INTRODUCTION
Postoperative optic opacification of hydrophilic acrylic intraocular lenses (IOLs) has a multifactorial origin, including factors related to IOL manufacturing, patient metabolic and ocular conditions, and surgical techniques and adjuvants used(1). Recently, opacification associated with the presence of gas or air in the anterior chamber has been reported(2-9).
Since 2005, the single-piece hydrophilic acrylic Oft Cryl® IOL (Oft Vision, São Paulo, Brazil) has been largely used in Brazil; however, no case of lens opacification has been reported in the peer-reviewed scientific literature. The purpose of this study was to report data from microscopic analysis of the first case of opacified Oft Cryl® IOL occurring in a patient who presented with gas in the anterior chamber in the early postoperative period of phacoemulsification and posterior vitrectomy with perfluoropropane gas injection.
CASE REPORT
A 51-year-old female patient presented with cataracts in both eyes (OU), and traumatic retinal detachment in the right eye (OD). She had no known associated systemic diseases. In November 2013, she underwent an uneventful posterior vitrectomy with perfluoropropane gas injection, endolaser, phacoemulsification, and Oft Cryl® IOL (Lot 27I13; Serial number 205039031T) implantation in OD at the Altino Ventura Foundation, Recife, Brazil. The patient was non-compliant in terms of head positioning, and on the first postoperative day the gas was filling the anterior chamber, being reabsorbed within a week. On April 2014, the patient underwent an uneventful phacoemulsification in the left eye (OS) by the same surgeon with an Oft Cryl® IOL (Lot 10B14; Serial number 210072454T) implantation. Her postoperative best-corrected visual acuity (BCVA) was 20/100 in OD and 20/20 in OS.
Eight months after OD surgery, the patient returned with decreased vision in OD. Her spectacle-corrected visual acuity (SCVA) was counting fingers at 50 cm in OD and 20/20 in OS. Slit-lamp examination revealed haziness of the IOL in OD and no alterations in OS. The lens in OD was explanted and sent to the Intermountain Ocular Research Center (John A. Moran Eye Center, University of Utah, USA) in the dry state. A hydrophobic acrylic Type 7B (Alcon, Inc., Forth Worth, USA) IOL was implanted in the capsular bag. There were no intraoperative or postoperative complications. The patient's final BCVA in OD was 20/40.
Laboratory analysis
Gross examination was performed and gross pictures were recorded using a digital camera (D40 with a 55 mm lens, Nikon Corp., Tokyo, Japan). The unstained specimen was evaluated and photographed under a light microscope (Olympus Optical Co., Ltd., Tokyo, Japan). The specimen was then rinsed in distilled water, immersed in 1% alizarin red solution (a special stain for calcium) for 20 minutes, rinsed again in distilled water, and reexamined under the light microscope.
Gross laboratorial analyses of the explanted IOL showed a localized round area of whitish discoloration in the central part of the lens optic, within the pupillary and anterior capsulorrhexis margins (Figure 1 A). Light microscopy revealed the presence of granular deposits within the area of gross whitish discoloration, densely distributed in an overall circular pattern (Figure 1 B). The granules were present on the anterior surface and subsurface of the lens, and stained positive for calcium (Figures 1 C and 1 D).
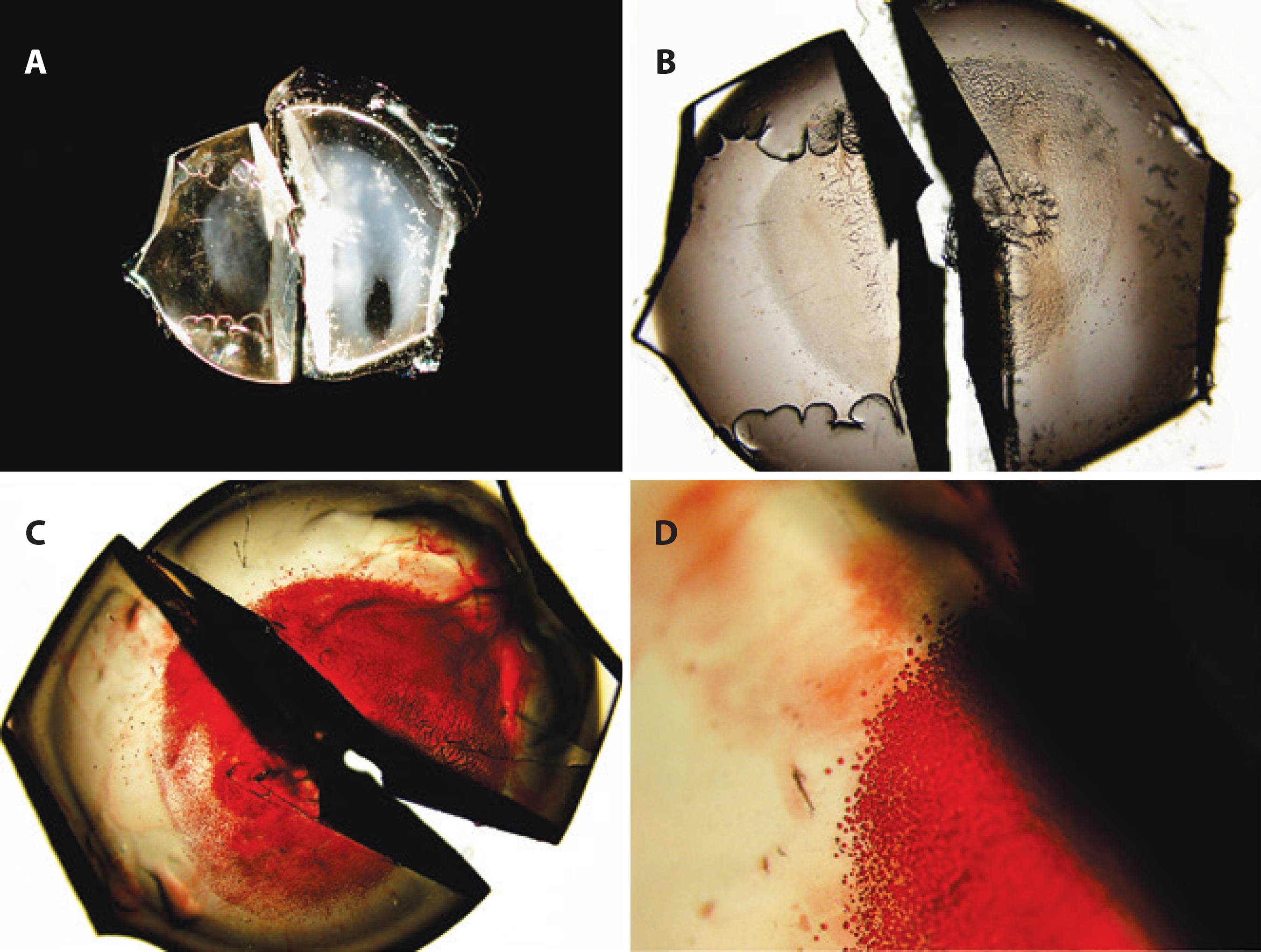
Figure 1 Gross photograph and light photomicrographs of the explanted lens. A) Gross photograph showing central opacification of the lens optic in a round configuration, with a diameter of approximately 4.0 mm. B) Light photomicrograph of the unstained specimen, showing granular deposits in the center of the optic as well as dry viscoelastic material (original magnification, ×20). C and D) Light photomicrographs showing positive (red) staining of the granules after staining with alizarin red (original magnification, ×20 and ×100, respectively).
DISCUSSION
Previous papers have described cases of IOL opacification in hydrophilic acrylic IOLs from different manufacturers(2-11). However, to the best of our knowledge, this is the first peer-reviewed report on Oft Cryl® IOL opacification. Microscopic analysis of the opacified lens revealed calcium granular deposits on the surface and subsurface of the lens.
Similarly to the pattern seen in the Oft Cryl® IOL, calcification within the pupillary and anterior capsulorrhexis margins has been described in eyes in which gas or air 1) was injected intracamerally to treat Descemet's membrane detachment, to aid in graft adherence in endothelial transplants; 2) was injected to treat hypotony following trabeculoplasty; or 3) went into the anterior chamber after injection in the vitreous cavity to treat retinal detachment and ocular hypotony(2-8). In these lenses, calcium granules were also found on the surface and subsurface of the IOLs.
Werner et al.(2) proposed three possible explanations for IOL calcification after procedures involving intracameral air or gas: 1) direct contact between the IOL surface and the exogenous gas/substance; 2) intracameral metabolic change because of the presence of an exogenous gas/substance; and 3) exacerbated inflammatory reaction after multiple surgical procedures. The formation of calcium deposits appears to depend both on the material of the IOL and on the local chemical microenvironment of the aqueous humor(12). The Oft Cryl® IOL is composed of a poly-hydroxyethylmethacrylate copolymer. The first two hypotheses can possibly explain the etiology of the Oft Cryl® IOL opacification observed in the present case because the characteristically round area of whitish discoloration on the center of the IOL optic suggests that the presence of the gas in the early postoperative period was a determining trigger of calcium deposition. Furthermore, our patient had no associated systemic disease, intraoperative complication, or significant or persistent postoperative inflammation that could justify IOL calcification. In addition, the Oft Cryl® IOL implanted in OS did not opacify throughout the follow-up period.
Since 2012, approximately 26,300 Oft Cryl® IOLs have been implanted at Altino Ventura Foundation in eyes with no co-morbidities, eyes undergoing combined phacoemulsification and vitrectomy, and eyes subject to combined phacoemulsification and trabeculectomy or endothelial transplants. This was our first case of opacification. Thus, this IOL should not be discredited based on the current report, which supports the hypothesis that intracameral gas can act as a trigger of hydrophilic lens calcification(2-9). Together with previous articles(2-9), the present report suggests that hydrophilic IOLs should be avoided in eyes that require procedures associated with intracameral presence of air or gas.
In conclusion, microscopic analysis of the opacified Oft Cryl® IOL showed calcium deposits on the anterior surface/subsurface of the lens optic, restricted to the pupillary and anterior capsulorrhexis margins. This suggests that opacification was triggered by intracameral gas in contact with the IOL in the early postoperative period.

