INTRODUCTION
Technological advances and improved staff training in neonatal care units are responsible for the increase in the survival of low-weight premature infants(1,2). However, premature children who survive may have motor and sensory losses at many levels.
Retinal immaturity can interfere with visual development during some child growth stages, making these infants susceptible to retinopathy, refractive variation and amblyopia, strabismus, and low vision(3-6).
Retinopathy of prematurity (ROP) is a vasoproliferative retinal disease with a multifactorial etiology that affects premature infants as a result of their immaturity and other risk factors(7). It is considered a major cause of preventable childhood blindness(8-11), and its incidence can be affected by the availability and accessibility of screening services(12).
The International Classification of Retinopathy of Prematurity is based on the extent (recorded as hours of the clock, from 1 to 12, or 30° segments), location (zones I-III), and staging (ROP 1-5) of the disease(13,14). Aggressive posterior ROP is a severe form of the disease that is associated with rapid progression. The vascular changes observed in the vessels of the posterior pole develop quickly and bleeding at the edge of the vascularized and non-vascularized retina can occur.
According to Chadha and Subramanian(15), vision is a highly complex function and is influenced by various clinical and non-clinical factors associated with visual function, such as contrast sensitivity, scanning speed, and visual field. Evaluation of quality of life in visually impaired children should take these factors into consideration as well as the effect of other factors such as the socioeconomic status of the family, access to educational support, and relationships with family members and other people. These measures may not be evaluated in all children attending low vision pediatric services.
The prematurity of a child can cause exceptional experiences and for parents, including unexpected situations and feelings of despair(16). Prematurity can lead to many challenging health situations, which can evolve with episodes of progress and setbacks that cause psychological consequences for the parents and the child; in addition, this can affect the professional lives of the parents and the socio-emotional status of the family(17).
When communicating the various diagnoses associated with prematurity situations, the clinicians should consider the effect on parent/child bonding(18). From birth, families of premature children face moments of struggle while trying to understand the diagnosis, treatment, and sequelae of prematurity. Deficits in these children are observed and diagnosed over the years due to day-to-day living and medical management. There are often difficulties related to the acceptance of these impairments and mobilization of resources to deal with them(19).
Parents can have reactions of shock, despair, and/or sadness(16,18,20), because they are often unaware of what prematurity entails and may have misconceptions about these births(16). The purpose of this study was to evaluate the effect of ROP on vision-related quality of life in children.
METHODS
This prospective observational cross-sectional study was conducted from July 2010 to April 2012 at the Department of Ophthalmology and Visual Sciences in the Low Vision and Visual Rehabilitation Sector of the Early Visual Stimulation Clinic. The study was approved by the Research Ethics Committee of the Federal University of São Paulo under number 0374/10 and followed the principles of the Helsinki Declaration and Resolution 196/96. Participants were informed of the aims and procedures of the study and they agreed to participate through signing of the Informed Consent form.
The Children's Visual Function Questionnaire (CVFQ) was used. The CVFQ is a validated and specific instrument that is completed by parents/caregivers and is designed to measure vision-related quality of life in children up to 7 years of age. A version for children under 3 years of age was used in this study; it contains 35 questions on topics related to the quality of the child’s visual function and is divided into 6 subscales(21,22): General Health (questions about the general health conditions of the child); Vision Health (or General Vision, questions about the child’s visual health); Competence (questions about the child’s ability to perform daily activities); Personality (questions about the effect of visual impairment on the child’s social behavior and personality); Family Impact (questions about the effect of visual problems on the parents and family and their concerns); and Treatment (questions about the effect of treatment for visual impairment on the child and family).
The subscale scores ranged from 0 (worst score) to 1 (best score). The score for each subscale was determined from the mean score of the responses to the subscale questions. The score for the Total Index was determined from the mean scores of the subscales. Responses classified as "not applicable" and unanswered items were omitted from the mean scores.
The questionnaires were administered by the researcher and completed by the parents during a 20-30-min private interview. The sample consisted of parents/caregivers of premature infants up to 3 years of age who had been diagnosed with ROP (with or without treatment) and did not have any neurological sequelae and/or other associated diseases (ROP group). The control group comprised parents/caregivers of premature children up to 3 years of age who did not have visual problems or any neurological sequelae and/or other associated diseases.
Parents/caregivers of children with the following neurological sequelae were excluded from the study: chronic encephalopathy, hydrocephalus, microcephaly, macrocephaly, central nervous system malformation, and intracranial hemorrhage at the time of the study. Prematurity data, including ROP diagnosis, previous treatments, and neurological sequelae, were obtained from the child’s medical records. Data regarding hospital discharge, birth summary, and medical referrals were obtained from the reports provided by the parents/caregivers. ROP diagnosis was obtained from the examination of the child either during hospitalization or from subsequent eye examinations.
Children with a gestational age (the duration from the last period of the woman to birth, measured in weeks or days) of less than 37 weeks were considered premature. Prior treatment included laser therapy or conventional surgery.
The SPSS program was used for sample description calculation (mean, median, standard deviation, minimum and maximum values, frequency, and proportions) and for statistical analysis of the CVFQ. The unpaired Student’s t-test was used for comparison of the mean quality of life scores. The significance level was set at 5% (p<0.05).
We used a multiple linear regression model based on the Total Index of quality of life to study the effect of the groups (ROP and control) and of other variables (parental education, gestational age, child’s age, and weight at birth) on children’s quality of life.
RESULTS
The study included a total of 88 individuals: 43 in the ROP group and 45 in the control group.
With regard to the distribution of children by gender in the groups, there were more girls in the ROP group (53%) and more boys in the control group (56%). Regarding age, the children were approximately 9 months of age on average in the ROP group and 1 year of age in the control group. This difference was statistically significant (p=0.019, Student’s t-test).
Considering birth weight, the majority of children in the ROP group weighed ≤1500 g (88.4%). The control group had a higher percentage of children with birth weights between 1000 g and 2000 g (64.5%). Two subjects for whom weight information was missing were excluded from statistical calculations. Dividing the sample according to the gestational age, most of the total sample (38.6%) and most of the ROP group (48.8%) was characterized in the age group of 26-29 weeks. In the control group, most of the children were in the age group of 34-36 weeks (48.9%) (Table 1).
Table 1 Sample description about child age, birth weight and gestational age
| N | Mean | Median | SD | Min-max | ||
|---|---|---|---|---|---|---|
| Child age (months) | ROP | 43 | 8.9 | 7.0 | 7.3 | 1-33 |
| Control | 45 | 12.7 | 14.0 | 7.7 | 1-25 | |
| Total | 88 | 10.9 | 8.0 | 7.7 | 1-33 | |
| Birth weight (grams) | ROP | 43 | 1050.7 | 950.0 | 380.0 | 505-2450 |
| Control | 43 | 1495.7 | 1480.0 | 606.8 | 625-3500 | |
| Total | 86 | 1273.2 | 1215.0 | 550.8 | 505-3500 | |
| Gestational age (weeks) | ROP | 43 | 27.7 | 28.0 | 2.6 | 23-33 |
| Control | 45 | 30.7 | 31.0 | 3.4 | 22-36 | |
| Total | 88 | 29.2 | 29.0 | 3.4 | 22-36 |
N= number; Min-max= mínimum and maximum; SD= standard deviation.
The majority of parents/caregivers in the total sample were women (94%), and were parents (98.9%); only 1 subject in the control group had a different relationship with the child (grandmother). In the ROP group, most of the participants were in the age range of 21-30 years (48.8%); in the control group, most were in the age range of 31-40 years (46.7%). Only 18.1% of the total sample was over the age of 41 years or under 21 years. More than half of the sample had some high school levels of schooling (51.2%). Regarding marital status, there was a predominance of married participants (Table 2).
Table 2 Sample description about parents and caregivers age, marital status and education
| ROP | Control | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||||
| Parents/caregivers age | Below 21 years | 5 | 11.6 | 6 | 13.3 | 11 | 12.5 | ||
| 21-30 years | 21 | 48.8 | 14 | 31.1 | 35 | 39.8 | |||
| 31-40 years | 16 | 37.2 | 21 | 46.7 | 37 | 42.0 | |||
| 41-50 years | 1 | 2.3 | 3 | 6.7 | 4 | 4.5 | |||
| Above 50 years | 0 | 0.0 | 1 | 2.2 | 1 | 1.1 | |||
| Total | 43 | 100.0 | 45 | 100.0 | 88 | 100.0 | |||
| Parent marital status | Single | 10 | 23.3 | 5 | 11.1 | 15 | 17.0 | ||
| Married | 31 | 72.1 | 38 | 84.4 | 69 | 078.4 | |||
| Divorced | 1 | 2.3 | 1 | 2.2 | 2 | 2.3 | |||
| Widower | 1 | 2.3 | 1 | 2.2 | 2 | 2.3 | |||
| Total | 43 | 100.0 | 45 | 100.0 | 88 | 100.0 | |||
| Parents education | Unconclued school | 4 | 9.3 | 4 | 8.9 | 8 | 9.1 | ||
| Concluded school | 6 | 14.0 | 1 | 2.2 | 7 | 8.0 | |||
| Unconcluded high school | 6 | 14.0 | 7 | 15.6 | 13 | 14.8 | |||
| Concluded high school | 18 | 41.9 | 14 | 31.1 | 32 | 36.4 | |||
| Incomplete university | 6 | 14.0 | 5 | 11.1 | 11 | 12.5 | |||
| Complete university | 3 | 7.0 | 8 | 17.8 | 11 | 12.5 | |||
| Post-graduation | 0 | 0.0 | 6 | 13.3 | 6 | 6.8 | |||
| Total | 43 | 100.0 | 45 | 100.0 | 88 | 100.0 | |||
N= number.
With regard to the stage of ROP, most children in the ROP group had stage 3 ROP (32.6%), followed by stage 5 ROP (25.6%) and stage 1 ROP (14%). Stage 2 ROP, stage 4 ROP, and aggressive posterior ROP were observed in similar numbers of patients (4 children each).
The mean Total Index score and the mean General Health, General Vision, Competence, Personality, and Family Impact subscale scores were lower in the ROP group than in the control group. Vision-related quality of life in the ROP group was significantly lower than that in the control group in terms of the Total Index score (p<0.001) and the CVFQ subscale scores: General Health (p=0.006), Vision Health (p<0.001), Competence (p<0.001), Personality (p<0.001), and Family Impact (p<0.001) (Figure 1). The Treatment subscale was not statistically analyzed because only 5 individuals in the ROP group were undergoing treatment. As a result of the inclusion criteria, this subscale was not applicable to the control group.
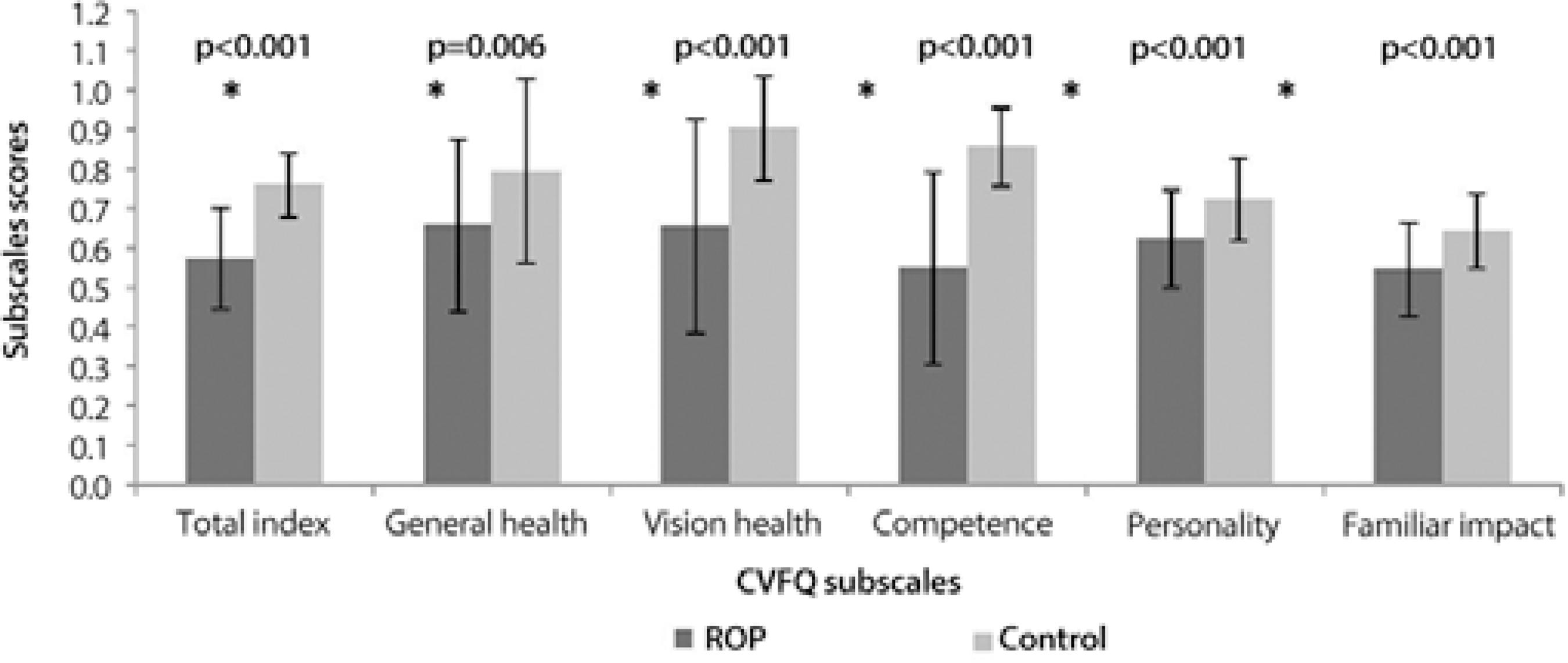
Figure 1 Comparison of quality of life between the ROP and control groups in terms of the Total Index and CVFQ subscale scores (mean and standard deviation).
Vision-related quality of life was analyzed according to the disease stage, and the ROP group was divided into 2 categories: stage 1, 2, and 3 ROP (24 participants) and stage 4 and 5 and aggressive posterior ROP (19 participants).
The mean Total Index score as well as the mean CVFQ subscale scores were lower in the stage 4 and 5 and aggressive posterior ROP group than in the stage 1, 2, and 3 ROP group. The Total Index score (p=0.006) as well as the Vision Health (p=0.001), Competence (p=0.045), and Family Impact (p=0.052) subscale scores in the stage 4 and 5 and aggressive posterior ROP group were significantly lower than those in the stage 1, 2, and 3 ROP group (Figure 2). As a result of the low number of subjects for comparison (4 in the stage 1, 2, and 3 ROP group and 1 in the stage 4 and 5 and aggressive posterior ROP group), the Treatment subscale was not analyzed.
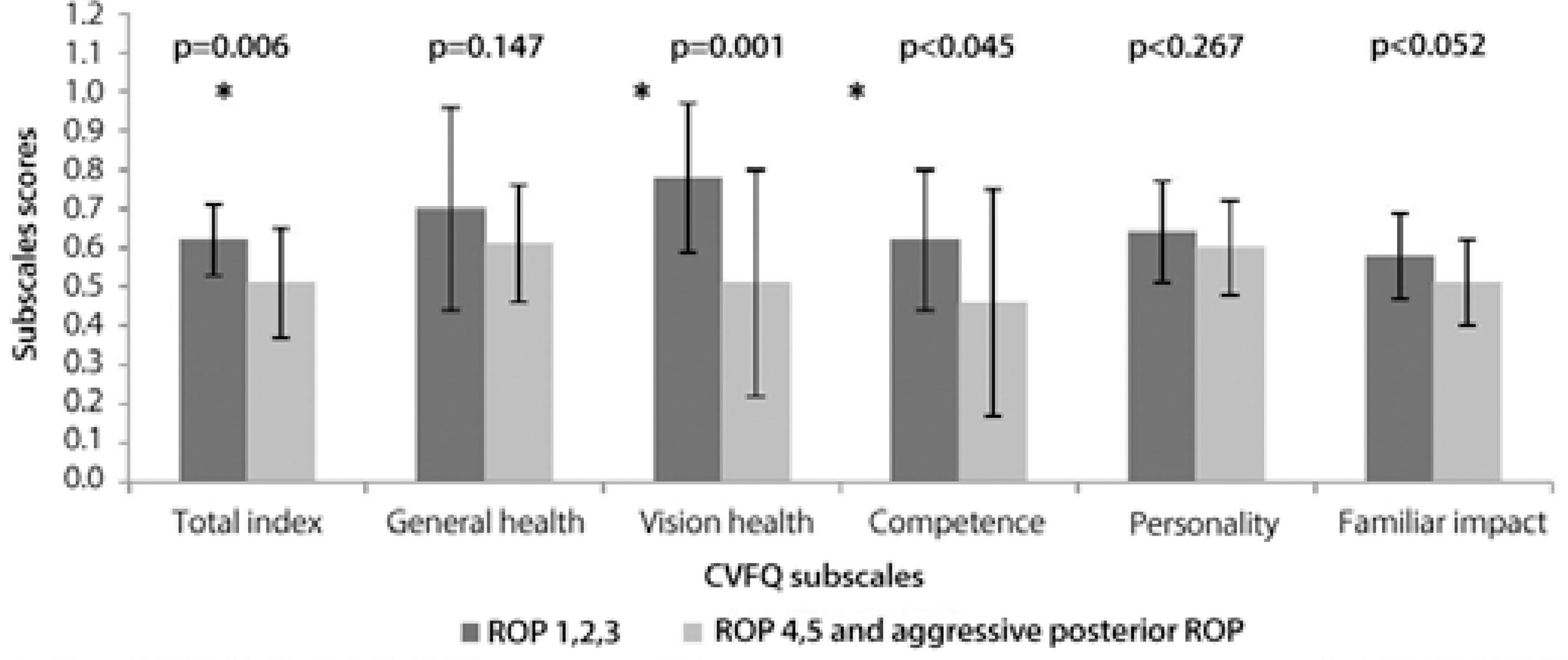
Figure 2 Comparison of quality of life between the groups of ROP severity in terms of the Total Index and CVFQ subscale scores (mean and standard deviation).
The means of the descriptive variables were different between the ROP and control groups. These differences were statistically analyzed using the multiple linear regression model in order to evaluate the effect of these variables on the Total Index of quality of life measured by the CVFQ.
To compare the groups, the mean of each variable was considered. For each categorical variable that contained a low number of individuals, the data was reorganized into 2 categories: parent’s/caregiver’s age (≤30 years/>30 years), marital status (single or unmarried/married or with partner), education (high school/higher education), and gestational age (<30 weeks/≥30 weeks). The numerical variables of child’s age, birth weight, and gestational age were also considered in the comparison between the groups.
The variables that showed significant differences between the groups were included in the multiple linear regression model: parental education (p=0.032), gestational age as a categorical and numerical variable (p<0.001), child’s age (p=0.019), and birth weight (p<0.001).
The multiple linear regression model was used to study the effect of the groups (ROP and control) and of other variables on quality of life. Although the birth weight variable was associated with the group, it was not included in the multiple linear regression model because of its high correlation with gestational age (0.815), a variable that was included in the model (Table 3).
Table 3 Estimates of multiple linear regression model adjusted (coefficient, standard error and p) of quality of life
| Model | Coefficient | Standard error | p |
|---|---|---|---|
| Constant | 0.313 | 0.052 | <0.001 |
| Parental education | 0.075 | 0.025 | 0.003 |
| Gestational age | -0.013 | 0.024 | 0.593 |
| Child's age | 0.002 | 0.001 | 0.145 |
| Multiple pregnancy | 0.037 | 0.026 | 0.158 |
| Group | 0.160 | 0.026 | <0.001 |
According to the estimates presented in table 3, the Total Index scores in the ROP group were significantly lower than those in the control group even after controlling for variables (p<0.001). The group variable was included in the regression, i.e., the occurrence of ROP impacts on quality of life, corroborating the results obtained in the statistical analysis when comparing the means between groups.
Another variable that had a significant effect on the Total Index score was the educational level of the parents (p=0.003); higher parental education was associated with a higher quality of life.
DISCUSSION
The results obtained from the CVFQ revealed a negative effect of ROP on vision-related quality of life in the ROP group compared with the control group in all subscales and in the Total Index score. Comparisons in terms of the disease stage showed a greater decrease in quality of life in children with more severe ROP.
The results of the General Health and Vision Health subscales indicated that visual problems affect children’s quality of life not only in terms of visual issues but also in terms of the general health status of the children with ROP.
The difficulties of children with visual problems, such as ROP, were identified through the Competence subscale results and were related to the performance of daily activities, such as eating alone, tracking movements, washing the face, and walking and jumping. Parents of younger children chose the answer "does not apply to my child" for the questions about walking and climbing stairs and brushing teeth because of the age of the children and/or not having observed such behaviors in their babies at the time of the questionnaire.
The same response was selected in the Personality subscale for questions about reading books, watching TV, playing video games, and playing with other children because they were inapplicable for parents of younger children or those who had not observed the activity in their children.
The difference between the groups in the Family Impact subscale highlighted the parents’ concerns and problems in dealing with children with visual problems and the social consequences of this condition. In this subscale, parents who had not observed these behaviors such as "my child feels different from other children" or "my child is teased because of his/her vision problems" opted for the answer "does not apply to my child."
Only 5 children in the ROP group (11.6%) were undergoing treatment. Because of the low representation of children receiving treatments, such as occlusion therapy, glasses, or eye drops and other medications, this subscale was excluded from statistical analysis. The diagnosis of ROP and the beginning of eye examinations at the time of the questionnaire may have contributed to the low number of answers regarding this topic.
Eye diseases can cause affect the quality of life of children and family members and result in losses in skill acquisition and global psychomotor development, as reported previously(22-24).
The lower quality of life scores obtained by the group with more severe ROP were similar to the results reported by Birch et al.(23), who found higher scores in the Competence, Personality and Family Impact subscales for the group of children with the worst eyesight.
When investigating the variables influencing quality of life, the effect of parental education on the Total Index score was confirmed, with higher education levels corresponding to better quality of life. This data can be justified by the fact that parents with more education may have better understanding of the medical information. Consequently, the bond between the physician and the family may be constructed and strengthened because of greater confidence. Previous studies have highlighted the problems of communication between patients’ families and health professionals as a result of the use of technical language(19,24-28).
According to Holditch-Davis et al.(29), the stress experienced by mothers when confronted by child prematurity can be aggravated by low education levels and socioeconomic status.
Lopes et al.(22), who used the CVFQ to assess vision-related quality of life in children with cataract, included a control group of children born at term. In the present study, the control group comprised children without visual problems or neurological disorders and related diseases who were born prematurely. The highest mean score for the control group was obtained in the Vision Health subscale (0.90), supporting the data by Lopes et al.(22). Other CVFQ subscales had lower values than 0.90 in the control group, which may indicate that premature birth had an effect on quality of life. Despite having higher means than the ROP group, the control group had low scores in the Family Impact and Personality subscales (values less than 0.75); this may explain the effect of prematurity on the family and on the personality development of the child.
CONCLUSION
ROP has a negative effect on vision-related quality of life in children, as shown by the use of the CVFQ. Quality of life worsened with severe ROP, whereas it improved with higher parental education levels.
Premature birth is associated with multiple sequelae and comorbidities, and vision may not be the only cause of low scores in the quality of life questionnaire related to health.
Knowledge of the quality of life of premature children is necessary for the medical community and society as a whole, because such children may require prolonged and expensive care, both during and after the neonatal period. Such information can help with the allocation of resources, provision of parental guidance, and medical decisions(30).
Given the stress to which they are subjected, families of ROP children are at risk for psychological problems and familial bonding disorders. They need support to organize their daily lives and face the challenges resulting from the issues caused by eye diseases and to better care for their children with low vision.
The data obtained will enable an increase in services and health professionals directly linked to the assistance of these families, helping them in the adaptation process. The quality of life questionnaire used in this study can help in evaluating the services, demonstrating its effectiveness.

