Arq. Bras. Oftalmol. 2026; 89 (3): 10.5935/0004-2749.2025-0272
Total: 385
Jabneel Tassiano dos Santos Nogueira; Taíse Maria Clemente de Araújo; Carlos Eduardo Ximenes da Cunha; Carlos Henrique de Almeida Cipriano; Camila Vieira Ventura*; Michel Bittencourt Santos*
DOI: 10.5935/0004-2749.2025-0272
ABSTRACT
PURPOSE: To assess musculoskeletal symptoms, identify the most affected body areas, and investigate factors associated with the development of musculoskeletal disorders among ophthalmologists in Brazil.
METHODS: A survey was conducted using an online questionnaire and snowball sampling. Statistical analyses were performed using Jamovi version 2.3.28, and graphs were generated using RStudio version 2023.06.2 + 561.
RESULTS: A total of 233 participants (42 ophthalmology residents and 191 ophthalmologists) were included, with a mean age of 40.4 years (standard deviation 11.3; range 25–73 years). Musculoskeletal symptoms were reported by 83% of participants. The cervical region (57.1%), upper back (54.5%), and lumbar region (53.6%) were the most frequently reported sites of pain. A high body mass index was identified in 54.9% of the sample, and 50.2% of participants reported using painkillers in the previous year for musculoskeletal symptoms. The mean duration of professional activity in ophthalmology was 13.5 years, and the mean weekly workload was 39 hours. A significant association was observed between weekly workload and the presence of musculoskeletal disorders (p=0.045).
CONCLUSION: This study demonstrated a high prevalence of musculoskeletal disorders among ophthalmologists in Brazil, particularly involving the cervical, lumbar, and upper back regions, consistent with findings reported in international studies. Important contributing factors include long working hours, a high patient volume, and repetitive or awkward postures during examinations and procedures. Preventive strategies and improvements in working conditions are needed to protect the health and well-being of ophthalmologists.
Keywords: Musculoskeletal Diseases/epidemiology; Back pain; Lumbar Vertebrae; Occupational diseases/epidemiology; Ergonomics; Ophthalmic practice; Ophthalmologists/statistics & numerical data; Brazil/epidemiology
INTRODUCTION
Musculoskeletal disorders (MSDs) are preventable conditions that affect the muscles, bones, tendons, ligaments, nerves, and other tissues responsible for supporting and moving the body(1,2). They are associated with repetitive movements, sustained or awkward posture, vibrations, or excessive forces and are characterized by pain, inflammation, injury, and tissue degeneration. MSDs can affect different regions of the body, including the neck, back, shoulders, arms, hands, hips, knees, and feet(1,2).
MSDs are common among healthcare professionals, particularly those who perform interventional and/or surgical procedures in their clinical practice(2-5). They are also associated with long surgical shifts or a high number of consultations and may negatively affect the quality of life of healthcare professionals(6,7). Consequently, poor musculoskeletal health may impair work capacity, potentially leading to reduced productivity and a decline in the quality of patient care(2). Conversely, practices such as regular physical exercise, maintaining body weight within a healthy body mass index (BMI) range, and adopting ergonomic measures may act as protective factors against these symptoms(6).
Ophthalmologists are routinely exposed to working postures that may compromise musculoskeletal health. Activities such as slit-lamp examinations, surgical and nonsurgical procedures, retinal mapping using binocular indirect ophthalmoscopy, and the frequent need to record and review information on a computer require repetitive movements, fine motor control, and sustained visual concentration and are often associated with inadequate postures maintained for prolonged periods(4,8).
It is concerning that only 46% of ophthalmologists are aware of proper ergonomic practices(1). This finding highlights the need for specific training during residency and throughout professional practice to prevent the development of MSDs, promote the adoption of appropriate postures, and support a healthier and more sustainable work environment.
Studies conducted in India and the United States have shown that most ophthalmologists experience MSDs, particularly pain in the lumbar region and upper back. These studies also reported mild to moderate activity limitations associated with these symptoms(8,9). However, to date, no studies have specifically investigated the occurrence of MSDs among ophthalmologists in Brazil. Therefore, the present study aimed to investigate the prevalence of MSDs among Brazilian ophthalmologists and to identify the most affected body regions and potential factors associated with the development of this condition among ophthalmologists and ophthalmology residents in Brazil.
METHODS
This study met all ethical requirements for research and was approved by the Altino Ventura Foundation Research Ethics Committee (Institutional Review Board approval number: 6.631.825).
A survey was conducted among professionals in the field of ophthalmology, including ophthalmologists and ophthalmology residents with at least 1 year of experience in the field. First-year ophthalmology residents were excluded to avoid potential bias related to limited occupational exposure.
This survey was developed by the researchers based on a literature review and remote discussions to determine the most appropriate questions. All experts agreed that the final version of the questionnaire was clear and unambiguous. The survey comprised questions organized into four sections addressing sociodemographic characteristics, working conditions, self-care practices, and musculoskeletal symptoms. To identify musculoskeletal symptoms, an adapted version of the Nordic Musculoskeletal Questionnaire (NMQ), previously validated in Brazil, was used(10). The questionnaire is widely employed to assess musculoskeletal discomfort, segmenting the body into nine anatomical regions: neck, shoulders, upper back, elbows, wrists/hands, lower back, hips/thighs, knees, and ankles/feet.[10]
The survey was distributed to potential participants via WhatsApp™, accompanied by a cover letter and a link to access the survey on Google Forms™ (Google LLC, Mountain View, California, USA). A snowball sampling strategy was adopted(11), in which participants were encouraged to share the questionnaire link with other potential respondents, thereby expanding the network of participants.
All participants provided informed consent electronically through the Google Forms™ platform. Each respondent could complete the survey only once. Participation was voluntary, anonymous, and without financial compensation. The collected data were stored electronically in a password-protected system to ensure confidentiality. The data collection period lasted 4 months. Participants who did not complete the questionnaire correctly were excluded from the analysis.
Qualitative variables were described using absolute and relative frequencies, while quantitative variables were summarized using means, standard deviations, and minimum and maximum values. Inferential analyses of associations between two qualitative variables were conducted using cross-tabulations of absolute and relative frequencies, followed by the chi-squared test for independence. A significance level of 5% was adopted for all tests. Analyses were performed using Jamovi version 2.3.28, and graphs were generated using RStudio version 2023.06.2 + 561.
The statistical analysis was conducted in two stages. First, a univariate analysis was performed to compare sex, BMI, medical training, and exercise practice with the presence of musculoskeletal symptoms according to the affected body region. In this stage, BMI was analyzed categorically (<25 and ≥25 kg/m²).
Quantitative variables, specifically age and working hours, were not included in the univariate analysis; instead, they were incorporated directly into a multiple logistic regression model along with the other explanatory variables. The model considered the presence of any MSD as the dependent variable, with sociodemographic and professional characteristics as independent variables. Analyses were performed using Jamovi version 2.3.28, and graphs were generated using RStudio version 2023.06.2 + 561.
RESULTS
The study included 233 participants from all regions of Brazil, with the majority from the Northeast (n=115, 49.3%) and Southeast (n=89, 38.2%) regions. Among respondents, 82% (n=191) were trained ophthalmologists, and 18% (n=42) were second- or third-year residents. The sample consisted predominantly of female participants (n=151, 64.8%), and the mean age was 40.4 ± 11.3 years (range 25–73 years) (Table 1). No participants were excluded due to incomplete or improperly completed questionnaires.
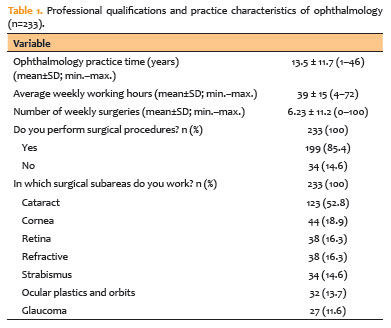
Most participants (n=128, 54.9%) had a BMI of 25 or higher, and 72.5% (n=169) reported engaging in regular exercise at least three times per week. The use of painkillers for musculoskeletal pain in the previous year was reported by 50.2% (n=117) of participants, and 38.2% (n=89) indicated that these symptoms affected their daily activities. Almost 56% (n=130) of participants reported dissatisfaction with workplace ergonomics.
The mean duration of professional practice in ophthalmology was 13.5 ± 11.7 years (range 1–46 years), and the mean weekly workload was 39.0±15 hours (range 4–72 hours). Among participants, 85.4% (n=199) performed surgical procedures, with the majority (52.8%, n=123) performing cataract surgery (Table 1). The mean number of weekly surgeries performed was 6.2 ± 11.2 (range 0–100).
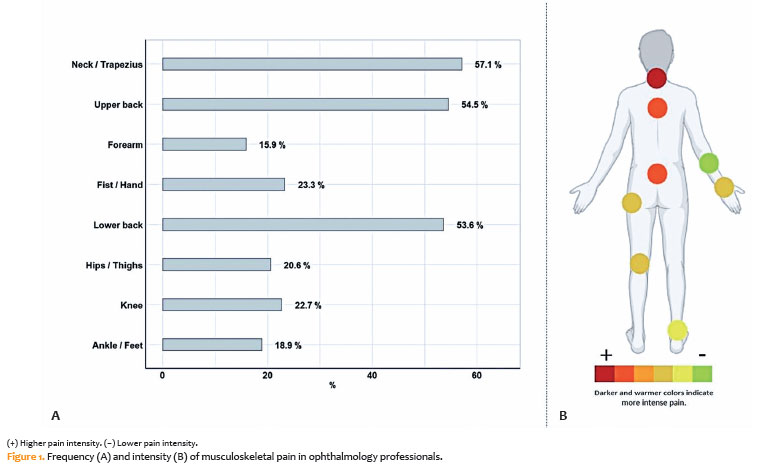
The prevalence of musculoskeletal symptoms in at least one body region was 82.4% (n=192), with the most frequently affected regions being the neck/trapezius (57.1%), upper back (54.5%), and lower back (53.6%) (Figure 1A and 1B).
The prevalence of musculoskeletal pain among participants varied according to characteristics such as sex, BMI, and physical exercise. Women reported more neck and trapezius pain (61.6%, n=93) than men (48.8%, n=40), although the difference was not statistically significant (p=0.059). No significant associations were observed between MSDs and BMI (p=0.803) or physical exercise (p=0.862) (Figures 2A–2C).
Ankle and foot pain was more common among participants with a BMI below 25 (27.6%, n=29) compared with those with a BMI of 25 or higher (11.7%, n=15), and this difference was statistically significant (p=0.002) (Figure 2B).
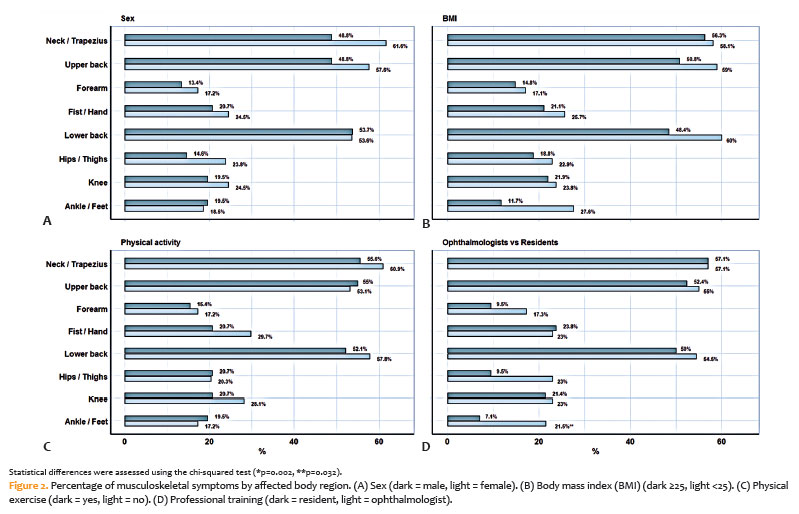
Pain in the ankles/feet and hips/thighs was more common among ophthalmologists (21.5%, n=41) than among ophthalmology residents (7.1%, n=3), and this difference was statistically significant (p=0.032) (Figure 2D).
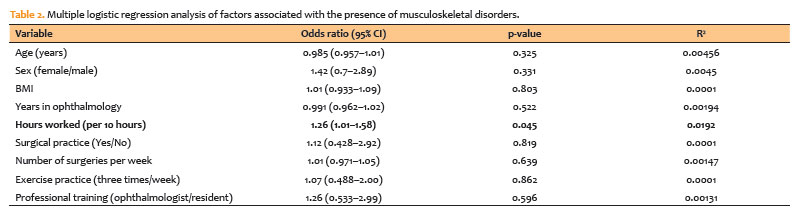
Logistic regression analysis indicated that weekly working hours were significantly associated with the presence of MSDs, with a 26% increase in the likelihood of symptoms for every additional 10 hours of work (odds ratio [OR] = 1.26, 95% confidence interval [CI] 1.01–1.58, p=0.04) (Table 2). Other variables, including surgical practice, number of weekly surgeries, regular exercise, and professional training, were not significantly associated with the presence of MSDs.
DISCUSSION
The present study highlights the high prevalence of MSDs among ophthalmologists and ophthalmology residents in Brazil. These findings are consistent with previous studies investigating MSDs in ophthalmologists in other countries, including Germany, India, and the United States(1,6,9).
Repetitive movements and sustained postures are characteristic of ophthalmology practice during slit-lamp examinations and surgical procedures. These factors are recognized as high-risk for the development of MSDs, contributing to chronic pain and functional limitations, which may reduce productivity and potentially lead to temporary absence from professional activities(1).
Previous studies have shown that the cervical, upper back, and lumbar regions are the most commonly affected body areas among ophthalmologists(1,9,12). Consistently, these regions were also identified in our study as the primary sites of musculoskeletal symptoms among Brazilian ophthalmologists. Pain of greater intensity in these areas may be associated with prolonged positioning of the upper limbs during ophthalmic examination(1). Moreover, most participants in our study reported dissatisfaction with workplace ergonomics. These findings underscore the urgency of improving working conditions to enhance ergonomics and reduce the risk of MSDs.
A recent study by Schechter et al. (2024) reported that 66% of ophthalmologists in the United States experienced work-related pain, with an average score of 4/10 on the pain scale. The authors noted that ophthalmologists with MSD symptoms spent significantly more time in surgery, highlighting the need for specific ergonomic guidance in the work environment, particularly in the operating room(9,12). In contrast, our study found no association between the frequency of MSDs and surgical practice. However, an association was observed with long working hours. Work overload and a high patient volume were identified as factors aggravating musculoskeletal symptoms, increasing the risk of repetitive strain injuries and fatigue, and negatively affecting the mental health and quality of life of professionals.
A notable aspect of this study was the predominance of female participants (65%), which may contribute to the higher prevalence of MSDs. The greater predisposition of women to musculoskeletal symptoms may be related to hormonal and social factors, as well as differences in pain perception and experience. These findings highlight the need for further research to better understand sex differences in the prevalence of MSDs among ophthalmologists(9,12).
Another noteworthy finding is the unexpected relationship between BMI and MSDs. Robert et al. (2024) reported an increased risk of MSDs among individuals with higher BMI, suggesting that a sedentary lifestyle may contribute significantly to the development of these symptoms. In our study, although most participants (54.9%, n=128) had a BMI of 25 or higher, indicating overweight or obesity(13), the relationship between BMI and MSDs was not statistically significant. Interestingly, contrary to expectations, participants with a BMI below 25 exhibited a higher prevalence of joint and foot pain. This finding suggests that biomechanics and the level of physical activity may play a more important role in the etiology of musculoskeletal pain than body weight alone.
Regular physical activity was shown to be beneficial but insufficient to prevent all musculoskeletal symptoms, highlighting the need for an integrated approach that combines physical exercise with ergonomic interventions. Fouzdar et al.(12) and Robert et al.(1) recommend modifications to ophthalmic instruments and the work environment to support healthier postures, particularly during the use of loupes and surgical procedures. These studies emphasize the importance of developing ergonomic innovations to extend the working lives of ophthalmologists and reduce the impact of MSDs on quality of life and professional performance.
This study has several limitations that should be considered when interpreting the findings. The convenience sampling methodology may have introduced some bias toward more engaged professionals or those experiencing more pronounced symptoms. However, widely distributing the questionnaire and encouraging participants to share it with colleagues aimed to minimize this potential bias. In addition, although data collection via an online questionnaire relies on self-reporting and may be subject to recall errors, the use of validated instruments, such as the NMQ, was intended to ensure the consistency and quality of responses. The cross-sectional design of the study does not allow causal relationships to be established between working conditions and the development of MSD. Nevertheless, it provides a valuable overview of symptom prevalence and associated factors.
This study demonstrated a high prevalence of MSDs among ophthalmologists and ophthalmology residents in Brazil, particularly affecting the cervical, lumbar, and upper back regions. Key contributing factors include long working hours, a high patient volume, and repetitive, awkward postures during examinations and procedures. These findings highlight the urgent need to improve ergonomic conditions and promote active lifestyles beginning in residency and continuing throughout professional practice. Raising awareness of ergonomic practices during training, combined with workplace adaptations, self-care strategies, and regular physical activity, is essential to reduce the incidence of MSD, enhance professional well-being, and support the sustainability of medical careers while mitigating potential negative impacts on public health.
Future studies employing longitudinal designs and detailed analyses of equipment use and work routines will be essential to strengthen understanding of risk factors and guide targeted interventions. Such research will facilitate the implementation of strategies to improve working conditions and optimize the quality of patient care.
AUTHORS' CONTRIBUTIONS:
Significant contribution to conception and design: Jabneel Tassiano dos Santos Nogueira, Camila Vieira Oliveira Carvalho Ventura, Michel Bittencourt Santos. Data acquisition: Jabneel Tassiano dos Santos Nogueira, Carlos Eduardo Ximenes da Cunha, Carlos Henrique de Almeida Cipriano. Data analysis and interpretation: Jabneel Tassiano dos Santos Nogueira, Taíse Maria Clemente de Araújo, Carlos Eduardo Ximenes da Cunha, Carlos Henrique de Almeida Cipriano. Manuscript drafting: Jabneel Tassiano dos Santos Nogueira, Taíse Maria Clemente de Araújo. Significant intellectual content revision of the manuscript: Jabneel Tassiano dos Santos Nogueira, Taíse Maria Clemente de Araújo, Camila Vieira Oliveira Carvalho Ventura, Michel Bittencourt Santos. Final approval of the submitted manuscript: Jabneel Tassiano dos Santos Nogueira, Taíse Maria Clemente de Araújo, Carlos Eduardo Ximenes da Cunha, Carlos Henrique de Almeida Cipriano, Camila Vieira Oliveira Carvalho Ventura, Michel Bittencourt Santos. Statistical analysis: Jabneel Tassiano dos Santos Nogueira, Taíse Maria Clemente de Araújo. Obtaining funding: Not applicable. Supervision of administrative, technical, or material support: Camila Vieira Oliveira Carvalho Ventura, Michel Bittencourt Santos. Research group leadership: Camila Vieira Oliveira Carvalho Ventura, Michel Bittencourt Santos.
REFERENCES
1. Robert R, Babu M, Sudhakar NA, Sumanth B. Digital survey assessment of individual and occupational factors associated with musculoskeletal disorders among indian ophthalmologists. J Curr Ophthalmol. 2023;35(3):281-6.
2. Epstein S, Sparer EH, Tran BN, Ruan QZ, Dennerlein JT, Singhal D, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists. JAMA Surg. 2018;153(2):e174947.
3. Vijendren A, Yung M, Sanchez J. Occupational health issues amongst UK doctors: a literature review. Occup Med. 2015;65(7):519-28.
4. Schechet SA, DeVience E, DeVience S, Shukla S, KaleemM. Survey of musculoskeletal disorders among US ophthalmologists. Dig J Ophthalmol. 2020;26(4):36-45.
5. Silva TP, Araújo WN, Stival MM, Toledo AM, Burke TN, Carregaro RL. Desconforto musculoesquelético, capacidade de trabalho e fadiga em profissionais da enfermagem que atuam em ambiente hospitalar. Rev Esc Enferm USP. 2018;52:e03332.
6. Bertelmann T, Heutelbeck A, Bopp S, Sagebiel LL, Eichberg S, Hallier E, et al. Prevalence of back pain among German ophthalmologists. Ophthalmic Res. 2021; 64(6):974-82.
7. Vitta AD, Canonici AA, Conti MH, Simeão SF. Prevalência e fatores associados à dor musculoesquelética em profissionais de atividades sedentárias. Fisioter Mov. 2012;25(2):273-80.
8. Kaup S, Shivalli S, Kulkarni U, Arunachalam C. Ergonomic practices and musculoskeletal disorders among ophthalmologists in India: An online appraisal. Eur J Ophthalmol. 2020;30(1):196-200.
9. Dhimitri KC, McGwin G Jr, McNeal SF, Lee P, Morse PA, Patterson M, et al. Symptoms of musculoskeletal disorders in ophthalmologists. Am J Ophthalmol. 2005; 139(1):179-81.
10. De Barros EN, Alexandre NM. Cross - cultural adaptation of the Nordic musculoskeletal questionnaire. Int Nurs Rev. 2003;50(2):101-8.
11. Parker C, Scott S, Geddes A. Snowball sampling [Internet]. Gloucestesrhire, England: University of Gloucestesrhire; SAGE Publications;. 2019. [cited 2025 June 19]. Available from: http://eprints.glos.ac.uk/id/eprint/6781
12. Fouzdar Jain S, Akhter S, Ishihara R, Siddicky S, High R, Suh DW. The prevalence of work-related musculoskeletal disease among pediatric ophthalmologists. Clin Ophthalmol. 2022;16:833-40.
13. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet. 2024;403(10431):1027-50.
Data Availability Statement: The datasets generated and/or analyzed during the current study are included in the manuscript.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Tiago E. Faria Arantes
*The authors contributed equally to this manuscript.
Submitted for publication:
September 15, 2025.
Accepted for publication:
February 10, 2026.
Approved by the following research ethics committee: Fundação Altino Ventura – FAV (CAAE: 76172223.9.0000.5532).
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.
Funding: This study received no specific financial support.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.