Arq. Bras. Oftalmol. 2026; 89 (3): 10.5935/0004-2749.2025-0232
Total: 445
Guilherme Barroso Guedes1; Tiago Santos Prata2,3; Matheus Pedrotti Chavez4; Augusto Paranhos Jr2
DOI: 10.5935/0004-2749.2025-0232
ABSTRACT
Repeat selective laser trabeculoplasty has emerged as a valuable option for managing intraocular pressure in patients with primary open-angle glaucoma or ocular hypertension. This review synthesizes current evidence of the efficacy, safety, and clinical applicability of repeat selective laser trabeculoplasty. Evidence from randomized controlled trials, systematic reviews, and observational studies indicate that repeat selective laser trabeculoplasty effectively sustains significant intraocular pressure reduction with minimal complications. This procedure demonstrates comparable efficacy to that of initial selective laser trabeculoplasty, supporting its role as a sustainable, drop-free management strategy. However, further research is warranted to optimize treatment intervals, assess long-term outcomes, and evaluate cost-effectiveness across different healthcare settings.
Keywords: Glaucoma; Ocular hypertension; Intraocular pressure; Selective laser trabeculoplasty
INTRODUCTION
Glaucoma and ocular hypertension (OHT) are leading causes of irreversible blindness globally, with primary open-angle glaucoma (POAG) being the most prevalent form. Elevated intraocular pressure (IOP) is the primary modifiable risk factor, and its control remains the cornerstone of glaucoma management. Pharmacological therapy has been used as the first-line treatment; however, its related issues, such as poor adherence, side effects, ocular surface disease, and economic burden, have prompted the search for alternative strategies.
Selective laser trabeculoplasty (SLT), introduced in the late 1990s, is a noninvasive, tissue-sparing approach to lowering IOP by enhancing aqueous outflow through the trabecular meshwork. Unlike argon laser trabeculoplasty, SLT involves the use of a Q-switched 532-nm Nd:YAG laser to selectively target pigmented trabecular meshwork cells, thereby minimizing thermal damage. The LiGHT trial and subsequent studies have established SLT as a viable first-line therapy, demonstrating comparable efficacy to medications with fewer side effects and improved adherence. Nevertheless, the transient nature of the efficacy of SLT in some patients requires consideration of repeat treatments to sustain long-term IOP control.
This review aimed to investigate current evidence on the effectiveness, safety, and clinical role of repeat SLT in patients with POAG or OHT.
METHODS
A comprehensive literature review was conducted, focusing on studies published in peer-reviewed journals up to May 2025. PubMed, Cochrane Library, and EMBASE databases were searched using the following keywords: "repeat SLT," "glaucoma," "ocular hypertension," "intraocular pressure," and "laser trabeculoplasty." The inclusion criteria included randomized controlled trials (RCTs), systematic reviews, meta-analyses, and observational studies evaluating repeat SLT in adult patients with POAG or OHT. The outcomes of interest were IOP reduction, effect duration, safety profile, comparison with initial SLT efficacy, and cost-effectiveness.
RESULTS AND DISCUSSION
Numerous studies affirm that repeat SLT effectively restores IOP control once the effects of the initial treatment diminish(1). Jang et al. (2021) conducted a meta-analysis of nine studies and 1,235 eyes and reported that repeat SLT achieved a mean IOP reduction of 4.1 mmHg (95% confidence interval [CI], 3.5–4.7 mmHg) at 24 months, with a success rate of 62% in maintaining target IOP without additional medications or surgery(2). These findings indicate the durability of repeat SLT, particularly in patients who responded well to initial treatment. In addition, repeat SLT has demonstrated comparable efficacy to that of an initially successful SLT and remained effective even in cases where the initial treatment yielded suboptimal results. A summary of key studies evaluating repeat SLT is presented in table 1.
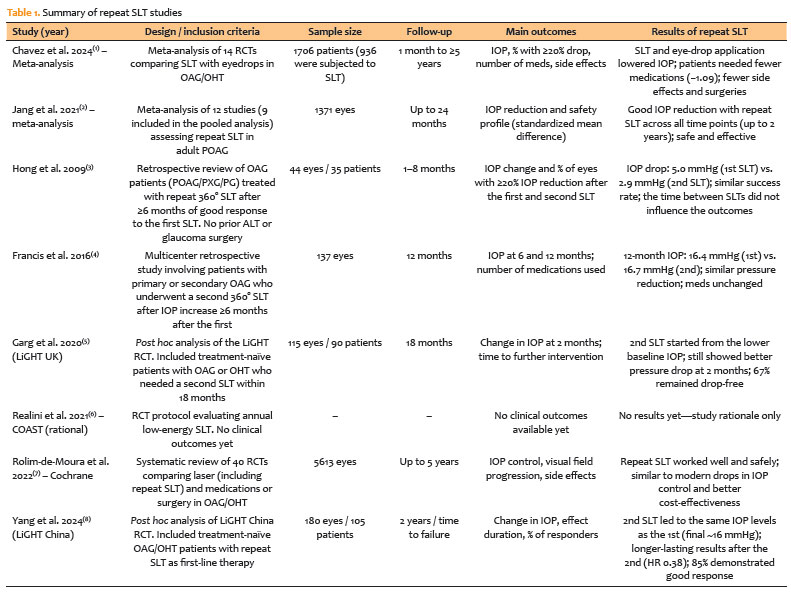
A post hoc analysis of the LiGHT trial evaluated 115 eyes that underwent repeat SLT(3). The mean IOP before the initial SLT was 22.1 mmHg, whereas that before repeat SLT was 18.7 mmHg. The adjusted IOP reduction at 2 months post-repeat SLT was 5.3 mmHg, compared with 4.2 mmHg after the initial SLT, suggesting greater efficacy when baseline pressures were considered. At 18 months post-repeat SLT, 67% of the eyes remained medication-free, indicating that it can sustain drop-free control over extended periods.
The LiGHT trial post hoc analysis also suggests that early IOP outcomes within the first two months after initial SLT do not reliably predict the success of subsequent repeat SLT. Eyes with limited early response may still achieve effective, drop-free pressure control after retreatment, indicating that a lack of early IOP reduction should not preclude future SLT repetition.(3) Moreover, caution should be exercised to avoid premature treatment escalation while still aiming to achieve strict, individualized target IOP levels.
Hong et al. (2009) examined 44 eyes and reported a mean IOP reduction of 5.0 mmHg after the initial SLT and 2.9 mmHg after repeat SLT at 3 months, with success rates (defined as ≥20% IOP reduction) of 55% and 50%, respectively(4). Notably, the interval between treatments (whether 6–12 months or >12 months) did not markedly influence the outcomes, supporting individualized retreatment timing tailored to each patient's needs.
Francis et al. (2016) analyzed 137 patients and found that the baseline IOP decreased from 20.3 ± 5.2 to 16.4 ± 3.9 mmHg after the initial SLT and from 19.4 ± 5.0 to 16.7 ± 4.7 mmHg after repeat SLT at 12 months (p<0.001)(5). A subanalysis of 62 matched patients revealed consistent efficacy, supporting the repeatability of SLT as a viable long-term IOP-lowering strategy.
Emerging strategies advocate for proactive, scheduled low-energy SLT to maintain long-term IOP control and minimize the need for medications. In Gandolfi's cohort, annual repetition of low-energy SLT resulted in 58.3% of patients remaining medication-free after 10 years, compared with 25.0% in standard SLT protocols (p<0.001). This proactive approach is potentially beneficial in that it can prevent IOP fluctuations and disease progression. The COAST, an ongoing randomized trial, has compared annual administration of repeat SLT at low energy and administration as needed at standard energy in treatment-naïve patients(6). Long-term data are awaited to evaluate the applicability of this strategy.
Safety profiles were consistent across studies. Jang et al. (2021) reported transient IOP spikes in 4% of cases, typically resolving within 24 h with conservative management(2). There were no cases of peripheral anterior synechiae or significant inflammation. Based on a real-world Brazilian study, repeat SLT was performed in 73 eyes (15.9%) without sight-threatening complications, supporting its safety(9). The Cochrane Review confirmed that SLT, including repeat procedures, had fewer systemic side effects than medications and achieved a favorable cost–benefit ratio, particularly in healthcare systems strained by the high costs of medications(7).
In addition to its efficacy and safety, repeat SLT markedly enhances patients' quality of life by reducing reliance on daily eyedrops, which is often associated with ocular surface disease, preservative toxicity, and poor adherence rates, reported to be as low as 50% in some studies(8).
However, challenges persist. First, the optimal retreatment timing remains unstandardized, with current practice being largely reactive-initiated only after IOP increase or disease progression. Therefore, predictive markers are needed to identify patients who would benefit the most from early or scheduled retreatments. Second, data on the efficacy and safety of third, fourth, or annual SLT sessions remain scarce, necessitating further long-term prospective studies.
Economic evaluations are also crucial. Although SLT has proven cost-effective compared with medications, particularly in healthcare systems facing high medication costs, comprehensive analyses of repeat SLT protocols across different regions and healthcare models are lacking.
In conclusion, repeat SLT is a safe, effective, and repeatable therapeutic option for sustaining IOP control in patients with OAG or OHT. It significantly reduces medication burden, improves adherence, enhances patients' quality of life, and potentially lowers long-term healthcare costs. Growing evidence supports its integration into routine glaucoma management, particularly within a laser-first treatment paradigm.
Future research should define standardized retreatment protocols, investigate the long-term outcomes of multiple SLT sessions, and conduct comprehensive cost-effectiveness analyses across diverse populations and healthcare systems. Individualized strategies guided by patient-specific risk factors, response patterns, and predictive biomarkers may further enhance the role of repeat SLT in glaucoma management. In addition, ongoing trials, such as the COAST, will be instrumental in elucidating the optimal application of SLT therapy, potentially shifting the paradigm toward proactive laser management.
AUTHORS' CONTRIBUTIONS
Significant contribution to conception and design: Guilherme Barroso Guedes, Tiago Santos Prata, Augusto Paranhos Jr. Data acquisition: Guilherme Barroso Guedes, Tiago Santos Prata, Matheus Pedrotti Chavez, Augusto Paranhos Jr. Data analysis and interpretation: Guilherme Barroso Guedes, Tiago Santos Prata. Manuscript drafting: Guilherme Barroso Guedes. Significant intellectual content revision of the manuscript: Guilherme Barroso Guedes, Tiago Santos Prata, Matheus Pedrotti Chavez, Augusto Paranhos Jr. Final approval of the submitted manuscript: Guilherme Barroso Guedes, Tiago Santos Prata, Matheus Pedrotti Chavez, Augusto Paranhos Jr. Statistical analysis: Guilherme Barroso Guedes. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Augusto Paranhos Jr. Research group leadership: Augusto Paranhos Jr.
REFERENCES
1. Chavez MP, Guedes GB, Pasqualotto E, Lopes LM, Ferreira RO, de Souza ES, et al. Selective laser trabeculoplasty versus medical therapy for the treatment of open angle glaucoma or ocular hypertension: a systematic review and meta-analysis of randomized controlled trials. J Glaucoma. 2024;33(12):973-86.
2. Jang HJ, Yu B, Hodge W, Malvankar-Mehta MS. Repeat selective laser trabeculoplasty for glaucoma patients: a systematic review and meta-analysis. J Curr Glaucoma Pract. 2021;15(3):117-24.
3. Garg A, Vickerstaff V, Nathwani N, Garway-Heath D, Konstantakopoulou E, Ambler G, et al. Efficacy of repeat selective laser trabeculoplasty in medication-naive open-angle glaucoma and ocular hypertension during the LiGHT trial. Ophthalmology. 2020;127(4):467-76.
4. Hong BK, Winer JC, Martone JF, Wand M, Altman B, Shields B. Repeat selective laser trabeculoplasty. J Glaucoma. 2009;18(3):180-3.
5. Francis BA, Loewen N, Hong B, Dustin L, Kaplowitz K, Kinast R. Repeatability of selective laser trabeculoplasty for open-angle glaucoma. BMC Ophthalmol. 2016;16(1):128.
6. Realini T, Gazzard G, Latina M, Kass M. Low-energy selective laser trabeculoplasty repeated annually: rationale for the COAST Trial. J Glaucoma. 2021;30(7):545-51.
7. Rolim-de-Moura CR, Paranhos A Jr, Loutfi M, Burton D, Wormald R, Evans JR. Laser trabeculoplasty for open-angle glaucoma and ocular hypertension. Cochrane Database Syst Rev. 2022;8(8):CD003919.
8. Yang Y, Xu K, Chen Z, Zhang Y, Ye Q, Ping YT, Fan Y, Liu P, Nathwani N, Jiang Y, Gazzard G, Yu M; LiGHT China Trial Study Group. Responsiveness to selective laser trabeculoplasty in open-angle glaucoma and ocular hypertension. JAMA Ophthalmol. 2024;142(10):918-24.
9. Abe RY, Maestrini HA, Guedes GB, Nascimento MM, Iguma CI, de Miranda Santos HD, et al. Real-world data from selective laser trabeculoplasty in Brazil. Sci Rep. 2022;12(1):1923.
Data Availability Statement: The datasets generated and/or analyzed during the current study are included in the manuscript.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Submitted for publication:
September 22, 2025.
Accepted for publication:
October 8, 2025.
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.