INTRODUCTION
The removal of a diseased eye is an aggressive intervention pre formed as a last resort, often for the treatment of infections refractory to medical management, malignant tumors, or blind painful eyes. Recommendation for eye removal can be very difficult for both patients and ophthalmologists.
Evisceration is the surgical removal of the eye's contents, with the exception of the sclera and extraocular muscles. It is indicated in the treatment of resistant endophthalmitis and in blind painful eyes after the possibility of a malignant tumor has been excluded. Enucleation involves complete removal of the globe from the orbit, leaving the other orbital structures intact. When a malignant intraocular tumor is suspected and other treatment modalities are not available or indicated, enucleation is often the intervention of choice. Exenteration involves complete removal of all orbital contents. This procedure is generally reserved for treating eyes with orbital disease, including ocular tumors1-4.
Multiple studies demonstrate that surgical indications for eye removal vary widely, depending on the availability of alternative treatment modalities such as radiotherapy, referral practices, and the prevalence of the disease in question5-10. In developing countries, access to funding and expertise can also affect treatment.
Few studies have addressed the issue of the frequency and indications of eye removal in Brazil. Here we present Latin America's largest and longest retrospective analysis to review the indications and types of eye removal preformed.
METHODS
All surgical pathological reports during the period from January 1, 2000, to December 31, 2012, in the database of the Ophthalmology Department at the Universidade Federal de São Paulo's (UNIFESP) Hospital were reviewed that contained at least one of the following keywords: eye, orbit, eyelid, ocular, or conjunctiva. Patients' charts were reviewed to determine the patient's age and sex, the anatomical structure from which the specimen was taken, the surgical procedure performed to obtain the specimen, the pathologist's diagnosis, and whether an evisceration, enucleation, or exenteration was performed. If all data points were available, the de-identified patient information was included in the study.
RESULTS
Over this 13-year study period, 3446 unique patient ophthalmo logical specimens were received at the Pathology Department coming from the Ophthalmology Department of the UNIFESP Hospital, of which 412 specimens were associated with eye-removal procedures. This represents 12% of the total number of surgical oph thalmological specimens.
The number of eye-removal procedures varied each year. From 2000 through 2012, the total number of eye-removal procedures per year fluctuated from eight to 81 (Figure 1). The most common indications for eye removal as well as the number of each procedure type for each indication are featured in table 1. The seven indications listed in table 1 accounted for 85.2% of the total eye-removal procedures performed across the 13-year study period. The indications in the remaining 61 eyes (14.8%) consisted of various other pathologies. Seven pathologies were associated with between two and five eyes (Table 3), and 42 pathologies were associated with only one eye (Table 4).
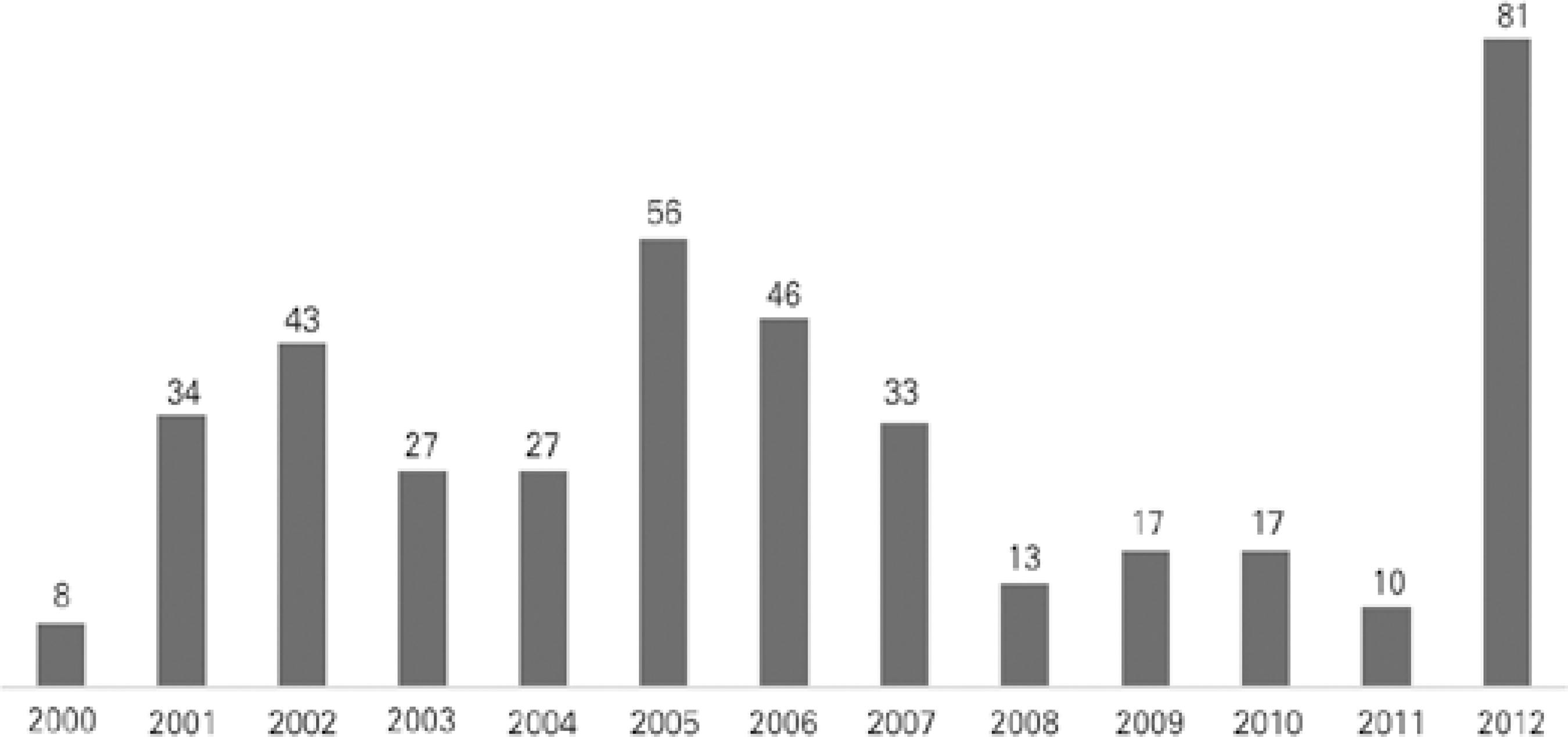
Table 1 Frequent indications for eye removal
| Diagnosis | Nº of cases | Evisceration | Enucleation | Exenteration |
|---|---|---|---|---|
| Melanoma | 146 | 00 | 135 | 11 |
| Retinoblastoma | 128 | 00 | 128 | 00 |
| Endophthalmitis | 026 | 11 | 015 | 00 |
| Nonspecific inflammation | 017 | 12 | 005 | 00 |
| Squamous cell carcinoma | 015 | 00 | 012 | 03 |
| Panophthalmitis (acute) | 014 | 00 | 014 | 00 |
| Phthisis bulbi | 005 | 05 | 000 | 00 |
Table 2 Age and sex information
| Diagnosis | Age range (years) | Mean age (years) | Male | Female | Sex unknown |
|---|---|---|---|---|---|
| Melanoma | 19-93 | 51.5 | 81 | 65 | 0 |
| Retinoblastoma | 0.33-27 | 02.7 | 84 | 61 | 3 |
| Endophthalmitis | 27-102 | 59.5 | 13 | 13 | 0 |
| Nonspecific inflammation | 5-82 | 41.1 | 09 | 08 | 0 |
| Squamous cell carcinoma | 35-84 | 51.5 | 12 | 03 | 0 |
| Panophthalmitis (acute) | 15-83 | 53.7 | 11 | 03 | 0 |
| Phthisis bulbi | 01-79 | 21.2 | 03 | 02 | 0 |
Table 3 Frequency of less common indications for eye removal
| Diagnosis | Frequency |
|---|---|
| Nonspecified carcinoma | 5 |
| Coats' disease | 4 |
| Basal cell carcinoma | 2 |
| Keratosis | 2 |
| Blood clot (embolic, thrombotic) | 2 |
| Medulloepitheliomas | 2 |
| Melanocytoma | 2 |
Table 4 Single patient diagnoses
| Actinic keratosis | Malformation of the anterior chamber | Organized hemorrhage of origin probably from pyogenic granuloma |
| Acute keratitis | Malignancy | Organized subretinal bleeding (hemorrhage). Fibrovascular subretinal membrane |
| Acute uveitis | Malignancy of blue cells | Recent hemorrhage |
| Adenoid cystic carcinoma | Malignancy undifferentiated with extraocular extensions | Retinal atrophy, retinochoroiditis scars, fibrosis with neovascularization, vitreous hemorrhage |
| Choroid hemangioma | Medulloepitheliomas teratoid | Sebaceous carcinoma |
| Chronic cerato-scleritis | Medulloepitheliomas teratoid ciliary body | Sebaceous glands carcinoma |
| Chronic iridocyclitis | Melanocytoma ciliary body | Shred of ocular conjunctiva with large hemorrhagic areas |
| Chronic keratitis | Metastasized carcinoma committing choroid, ciliary body, and iris | Traumatic perforation of the ocular globe |
| Ciliary body adenocarcinoma | Metastasized hepatocellular carcinoma | Trichoblastic carcinoma |
| Circumscribed choroidal hemangioma. Subretinal hemorrhage. Atrophic retina and optic nerve |
Metatypical carcinoma | Undetermined histogenesis neoplasia |
| Corneal drilling with disruption of ocular structures and choroid | Microfocus calcification at cribriform level | Undetermined histogenesis neoplasia with large areas of necrosis and hemorrhage |
| Diffuse uveoscleritis not granulomatous | Mucoepidermoid carcinoma | Without residual neoplasia |
| Glaucoma | Neoplasms 100% necrotic | Xanthogranuloma juvenile |
| Keratitis interstitial | Ocular globe malformation |
Of the 412 patients who underwent eye-removal procedures, 234 (56.8%) were male and 175 (42.5%) were female. Three patients (0.7%) with retinoblastoma had absent information regarding sex. The patients' age ranged between 4 months and 102 years, with a mean of 34.8 years. Table 2 provides an overview of patients' age and sex for the seven most common indications for eye removal in the study sample.
DISCUSSION
Eye removal is an aggressive procedure generally reserved for eyes with malignant tumors, eyes with certain advanced diseases, blind painful eyes that are not well controlled by medication or neurolytic agents, and trauma cases. Indications range from ocular cancer to preventable causes such as trauma or neglected diabetes, where secondary glaucoma may result in a blind painful eye. In some regions, such as Brazil, indications for eye removal may be related to access to health care.
We found ocular melanoma to be the most common indication for eye removal at our center. We observed a nonlinear trend in the total number of eye-removal procedures performed annually at our center over the 13-year study period.
Small-sized and medium-sized melanomas may be treated by plaque radiotherapy, whereas enucleation is frequently performed for large tumors, as well as for small-sized and medium-sized tumors when plaque radiotherapy is unavailable. Because of federal regulations and other factors, plaque radiotherapy is not available to all patients in the public healthcare system in Brazil. Although our center does offer plaque radiotherapy to patients in the public healthcare system, plaques have not been available at our center since 2010 because of funding reallocations. Thus, enucleation is the primary treatment approach for ocular melanoma when plaque radiotherapy is unavailable. This may account for the spike in eye-removal procedures seen from 2011 (n=10) to 2012 (n=81).
Unfortunately, we did not have access to follow-up data to determine how many enucleations resulted following plaque radiotherapy before 2012. This reality has prompted our group to conduct a prospective study treating choroidal melanomas with primary vitrectomy and endoresection. The details of this study are pending publication.
Retinoblastoma was the second most frequent indication for eye removal in our study. Advanced retinoblastoma can be cured in most cases by enucleating the eye, but less advanced cases can be treated with systemic chemotherapy and local modalities such as laser photocoagulation or cryotherapy. Unfortunately, in Brazil, retinoblastoma is often diagnosed when the disease is in an advanced stage, and therefore a large percentage of patients are treated by enucleation11. In a study by Leal-Leal et al., 500 cases of retinoblastoma from 16 centers in Mexico were retrospectively analyzed according to various pathological and demographic criteria12. The authors reported that 84.9% patients were treated by enucleation and concluded that the development of an early detection program and treatment protocol for retinoblastoma was necessary at the national level in Mexico. Although our study did not address enucleation rates in patients with retinoblastoma, previous studies have highlighted that retinoblastoma is generally diagnosed at later stages in developing countries13,14, leading to increased enucleation rates and decreased survival rates15.
In 2012, our center introduced intra-arterial chemotherapy as an effective alternative to enucleation for advanced cases of retinoblastoma16. These cases are not reflected in the number of enucleation procedures reported in this study. Given the use of this new modality, we anticipate a significant reduction in the number of enucleations of eyes with advanced retinoblastoma and thus a significant reduction in the total number of eye-removal procedures at our center.
Ocular melanoma and retinoblastoma were the most common indications for eye removal at our center over the 13-year study period. A Serbian study reviewed 586 cases of patients who underwent enucleation and similarly found that the most common indication was melanoma, followed by retinoblastoma17. Although our study addressed all forms of eye removal, enucleation was the most common procedure performed, and it was the most common procedure used to treat both melanoma and retinoblastoma.
Our results differ from the most recent Brazilian analysis of eye removals at the Araujo Jorge Hospital, a single center 1000 km northwest of São Paulo, by Sirianni et al.18 This was a retrospective review of 269 cases of malignancy in the ocular cavity and indications for eye removal. The authors reported that basal cell carcinoma was the most common malignancy seen, representing 58% of the total cases. In our sample, basal cell carcinoma accounted for two cases (0.5%; not listed in the results because of the low frequency). In the study of Sirianni et al., melanoma accounted for only 6.7% cases, in contrast to 35.4% cases in our study. These differences are most likely accounted for by increased ultraviolet exposure to the north of São Paulo and delay in referral in this relatively underserved region.
Like our study, the study of Sirianni et al. reported that enuclea tion was the most common surgical procedure used to treat retinoblastoma and ocular melanoma, whereas exenteration was used in most cases of squamous cell carcinoma of the conjunctiva and all cases of basal cell carcinoma. The Araujo Jorge Hospital and our facility are not designated trauma centers, which accounts for the absence of trauma as an indication for eye removal in both data sets.
Another study reviewed the clinical causes for ocular enucleation in 1375 cases from a single center in Beijing, China19. The study found that enucleated eyes accounted for 29.5% of all cases sent to the pathology department, which is significantly higher than the 12% we report for all eye-removal procedures at our center. In that study, trauma accounted for 62.5% of all enucleation procedures, followed by tumors at 28.5%. In our sample, trauma accounted for two cases (0.5%; not listed in the results because of the low frequency). Collectively, these differences highlight the importance of evaluating the indications for eye removal in a regional-specific and center-specific manner.
As shown in tables 1 and 3, other indications for eye removal were frequently observed in our study. Evisceration or enucleation was the procedure used to treat all cases for the listed indications, with the exception of invasive squamous cell carcinoma, in which three cases (20% of all squamous cell carcinomas) were treated by exenteration. Endophthalmitis accounted for 6.3% of all indications for eye removal. A previous report found that older age, absence of light perception, endophthalmitis associated with corneal ulcer, and endogenous endophthalmitis were risk factors that were significantly associated with endophthalmitis leading to enucleation or evisceration20. Unfortunately, we were not able to compare patients with endophthalmitis who underwent eye removal with those who did not.
Contrary to the sum of existing literature, ocular melanoma and retinoblastoma accounted for most eye-removal procedures during our 13-year study period. This difference is most likely because of referral patterns in the São Paulo area that limit the number of trauma cases seen in our center, the difficulty in accessing nonsurgical oncological treatment for some of our patients, and the often delayed presentation of patients to the clinic.
Orbital and ocular tumors are best treated at an early stage. The recent introduction of intra-arterial chemotherapy for retinoblastoma at our center, as well as efforts to treat choroidal melanomas with primary vitrectomy and endoresection, may significantly decrease the total number of eye-removal procedures at our center in the coming years, although eye removal will still account for a substantial proportion of surgical procedures.
The rate of enucleation for tumors is high in our series, in contrast to declining trends reported from other parts of the world. The morbidity associated with the procedure can have a significant impact on the patient's self-esteem, workplace productivity, and quality of life, especially when vision loss is unnecessary.

