Arq. Bras. Oftalmol. 2025; 88 (3): 10.5935/0004-2749.2025-0048
Total: 1596
Gustavo Rosa Gameiro1; Maura Abraham-Marin1; Zelia Maria Correa1,2
DOI: 10.5935/0004-2749.2025-0048
Dear Editor,
We read with great interest the article by Carvalho et al., describing the use of congenital hypertrophy of the retinal pigment epithelium (CHRPE) as a phenotypic marker for familial adenomatous polyposis (FAP)(1). The study highlights the importance of CHRPE as a risk factor for FAP, particularly in cases with bilateral fish-tail lesions(2,3). This is an informative and important finding that motivated us to add further insights into the clinical spectrum of retinal pigment epithelium (RPE) hypertrophy through a review of the three distinct presentations. Knowledge of these is critical for accurate diagnosis and differentiation.
1. Solitary RPE hypertrophy (Figures 1A and 1B): Although these are sometimes called CHRPE, they have not been definitively proven to be congenital. They appear as single, broad-base gray-black spots in fundus photography and are commonly located in the peripheral retina. They are characterized by sharp margins and a shadow effect that mimics thickness, making these an important differential diagnosis with choroidal melanoma. Some chronic lesions may present with patches of lost melanin pigment, leading to lacunae that can enlarge over time. These lesions are sporadic, asymptomatic, and predominantly located in the fundus periphery. They are not associated with systemic conditions. Rare instances have been reported of neoplasms such as melanoma and adenocarcinoma arising de novo from extensive RPE(4,5).
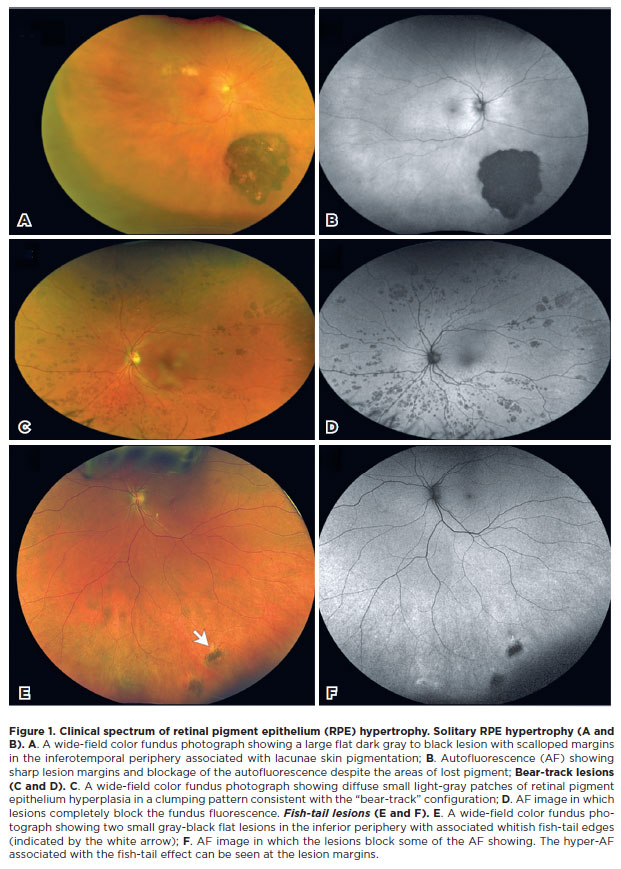
2. Bear-track lesions (Figures 1C and 1D): Bear-track lesions are so named because they manifest as clusters of small pigmented lesions resembling bear paw prints. While congenital, bear tracks are sporadic and unrelated to FAP. Their lack of any specific systemic associations and the absence of fish-tail depigmentation distinguish them from FAP-associated CHRPE.
3. Fish-tail lesions (Figure 1E and 1F): These ovoid lesions exhibit a unique fish-tail-like area of depigmentation at one margin. They are most often associated with FAP. Their bilaterality and tendency to appear as multiple lesions (typically 2–6 per eye) make them a significant phenotypic marker for this condition. Recognizing these features is essential for early identification and screening of at-risk patients.
We believe a more detailed discussion of these forms of RPE hypertrophy would add to the utility of Carvalho et al.'s findings and assist your readers in distinguishing between FAP-associated lesions and other RPE abnormalities.(2)
We also feel that the use of the term "congenital" in this context is problematic as there is no evidence to indicate, which if any of these variations are truly congenital. The lesions are known to grow in more than 50% of cases. In clinics, patients with RPE hypertrophy merit an annual fundus evaluation to monitor for lesion enlargement and the other aforementioned risks.
We commend the authors for their significant contribution and for raising awareness of CHRPE as an important screening finding. We hope the points we have made will broaden the discussion of this condition and further emphasize the importance of early diagnosis and multidisciplinary approaches to hereditary syndromes like FAP.
REFERENCES
1. Carvalho AA, Crespo TS, Násser LS, Maia CM, Fonseca CA, Silveira CM, et al. Use of congenital hypertrophy of the retinal pigment epithelium as a clinical sign of familial adenomatous polyposis. Arq Bras Oftalmol. 2024;88(3):S0004-27492025000300300.
2. Traboulsi EI, Maumenee IH, Krush AJ, Giardiello FM, Levin LS, Hamilton SR. Pigmented ocular fundus lesions in the inherited gastrointestinal polyposis syndromes and in hereditary nonpolyposis colorectal cancer. Ophthalmology. 1988;95(7):964-9.
3. Bonnet LA, Conway RM, Lim LA. Congenital Hypertrophy of the Retinal Pigment Epithelium (CHRPE) as a screening marker for Familial Adenomatous Polyposis (FAP): systematic literature review and screening recommendations. Clin Ophthalmol. 2022;16:765-74.
4. Salmon B, Schalenbourg A. "De novo" appearance of a choroidal melnoma during 5 years' follow-up for CHRPE. Klin Monbl Augenheilkd. 2022;239(4):590-2.
5. Trichopoulos N, Augsburger JJ, Schneider S. Adenocarcinoma arising from congenital hypertrophy of the retinal pigment epithelium. Graefes Arch Clin Exp Ophthalmol. 2006;244(1):125-8.
AUTHORS' CONTRIBUTIONS:
Significant contribution to conception and design: Gustavo Rosa Gameiro, Maura Abraham-Marin, Zelia Maria Correa. Data acquisition: Gustavo Rosa Gameiro, Maura Abraham-Marin, Zelia Maria Correa. Data analysis and interpretation: Gustavo Rosa Gameiro, Maura Abraham-Marin, Zelia Maria Correa. Manuscript drafting: Gustavo Rosa Gameiro, Maura Abraham-Marin, Zelia Maria Correa Significant intellectual content revision of the manuscript: Zelia Maria Correa. Final approval of the submitted manuscript: Gustavo Rosa Gameiro, Maura Abraham-Marin, Zelia Maria Correa. Statistical analysis: not applicable. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Zelia Maria Correa. Research group leadership: Zelia Maria Correa.
Submitted for publication:
February 10, 2025.
Accepted for publication:
February 11, 2025.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.
Funding: This study received no specific financial support.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.