INTRODUCTION
Drug reaction with eosinophilic and systemic symptoms (DRESS) syndrome is an adverse drug reaction characterized by generalized skin rash, enlarged lymph nodes, and fever. Laboratory testing typically demonstrates eosinophilia, atypical lymphocytes, and multiple organ injury(1-5). The incidence of DRESS syndrome is reportedly 1 in 1,000-10,000 prescriptions of each causal drug, and symptoms may appear within 8 weeks after the first use(2-6). Herein, we report two cases of DRESS syndrome in patients who developed during ocular treatment.
Case 1
A 65-year-old man presented with pain, redness, tearing, and decreased vision in his left eye (OS) for 10 days and fever for 1 day. His medical history included hypertension, diabetes, and dyslipidemia. The patient had undergone phacoemulsification with intraocular lens implantation complicated with posterior capsule rupture in OS 2 months prior to this evaluation. His best corrected visual acuity (VA) was 20/25 in the right eye (OD) and light perception in OS. Anterior biomicroscopy was normal in OD. Conjunctival hyperemia 3+/4, a corneal ulcer with stromal infiltrate, hypopyon, and vitritis 4+/4 were observed in OS. Fundoscopy was normal in OD and impossible in OS. The patient was hospitalized, and empirical intravenous (IV) cephalothin, topical moxifloxacin 0.5%, and atropine 1% in OS were initiated. Further, intravitreal injection of vancomycin and ceftazidime was performed in OS. Corneal scrap cultures were positive for Enterobacter aerogenes sensitive to carbapenems. IV meropenem was added to the antibiotic regimen, and the patient improved after 4 days of treatment.
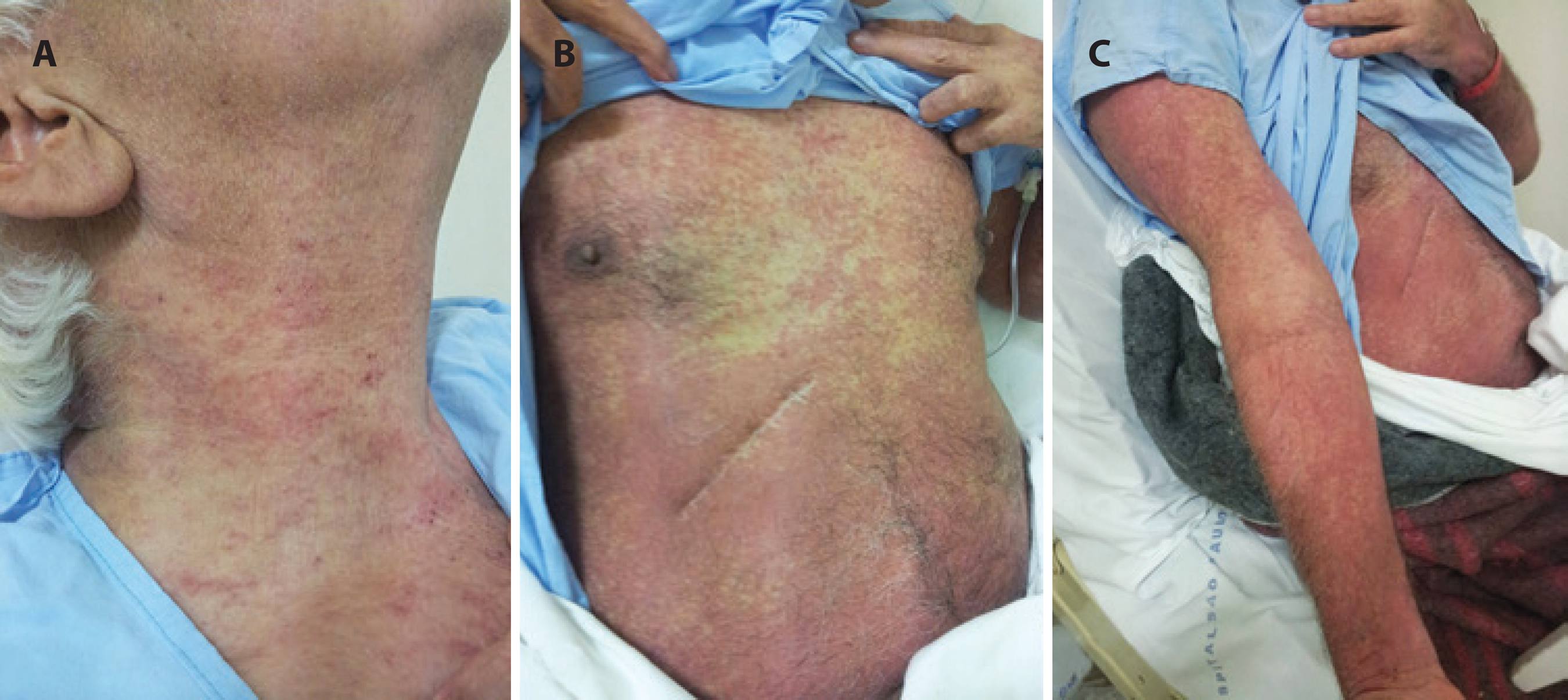
During hospitalization, he developed severe systemic hypertension and eosinophilia (1,417 eosinophils per microliter of blood; 15.5% leukocytes) and a macular rash involving the neck, chest, abdomen, and arms (Figure 1). Skin biopsy demonstrated urticarial dermatitis. Despite treatment, the skin lesions worsened, and the patient developed fever, tachypnea, tachycardia, hypotension, generalized tremors, and disorientation. Laboratory testing demonstrated leukopenia, elevated hepatic enzymes, and hyponatremia. He was first diagnosed as having bacterial sepsis. Treatment was expanded with IV polymyxin B and vancomycin. However, fever and hypotension persisted with worsening of skin lesions, reduced urinary output, increased serum creatinine levels, and eosinophilia. Blood and urine cultures were negative. DRESS syndrome was diagnosed, and the patient i.v. prednisone 1 mg/kg/day was initiated. After 4 days in the intensive care unit (ICU), the patient was hemodynamically stabilized with clinical improvement. VA in OS remained light perception due to the complications of serious endophthalmitis.
Case 2
A 54-year-old woman complained of low VA in OS for 2 days associated with sudden onset of ocular pain and a paracentral dark spot affecting the visual field in OD. The patient had myalgia, fever, and lymphadenopathy. Medical, family, and ocular histories were unremarkable. VA was 20/20 in OD and 20/400 in OS. Anterior biomicroscopy and intraocular pressures were normal in both eyes. Fundoscopy of OD was normal and OS demonstrated vitritis 2+/4+ and a yellowish exudative plaque at the posterior pole affecting the fovea. Serology test was positive for toxoplasmosis IgM only. Treatment was initiated with topical prednisolone acetate 1%, topical tropicamide 1%, systemic pyrimethamine 50 mg/day, sulfadiazine 4 mg/day, folinic acid 5 mg/day, and oral prednisone 1 mg/kg/day. Symptoms and ocular signs improved with treatment.
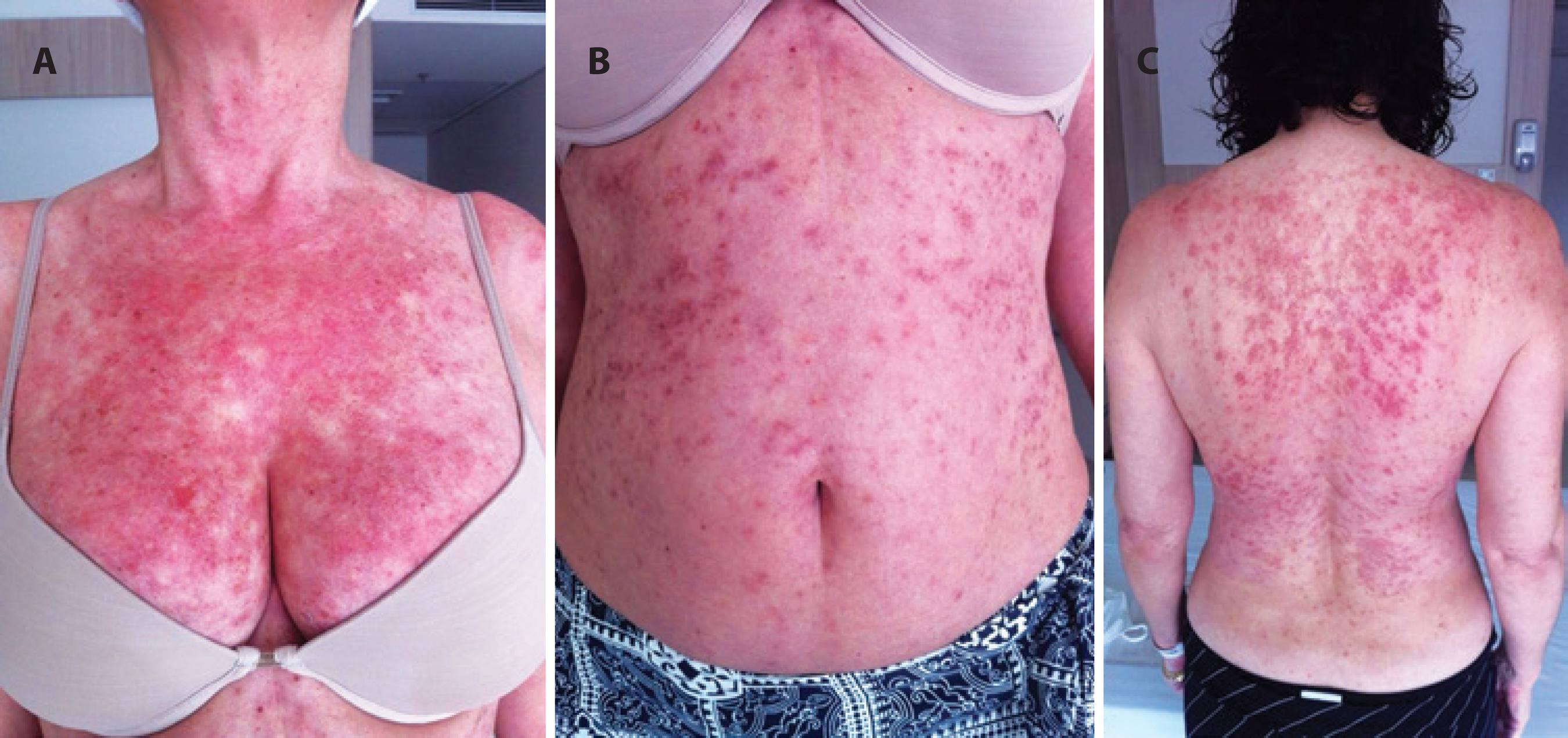
After 1 month, the patient developed a macular morbilliform rash affecting the chest, abdomen, and back (Figure 2). She also developed eosinophilia and persistent lymphadenopathy. DRESS syndrome was diagnosed, and the patient was admitted to ICU and treated with oral pyrimethamine, folinic acid, azithromycin, and i.v. prednisolone 1 mg/kg/day. The patient was discharged after improvement in systemic symptoms with a VA of 20/50 in OS due to a chorioretinitis scar adjacent to the fovea.
DISCUSSION
DRESS syndrome is a severe drug reaction that typically develops between 2 and 8 weeks after drug exposure with symptoms persisting for longer than 2 weeks(2-4). Diagnostic criteria include widespread rash, fever, and laboratory abnormalities (eosinophilia >1,500/mm3 or atypical lymphocytes)(1-7). Systemic involvement affecting the liver (50%), kidneys (10%), lungs (10%), heart, pancreas, and others may also be observed with laboratory testing revealing specific organ damage(2-4). Histological examinations of skin biopsy are nonspecific, for DRESS syndrome but may be important in ruling out other etiologies(4). Differential diagnoses of DRESS syndrome include infections, Stevens Johnson syndrome, connective tissue diseases, and hematological diseases(2,6,8).
Several drugs have been reported to cause DRESS syndrome, including allopurinol, anticonvulsants (phenobarbital, carbamazepine, phenytoin, lamotrigine, and sodium valproate), vancomycin, minocycline, trimethoprime-sulfamethoxazole, pyrimethamine-sulfadiazine, proton pump inhibitors, azathioprine, and hydroxychloroquine, among others(2-5). Amoxicillin has been variously described either as a cause or as an aggravating factor of DRESS syndrome(2). In our first case, DRESS syndrome may have been triggered by i.v. cephatotin, i.v. meropenem, or intravitreal injection of vancomicin or ceftazidime. As vancomycin is one of the medications most commonly associated with DRESS syndrome, it is possible that DRESS syndrome was triggered by intravitreal injection of this drug. To our knowledge, there are no previously reported cases of DRESS syndrome associated with intravitreous injection of antibiotics. In our second case, the association between DRESS syndrome and sulfadiazine was more evident and easier to identify. The pathogenesis of DRESS syndrome has yet to be elucidated; however, a number of authors have reported associations with specific HLA groups and herpes virus reactivation(2-5,8).
As prospective randomized trials for DRESS syndrome treatment have yet to be reported, data regarding the management of DRESS syndrome have exclusively been provided by case and series reports. Ideally, patients with DRESS syndrome are treated in ICU, causal drugs must be discontinued, and systemic involvement should be treated specifically(2,9). The majority of authors recommend systemic glucocorticoid administration (1 mg/kg/d) until the disease is controlled before slowly tapering the dose(2,9). Cutaneous rash may persist for weeks and return if corticosteroids are quickly discontinued or if there is new exposure to the causative drug. The prognosis of DRESS syndrome is associated with early recognition and discontinuation of the offending drug. Due to the severity and multiplicity of systemic involvement, DRESS syndrome has a high morbidity and mortality reaching 10%-40%(2,3,9). The patient must be informed of the lifetime contraindication to the use of the causal drug and increased risk of developing autoimmune diseases (thyroiditis, adrenal insufficiency, diabetes insipidus, connective tissue disease, or a reaction resembling graft-versus-host disease)(2,10).
DRESS syndrome is a rare but potentially fatal complication related to an adverse reaction to one of several potentially causative medications. Many of these pharmacological agents are routinely used in ophthalmic practice, such as trimethoprim-sulfamethoxazole and vancomycin. Herein, we report two cases of DRESS syndrome associated with ocular treatment. Thus, ophthalmologists should be aware of DRESS syndrome and be able to recognize the initial signs of this condition. Treatment of DRESS syndrome requires hospitalization and intensive care follow-up.

