UBM(16,19). Kayıkçıoğlu et al.(19) evaluated only CBT and reported a significant decrease after laser treatment. In addition, Safwat et al. found significant reductions in CMT and ciliary process length at 3 months after treatment(16). Moreover, the effects of TDLC on IOP and various ocular structures were also investigated in cases with refractory acute primary angle closure(20). Liu et al. found that TDLC applied to the inferior quadrant effectively lowered IOP, increased anterior chamber depth, and widened the inferior angle in these eyes. They also reported that the angle-opening distance at 500 μm and the maximum CBT value increased significantly on Day 1 after the procedure, whereas the iris thickness at 500 μm remained unchanged. The authors suggested that these early changes were due to initial shrinkage causing posterior movement of the lens–iris diaphragm, followed by swelling due to edema formation(20).
In our study, significant decreases in CBT, CMT, and CPT were detected at the third and sixth months compared to baseline. In human autopsy eyes, Pantcheva et al.(10) investigated acute histological changes in laser-treated areas after TDLC. They observed destruction of the ciliary epithelium and coagulative necrosis of the ciliary processes’ stroma in the acute period. Additionally, disruption of the ciliary body muscle and stroma was noted(10). Necrosis, tissue damage, chronic poor perfusion, and ischemia may eventually lead to focal atrophy and fibrosis of ciliary structures(7,23). In our study, the reductions in CBT, CMT, and CPT after TDLC may be explained by these histological changes(7,10,23).
As far as we know, the effects of single-session TDLC on IRT and ST have not been comprehensively investigated. In our study, IRT and ST did not change at the third and sixth months compared to baseline. Pantcheva et al.(10) also showed that the sclera was not affected in the acute period after TDLC in human autopsy eyes. The lack of change in ST in our study may be because laser energy passes through the sclera and is mainly absorbed by deeper ciliary structures(3,5). Similarly, the absence of change in IRT may be related to improvements in the G-probe design, which help prevent iris damage(5,7).
To the best of our knowledge, our study is the first to comprehensively investigate the relationships between IOP change and changes in CBT, CMT, CPT, IRT, and ST. Therefore, direct comparison with previous studies is limited. We found that as CBT and CPT changes increased, the IOP change also increased. In TDLC, diode laser energy is strongly absorbed by melanin in the ciliary body epithelium(2,3). Laser-induced coagulative necrosis and tissue damage may lead to shrinkage, atrophy, and fibrosis, resulting in reduced aqueous humor production(2,3,7,9,10,23). Greater shrinkage of the ciliary body, especially the ciliary processes, may therefore contribute to greater IOP reduction.
On the other hand, changes in CMT, IRT, and ST were not significantly correlated with IOP change in our study. Based on these findings, greater CPT shortening, and consequently CBT shortening, may be important factors contributing to further IOP reduction after TDLC.
In the literature, complications such as temporary IOP elevation, anterior chamber reaction, hyphema, and episcleral edema have been reported after single-session TDLC(15-17). In our study, a temporary increase in IOP was observed in seven (16.3%) cases, and anterior chamber reaction in 16 (37.2%) patients within the first week after TDLC. These resolved with local and/or systemic treatment within 2 weeks. No cases of conjunctival or scleral burns, hyphema, pupillary distortion, hypotony, or phthisis bulbi were observed. Temporary IOP elevation may be related to inflammation or intraocular volume changes caused by air bubbles during cyclodestruction(5,24). Anterior chamber reaction may be associated with disruption of the blood–aqueous barrier(4).
This study has some limitations. It included a relatively small number of cases and had a short follow-up period. Histological tissue changes could not be directly evaluated. In addition, there may be other factors affecting ciliary structures and/or IOP after TDLC that were not identified. Future studies with larger sample sizes and longer follow-up periods may provide more comprehensive data.
In conclusion, single-session TDLC did not affect IRT and ST but significantly reduced CBT, CMT, and CPT, and its IOP-lowering effect persisted up to the sixth month in many cases. As CBT and CPT changes increased, the IOP reduction also increased. Greater shortening of CPT and CBT may therefore contribute to further IOP reduction. These findings may guide future studies on TDLC. In addition to IOP measurements, evaluation of structural changes in the ciliary region using UBM may help clinicians assess the effectiveness of this procedure in refractory glaucoma patients.
ACKNOWLEDGMENTS
The authors would like to thank Enago (www.enago.br) for the English language review.
AUTHOR’S CONTRIBUTIONS:
Significant contribution to conception and design: Hakan Öztürk, Bediz Özen. Data acquisition: Hakan Öztürk, Bediz Özen. Data analysis and interpretation: Hakan Öztürk, Bediz Özen. Manuscript drafting: Hakan Öztürk, Bediz Özen. Significant intellectual content revision of the manuscript: Hakan Öztürk, Bediz Özen. Final approval of the submitted manuscript: Hakan Öztürk, Bediz Özen. Statistical analysis: not applicable. Obtaining funding: not appliable. Supervision of administrative, technical, or material support: Hakan Öztürk, Bediz Özen. Research group leadership: Hakan Öztürk, Bediz Özen.
REFERENCES
1. Kang JM, Tanna AP. Glaucoma. Med Clin North Am. 2021;105(3):493-510.
2. Chen MF, Kim CH, Coleman AL. Cyclodestructive procedures for refractory glaucoma. Cochrane Database Syst Rev. 2019;3(3):CD012223.
3. Anand N, Klug E, Nirappel A, Solá-Del Valle D. A review of cyclodestructive procedures for the treatment of glaucoma. Semin Ophthalmol. 2020; 35(5-6):261-75.
4. Kumar H, Mansoori T, Warjri GB, Somarajan BI, Bandil S, Gupta V. Lasers in glaucoma. Indian J Ophthalmol. 2018;66(11):1539-53.
5. Souissi S, Le Mer Y, Metge F, Portmann A, Baudouin C, Labbé A, et al. An update on continuous-wave cyclophotocoagulation (CW-CPC) and micropulse transscleral laser treatment (MP-TLT) for adult and paediatric refractory glaucoma. Acta Ophthalmol. 2021;99(5):e621-e653.
6. European Glaucoma Society Terminology and Guidelines for Glaucoma. 4th ed. Chapter 3: Treatment principles and options supported by the EGS foundation: Part 1: Foreword; Introduction; Glossary; Chapter 3 Treatment principles and options. Br J Ophthalmol. 2017;101(6):130-95.
7. Dastiridou AI, Katsanos A, Denis P, Francis BA, Mikropoulos DG, Teus MA, et al. Cyclodestructive procedures in glaucoma: a review of current and emerging options. Adv Ther. 2018;35(12):2103-27.
8. Lin SC. Endoscopic and transscleral cyclophotocoagulation for the treatment of refractory glaucoma. J Glaucoma. 2002;17(3):238-47.
9. Ndulue JK, Rahmatnejad K, Sanvicente C, Wizov SS, Moster MR. Evolution of cyclophotocoagulation. J Ophthalmic Vis Res. 2018;13(1):55-61.
10. Pantcheva MB, Kahook MY, Schuman JS, Noecker RJ. Comparison of acute structural and histopathological changes in human autopsy eyes after endoscopic cyclophotocoagulation and trans-scleral cyclophotocoagulation. Br J Ophthalmol. 2007;91(2):248-52.
11. Li J, Drechsler J, Lin A, Widlus M, Qureshi A, Stoleru G, et al. Repeatability and reliability of quantified ultrasound biomicroscopy image analysis of the ciliary body at the pars plicata. Ultrasound Med Biol.2021;47(7):1949-56.
12. Vasquez LM, Giuliari GP, Halliday W, Pavlin CJ, Gallie BL, Héon E. Ultrasound biomicroscopy in the management of retinoblastoma. Eye (Lond). 2011;25(2):141-7.
13. Dada T, Gadia R, Sharma A, Ichhpujani P, Bali SJ, Bhartiya S, et al. Ultrasound biomicroscopy in glaucoma. Surv Ophthalmol. 2011;56(5):433-50.
14. Maslin JS, Barkana Y, Dorairaj SK. Anterior segment imaging in glaucoma: an updated review. Indian J Ophthalmol. 2015;63(8):630-40.
15. Graber M, Rothschild PR, Khoueir Z, Bluwol E, Benhatchi N, Lachkar Y. High intensity focused ultrasound cyclodestruction versus cyclodiode treatment of refractory glaucoma: a retrospective comparative study. J Fr Ophtalmol. 2018;41(7):611-8.
16. Safwat AM, Hammouda LM, El-Zembely HI, Omar IA. Evaluation of ciliary body by ultrasound bio-microscopy after trans-scleral diode cyclo-photocoagulation in refractory glaucoma. Eur J Ophthalmol. 2020;30(6):1335-41.
17. Bezci Aygün F, Mocan MC, Kocabeyoğlu S, İrkeç M. Efficacy of 180° cyclodiode transscleral photocoagulation for refractory glaucoma. Turk J Ophthalmol. 2018;48(6):299-303.
18. Miljković A, Babić N, Čanadanović V, Davidović S, Ljikar J, Vasin M. Efficacy of cyclocryotherapy and transscleral diode laser cyclophotocoagulation in the management of refractory glaucoma. Acta Clin Croat. 2021;60(2):171-7.
19. Kayıkçıoğlu ÖR, Öztürk Şahin B, Emre S, Bilgin S. Ciliary body thickness measurement with ultrasound biomicroscopy following transscleral diode laser cyclophotocoagulation. Glokom Katarakt. 2016;11(1):44-7. (Turkish)
20. Liu W, Qin L, Xu C, Huang D, Guo R, Ji J, et al. Transscleral cyclophotocoagulation followed by cataract surgery: a novel protocol to treat refractory acute primary angle closure. BMC Ophthalmol. 2020;20(1):209.
21. Muftuoglu O, Hosal BM, Zilelioglu G. Ciliary body thickness in unilateral high axial myopia. Eye (Lond). 2009;23(5):1176-81.
22. Okamoto Y, Okamoto F, Nakano S, Oshika T. Morphometric assessment of normal human ciliary body using ultrasound biomicroscopy. Graefes Arch Clin Exp Ophthalmol. 2017;255(12):2437-42.
23. Lin SC, Chen MJ, Lin MS, Howes E, Stamper RL. Vascular effects on ciliary tissue from endoscopic versus trans-scleral cyclophotocoagulation. Br J Ophthalmol. 2006;90(4):496-500. Comment in: Br J Ophthalmol. 2006;90(6):666-8.
24. Uppal S, Stead RE, Patil BB, Henry E, Moodie J, Vernon SA, et al. Short-term effect of diode laser cyclophotocoagulation on intraocular pressure: a prospective study. Clin Exp Ophthalmol. 2015;43(9):796-802.
Data Availability Statement: The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request, subject to appropriate conditions.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Tiago Prata
Submitted for publication:
January 31, 2026.
Accepted for publication:
March 26, 2026.
Approved by the following research ethics committee: Izmir Tepecik Training and Research Hospital (Approval No. 2020/12-44)
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.