Arq. Bras. Oftalmol. 2023; 86 (6): 10.5935/0004-2749.2023-1006
Total: 2371
Fernando Procianoy1; Antonio Augusto Velasco e Cruz2
DOI: 10.5935/0004-2749.2023-1006
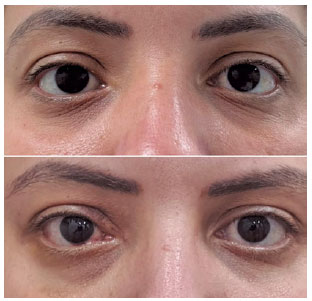
Orbital decompression is a recognized oculoplastic surgery procedure, initially used for treating compressive optic neuropathy and facial disfigurement in thyroid eye disease(1-5). The advancement of techniques and integration of technology have resulted in safer, more efficient procedures. Currently, surgeons can choose to remove orbital fat and/or reshape several orbital bone walls in different ways and combinations to achieve desired outcomes. These advancements have ushered in a new era of orbital surgery, targeting exophthalmos reduction in patients with or without thyroid eye disease (Figure 1), even without compressive orbitopathy(6,7).
Despite alterations in patient profiles and indications, surgeons persist in using the term "orbital decompression" to refer to this wide variety of diseases and surgical indications. In an era where monoclonal antibody treatments also address exophthalmos reduction, it might be time to rethink the naming of surgical procedures based on their main indications. The term "orbital decompression" seems incorrect when used for a procedure conducted in an orbit without any compression symptoms such as optic neuropathy or vascular congestion.
Most of the orbital surgeries we perform today on patients with thyroid eye disease aim to reduce exophthalmos, without any actual orbital compression. For this patient profile, expectations and concerns differ from patients with sight-threatening diseases or significant functional issues such as diplopia. The differences in surgeon and patient expectations, procedure selection, and postoperative care require distinguishing between these two types of procedures-for patient comprehension, accurate documentation, and even for billing purposes.
Therefore, we suggest using the term "orbital resizing" for exophthalmos-reduction procedures performed on patients without actual orbital compression, at the discretion of each surgeon.
REFERENCES
1. Baylis HI, Call NB, Shibata CS. The transantral orbital decompression (Ogura technique) as performed by the ophthalmologist: a series of 24 patients. Ophthalmology. 1980;87(10):1005-12.
2. Anderson RL, Linberg JV. Transorbital approach to decompression in Graves' disease. Arch Ophthalmol. 1981;99(1):120-4.
3. Hurwitz JJ, Birt D. An individualized approach to orbital decompression in Graves' orbitopathy. Arch Ophthalmol. 1985;103(5):660-5.
4. Shorr N, Seiff SR. The four stages of surgical rehabilitation of the patient with dysthyroid ophthalmopathy. Ophthalmology. 1986; 93(4):476-83.
5. Fells P. Orbital decompression for severe dysthyroid eye disease. Br J Ophthalmol. 1987;71(2):107-11.
6. Fatourechi V, Garrity JA, Bartley GB, Bergstralh EJ, DeSanto LW, Gorman CA. Graves ophthalmopathy. Results of transantral orbital decompression performed primarily for cosmetic indications. Ophthalmology. 1994;101(5):938-42.
7. Limongi RM, Feijó ED, Rodrigues Lopes E Silva M, Akaishi P, Velasco E Cruz AA, Christian Pieroni-Gonçalves A, et al. Orbital bone decompression for non-thyroid eye disease proptosis. Ophthalmic Plast Reconstr Surg. 2020;36(1):13-6.
Submitted for publication:
September 25, 2023.
Accepted for publication:
October 10, 2023.
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.