Arq. Bras. Oftalmol. 2025; 88 (2): 10.5935/0004-2749.2023-0185
Total: 2759
Clarissa R. Pereira1; Thais S. A. Benassi1; Luiz Guilherme M. Mello1,2; Leonardo P. Cunha1,3; Rony Carlos Preti1; Leandro C. Zacharias1; Eduardo C. de Souza1; Mário L. R. Monteiro1
DOI: 10.5935/0004-2749.2023-0185
ABSTRACT
Optic neuritis is an important cause of unilateral and acute visual loss in young adults, but other differential diagnoses should be considered, especially when the disease has an atypical presentation. This report presents the case of a young woman with reduced visual acuity in her right eye, associated with optic disc edema and a relative afferent pupillary defect, that was initially misdiagnosed as optic neuritis and subsequently found to have paracentral acute middle maculopathy, possibly secondary to subtle impending central retinal vein occlusion. This case emphasizes the need to remember that retinal vascular diseases can occasionally mimic optic neuritis. Detailed anamnesis and ophthalmic examination can avoid unnecessary interventions.
Keywords: Optic disc; Papilledema; Optic neuritis; Retinal diseases; Diagnosis, differential; Visual acuity; Diagnostic errors
INTRODUCTION
Optic neuritis (ON) is an important cause of acute unilateral visual loss in young adults, which usually requires extensive neurologic investigation and urgent treatment to prevent permanent visual loss(1). However, the differential diagnoses of other ocular and optic nerve conditions are necessary to prevent inadequate management.
Here, we describe the case of a young woman who presented with episodes of transient visual loss followed by permanent visual impairment and central scotoma in her right eye (OD), which was associated with pain, optic disc edema, and a relative afferent pupillary defect (RAPD).
The initial suspicion of ON was dismissed after carefully evaluating the clinical history, ophthalmologic examination, and optical coherence tomography (OCT) that established the diagnosis of paracentral acute middle maculopathy (PAMM).
CASE REPORT
A 32-year-old Caucasian woman presented to our service after 3 weeks of subacute visual loss in the OD. She reported the occurrence of painless central visual blurring in this eye thrice daily for three consecutive days that lasted up to 60 min, with spontaneous and complete improvement.
On the fourth day, visual blurring persisted, and she began to experience pain with eye movement. She also described paresthesia on the ipsilateral hemiface, dizziness, tinnitus, and worsening vision during exercises, but denied motor disabilities, nausea, vomiting, or hiccups.
Past medical history revealed migraine, long-standing joint pain in her left knee, which was occasionally treated with oral nonsteroidal anti-inflammatory drugs, and oral contraceptive use. Thus, she went to a clinical emergency department where she underwent computed tomography (CT), and the patient was discharged after receiving pain medication. However, visual blurring persisted, and she consulted an ophthalmologist who observed mild disc edema in her OD and some vascular congestion, and she was referred for a neuro-ophthalmologic evaluation. After 2 weeks, she was examined by a neuro-ophthalmologist who reported a best-corrected visual acuity (BCVA) of 20/40 in the OD and 20/20 in the left eye (OS), right RAPD, and mild optic disc edema associated with peripapillary hemorrhages inferiorly in OD. Therefore, ON was considered, and she was urgently referred to our service.
After 1 week, the patient came to our service reporting some improvement, but she still complained of a central blur. BCVA was 20/20 in both eyes, with difficulty in the OD, and a mild right RAPD was also detected. Eye movements, slit lamp examination, and intraocular pressure were unremarkable. Fundus examination showed mild optic disc edema, few peripapillary hemorrhages, and a discrete pigmentary abnormality in the macula (Figure 1). Compared with the contralateral eye, a small candle-flame-shaped hemorrhage in the superior temporal arcade and mild venous engorgement in the OD were found.

Automated visual field analysis showed a small paracentral relative scotoma in the OD (Figure 2) and was unremarkable in the OS. No significant abnormalities were found in fluorescein angiography of both eyes.
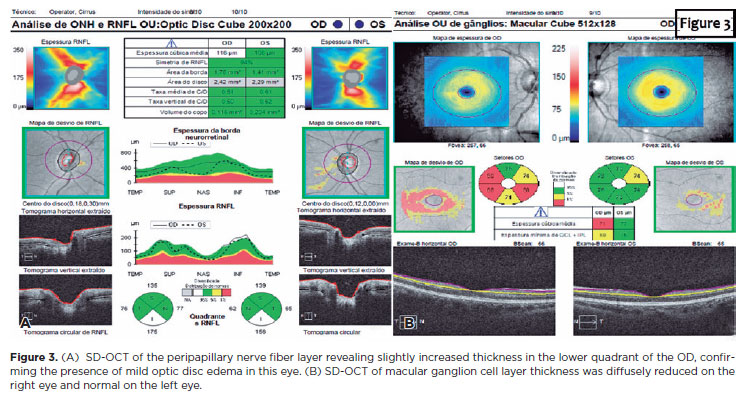
The OCT revealed an increased thickness of the peripapillary retinal nerve fiber layer (pRNFL) and diffuse thinning of the macular ganglion cell layer in OD (Figure 3A), which supported the suspicion of mild optic disc edema (Figure 3B).
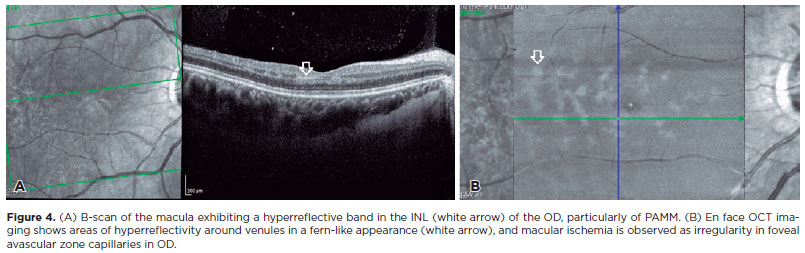
A cross-sectional B-scan of the macula showed a hyperreflective parafoveal band in the inner nuclear layer (INL) of the OD, and the patient was diagnosed with PAMM (Figure 4A). OCT angiography revealed an attenuation of the parafoveal deep vascular complex, reinforcing the hypothesis of PAMM. The en face OCT image showed areas of hyperreflectivity around the venules in a fern-like appearance and an irregularity in the capillaries of the foveal avascular zone, denoting macular ischemia in OD (Figure 4B).
No abnormalities were found in cerebrospinal fluid analysis, brain magnetic resonance imaging with angiography, Doppler ultrasound of the carotid and vertebral arteries, and laboratory results.
DISCUSSION
Initially, PAMM was described as a variant of acute macular neuroretinopathy (AMN)(2). With the development of spectral-domain OCT (SD-OCT), PAMM was distinguished from AMN because of the preferential involvement of the inner rather than the outer retina, characterized by the development of a parafoveal hyperreflective band in the INL of the retina on OCT(2,3).
The mechanism of PAMM is unclear, but middle retinal ischemia may occur due to reduced blood flow in the deep and intermediate capillary plexuses(2-5). The INL of the retina is a region of a functional watershed zone due to its relative distal location to the inner retinal circulation and choriocapillaris. When the blood supply decreases, the oxygen tension increases in the superficial layers of the retina and choroid, making this intermediate region more susceptible to ischemia(4). In line with this theory, PAMM was frequently associated with other retinal vascular diseases, such as retinal vessel occlusion and sickle cell retinopathy(6-8).
Patients' complaints are often devalued because of normal visual acuity and subtle fundus abnormalities(3). Therefore, knowing the clinical spectrum of PAMM is important to promote suspicion in the acute phases of the disease, proceeding with an active investigation through SD-OCT, which is essential for the diagnosis(2,3).
PAMM has also been associated with other conditions, such as drug intake (amphetamines, vasopressors, caffeine, and oral contraceptives), migraine, hypovolemia, orbital compression, viral infections, and vaccination(2,3,5). Recently, PAMM was associated with SARS-CoV-2 infection and vaccination(9). Notably, COVID-19 increases the risk of vascular thrombotic events, including retinal circulation; thus, PAMM can be a possible complication(9).
Currently, PAMM has no specific treatment, but patients should be educated about controllable risk factors to prevent further vascular events, such as the involvement of the other eye(10).
Although some initial features of our case suggested ON, particularly the presence of optic disc edema and RAPD, other clinical and fundoscopic findings pointed to a vascular etiology. Moreover, OCT was essential to characterize PAMM.
The exact mechanism for the development of the ischemia in our case remains unclear, but it was most likely related to impending central retinal vein occlusion and oral hormonal contraceptive use.
In conclusion, this case documents a possible confusion between ON and retinal vascular disease, emphasizing the importance of a careful evaluation to determine the correct diagnosis of acute visual loss in young patients, avoiding unnecessary testing and treatment.
ACKNOWLEDGMENT
This study was supported by CAPES - Coordenação de Aperfeiçoamento de Nível Superior, Brasília, Brazil, and CNPq - Conselho Nacional de Desenvolvimento Científico e Tecnológico, (No 308172/2018-3), Brasília, Brazil.
AUTHORS' CONTRIBUTION
Significant contribution to conception and design: Clarissa R. Pereira, Thais A. S. Benassi, Luiz Guilherme M. Mello, Leonardo P. Cunha, Rony Carlos Preti, Leandro C. Zacharias, Eduardo C. Souza, Mario L. R. Monteiro. Data acquisition: Clarissa R. Pereira, Thais A. S. Benassi, Mario L. R. Monteiro. Data analysis and interpretation: Clarissa R. Pereira, Thais A. S. Benassi, Luiz Guilherme M. Mello, Leonardo P. Cunha, Rony Carlos Preti, Leandro C. Zacharias, Eduardo C. Souza, Mario L. R. Monteiro. Manuscript drafting: Clarissa R. Pereira, Mario L. R. Monteiro. Significant intellectual content revision of the manuscript: Clarissa R. Pereira, Thais A. S. Benassi, Luiz Guilherme M. Mello, Leonardo P. Cunha, Rony Carlos Preti, Leandro C. Zacharias, Eduardo C. Souza, Mario L. R. Monteiro. Final approval of the submitted manuscript: Clarissa R. Pereira, Thais A. S. Benassi, Luiz Guilherme M. Mello, Leonardo P. Cunha, Rony Carlos Preti, Leandro C. Zacharias, Eduardo C. Souza, Mario L. R. Monteiro. Statistical analysis: not applicable. Obtaining funding: Mario L. R. Monteiro Supervision of administrative, technical, or material support: Mario L. R. Monteiro Research group leadership: Mario L. R. Monteiro.
REFERENCES
1. Petzold A, Fraser CL, Abegg M, Alroughani R, Alshowaeir D, Alvarenga R, et al. Diagnosis and classification of optic neuritis. Lancet Neurol. 2022;21(12):1120-34.
2. Sarraf D, Rahimy E, Fawzi AA, Sohn E, Barbazetto I, Zacks DN, et al. Paracentral acute middle maculopathy: a new variant of acute macular neuroretinopathy associated with retinal capillary ischemia. JAMA Ophthalmol. 2013;131(10):1275-87.
3. Rahimy E, Kuehlewein L, Sadda SR, Sarraf D. Paracentral Acute Middle Maculopathy: What We Knew Then and What We Know Now. Retina. 2015;35(10):1921-30.
4. Rahimy E, Sarraf D, Dollin ML, Pitcher JD, Ho AC. Paracentral acute middle maculopathy in nonischemic central retinal vein occlusion. Am J Ophthalmol. 2014;158(2):372-380.e1.
5. Chen X, Rahimy E, Sergott RC, Nunes RP, Souza EC, Choudhry N, et al. Spectrum of Retinal Vascular Diseases Associated With Paracentral Acute Middle Maculopathy. Am J Ophthalmol. 2015;160(1):26-34.e1.
6. Sridhar J, Shahlaee A, Rahimy E, Hong BK, Khan MA, Maguire JI, et al. Optical Coherence Tomography Angiography and En Face Optical Coherence Tomography Features of Paracentral Acute Middle Maculopathy. Am J Ophthalmol. 2015;160(6):1259-1268.e2.
7. Christenbury JG, Klufas MA, Sauer TC, Sarraf D. OCT Angiography of paracentral acute middle maculopathy associated with central retinal artery occlusion and deep capillary ischemia. ophthalmic surg lasers imaging retina. 2015;46(5):579-81.
8. Nemiroff J, Kuehlewein L, Rahimy E, Tsui I, Doshi R, Gaudric A, et al. Assessing deep retinal capillary ischemia in paracentral acute middle maculopathy by optical coherence tomography angiography. Am J Ophthalmol. 2016;162:121-32.e1.
9. Castro CS, Ferreira AS, Silva NP, Lume MR, Furtado MJ. Paracentral acute middle maculopathy after COVID-19: multimodal evaluation. Retin Cases Brief Rep. 2023;17(6):791-6.
10. Maltsev DS, Kulikov AN, Burnasheva MA, Chhablani J. Prevalence of resolved paracentral acute middle maculopathy lesions in fellow eyes of patients with unilateral retinal vein occlusion. Acta Ophthalmol. 2020;98(1):e22-8.
Submitted for publication:
July 17, 2023.
Accepted for publication:
March 1, 2024.
Approved by the following research ethics committee: Hospital das Clinicas da Faculdade de Medicina da Universidade de Sao Paulo (CAAE: 66585623.2.0000.0068).
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.