Arq. Bras. Oftalmol. 2009; 72 (5): 10.1590/S0004-27492009000500008
Total: 1435
Jefferson Augusto Santana Ribeiro1; André Messias2; Ingrid U. Scott3; Rodrigo Jorge4
DOI: 10.1590/S0004-27492009000500008
ABSTRACT
PURPOSE: To describe an intravitreal injection technique using a commercially available 29-gauge insulin needle syringe (29GN syringe) and a 21-gauge (G) needle, comparing compound waste associated with this technique application and the one described in ranibizumab (Lucentis®) kit instructions. METHODS: Ten 0.3 ml doses of distilled water were aspirated using the 29GN syringe and 21G needle (PT technique), and another ten equal doses were aspirated employing the sterilized Lucentis® kit (LK technique), which contains a 1ml tuberculin syringe, a 18G needle for compound aspiration and a 30G needle for intravitreal injection. For aspiration using the PT technique, a 21G needle is attached over a 29GN syringe. After compound aspiration, the 21G needle is removed and intravitreal injection is performed using the 29G needle. Using a precision balance, the aspiration needles (21G for PT; 18G for LK) were weighed before and after water aspiration and the syringe-needle complexes for injection (29GN for PT; 30G for LK) were weighed before aspiration and after emptying them. The volumes left in the aspiration needles and needle-syringe complexes were estimated by the difference in weight in grams, which were converted to millilitres. RESULTS: The mean (±SD) residual volume (ml) of aspiration needles (21G for PT; 18G for LK) was significantly lower with PT technique (0.0034 ± 0.0016) when compared to LK tech nique (0.0579 ± 0.0011) (p<0.01). The mean (±SD) residual volume (ml) of syringe-needle complexes was significantly lower with PT technique (0.0056 ± 0.0011) than with LK (0.0906 ± 0.003 ml) (p<0.01). CONCLUSION: The proposed technique is a reasonable alternative for minimizing medication loss during intravitreal injection procedures.
Keywords: Angiogenesis inhibitors; Injections; Retinal diseases; Ophthalmologic surgical procedures; Macular degeneration; Drug administration routes; Vitreous body
RESUMO
OBJETIVO: Descrever técnica de injeção intravítrea utilizando agulha-seringa de 29 gauge (seringa 29GN) e agulha 21 gauge (G) comercialmente disponíveis, comparando perda de composto associada à aplicação desta técnica com a descrita nas instruções do kit do ranibizumabe (Lucentis®). MÉTODOS: Dez doses de 0,3 ml de água destilada foram aspiradas com a seringa 29GN e a agulha 21G (técnica PT) e outras dez doses iguais foram aspiradas utilizando-se o kit do Lucentis® (técnica LK). Para aspiração com a técnica PT, a agulha 21G é colocada sobre a seringa 29GN. Depois da aspiração, a agulha 21G é removida e a injeção intravítrea é realizada com a agulha 29G. A técnica LK utiliza seringa de tuberculina de 1 ml acoplada a agulha 18G para aspiração e agulha 30G para injeção intravítrea. Usando balança de precisão, as agulhas de aspiração (21G para PT; 18G para LK) foram pesadas antes e depois da aspiração da água e os complexos agulha-seringa para injeção (29GN para PT; 30G para LK) foram pesados antes da aspiração e após serem esvaziados. Os volumes restantes nas agulhas de aspiração e complexos agulha-seringa foram estimados pela diferença dos pesos em gramas com conversão para mililitros. RESULTADOS: O volume (ml) residual médio (±DP) das agulhas de aspiração (21G para PT; 18G para LK) foi significativamente menor com a técnica PT (0,0034 ± 0,0016) quando comparado à técnica LK (0,0579 ± 0,0011) (p<0,01). O volume (ml) residual médio (±DP) dos complexos agulha-seringa foi significativamente menor com a técnica PT (0,0056 ± 0,0011) do que LK (0,0906 ± 0,003 ml) (p<0,01). CONCLUSÃO: A técnica de injeção proposta é uma alternativa razoável para minimizar perda de medicação durante aplicação de injeções intravítreas.
Descritores: Inibidores da angiogênese; Injeções; Doenças retinianas; Procedimentos cirúrgicos oftalmológicos; Degeneração macular; Vias de administração de medicamentos; Corpo vítreo
ORIGINAL ARTICLE
Alternative technique for reducing compound waste during intravitreal injections
Técnica alternativa para reduzir a perda de medicação durante injeção intravítrea
Jefferson Augusto Santana RibeiroI; André MessiasII; Ingrid U. ScottIII; Rodrigo JorgeIV
IAssistant physician, Department of Ophthalmology, Ribeirão Preto School of Medicine - University of São Paulo - USP - Ribeirão Preto (SP) - Brazil
IIProfessor of Ophthalmology, Department of Ophthalmology of USP - Ribeirão Preto (SP) - Brazil
IIIAssistant Professor, Departments of Ophthalmology and Public Health Sciences, Penn State College of Medicine - Hershey (PA) - USA
IVAssistant Professor, Department of Ophthalmology of USP - Ribeirão Preto (SP) - Brazil
RESUMO
PURPOSE: To describe an intravitreal injection technique using a commercially available 29-gauge insulin needle syringe (29GN syringe) and a 21-gauge (G) needle, comparing compound waste associated with this technique application and the one described in ranibizumab (Lucentis®) kit instructions.
METHODS: Ten 0.3 ml doses of distilled water were aspirated using the 29GN syringe and 21G needle (PT technique), and another ten equal doses were aspirated employing the sterilized Lucentis® kit (LK technique), which contains a 1ml tuberculin syringe, a 18G needle for compound aspiration and a 30G needle for intravitreal injection. For aspiration using the PT technique, a 21G needle is attached over a 29GN syringe. After compound aspiration, the 21G needle is removed and intravitreal injection is performed using the 29G needle. Using a precision balance, the aspiration needles (21G for PT; 18G for LK) were weighed before and after water aspiration and the syringe-needle complexes for injection (29GN for PT; 30G for LK) were weighed before aspiration and after emptying them. The volumes left in the aspiration needles and needle-syringe complexes were estimated by the difference in weight in grams, which were converted to millilitres.
RESULTS: The mean (±SD) residual volume (ml) of aspiration needles (21G for PT; 18G for LK) was significantly lower with PT technique (0.0034 ± 0.0016) when compared to LK tech nique (0.0579 ± 0.0011) (p<0.01). The mean (±SD) residual volume (ml) of syringe-needle complexes was significantly lower with PT technique (0.0056 ± 0.0011) than with LK (0.0906 ± 0.003 ml) (p<0.01).
CONCLUSION: The proposed technique is a reasonable alternative for minimizing medication loss during intravitreal injection procedures.
Keywords: Angiogenesis inhibitors; Injections; Retinal diseases; Ophthalmologic surgical procedures; Macular degeneration; Drug administration routes; Vitreous body
ABSTRACT
OBJETIVO: Descrever técnica de injeção intravítrea utilizando agulha-seringa de 29 gauge (seringa 29GN) e agulha 21 gauge (G) comercialmente disponíveis, comparando perda de composto associada à aplicação desta técnica com a descrita nas instruções do kit do ranibizumabe (Lucentis®).
MÉTODOS: Dez doses de 0,3 ml de água destilada foram aspiradas com a seringa 29GN e a agulha 21G (técnica PT) e outras dez doses iguais foram aspiradas utilizando-se o kit do Lucentis® (técnica LK). Para aspiração com a técnica PT, a agulha 21G é colocada sobre a seringa 29GN. Depois da aspiração, a agulha 21G é removida e a injeção intravítrea é realizada com a agulha 29G. A técnica LK utiliza seringa de tuberculina de 1 ml acoplada a agulha 18G para aspiração e agulha 30G para injeção intravítrea. Usando balança de precisão, as agulhas de aspiração (21G para PT; 18G para LK) foram pesadas antes e depois da aspiração da água e os complexos agulha-seringa para injeção (29GN para PT; 30G para LK) foram pesados antes da aspiração e após serem esvaziados. Os volumes restantes nas agulhas de aspiração e complexos agulha-seringa foram estimados pela diferença dos pesos em gramas com conversão para mililitros.
RESULTADOS: O volume (ml) residual médio (±DP) das agulhas de aspiração (21G para PT; 18G para LK) foi significativamente menor com a técnica PT (0,0034 ± 0,0016) quando comparado à técnica LK (0,0579 ± 0,0011) (p<0,01). O volume (ml) residual médio (±DP) dos complexos agulha-seringa foi significativamente menor com a técnica PT (0,0056 ± 0,0011) do que LK (0,0906 ± 0,003 ml) (p<0,01).
CONCLUSÃO: A técnica de injeção proposta é uma alternativa razoável para minimizar perda de medicação durante aplicação de injeções intravítreas.
Descritores: Inibidores da angiogênese; Injeções; Doenças retinianas; Procedimentos cirúrgicos oftalmológicos; Degeneração macular; Vias de administração de medicamentos; Corpo vítreo
INTRODUCTION
Drug administration via intravitreal injections is a frequently employed procedure(1-2) in the management of numerous vitreoretinal diseases(3). Intravitreal injections of anti-vascular endothelial growth factor (VEGF) drugs such as pegaptanib, bevacizumab and ranibizumab are used for the treatment of many posterior segment disorders(4-8).
The management of wet age-related macular degeneration using ranibizumab (Lucentis®) (Novartis®, Stein, Switzerland) typically involves many intravitreal injections per patient and, consequently, high drug costs. Outside of the United States of America, ophthalmologists receive Lucentis® as part of a Lucentis® kit, which contains one vial of 0.3 ml/0.3 mg of Lucentis®, one 18G needle (BD® Blunt Fill Needle-Filter, 1.2 mm x 40 mm) for medication aspiration, one 30G needle (BD Microlance® 3, 0.3 mm x 13 mm) for drug injection, and one 1ml tuberculin syringe (BD Plastipak®)(9).
According to the information sheet of Lucentis®, the loss of medication after the procedure is 0.25 ml, considering the bottle dose of 0.3 ml and the injection dose of 0.05 ml. Due to high cost and reduced medication volume per bottle, it is reasonable to use an injection technique with minimum drug loss. Thus, the objective of the present study is to report an intravitreal injection technique that reduces waste of medication and that may be extrapolated for other drugs or compounds.
METHODS
Ten 0.3 ml doses of distilled water were aspirated employing each of 2 different techniques: the one proposed in this study and the one described in Lucentis® printed directions.
Technique description
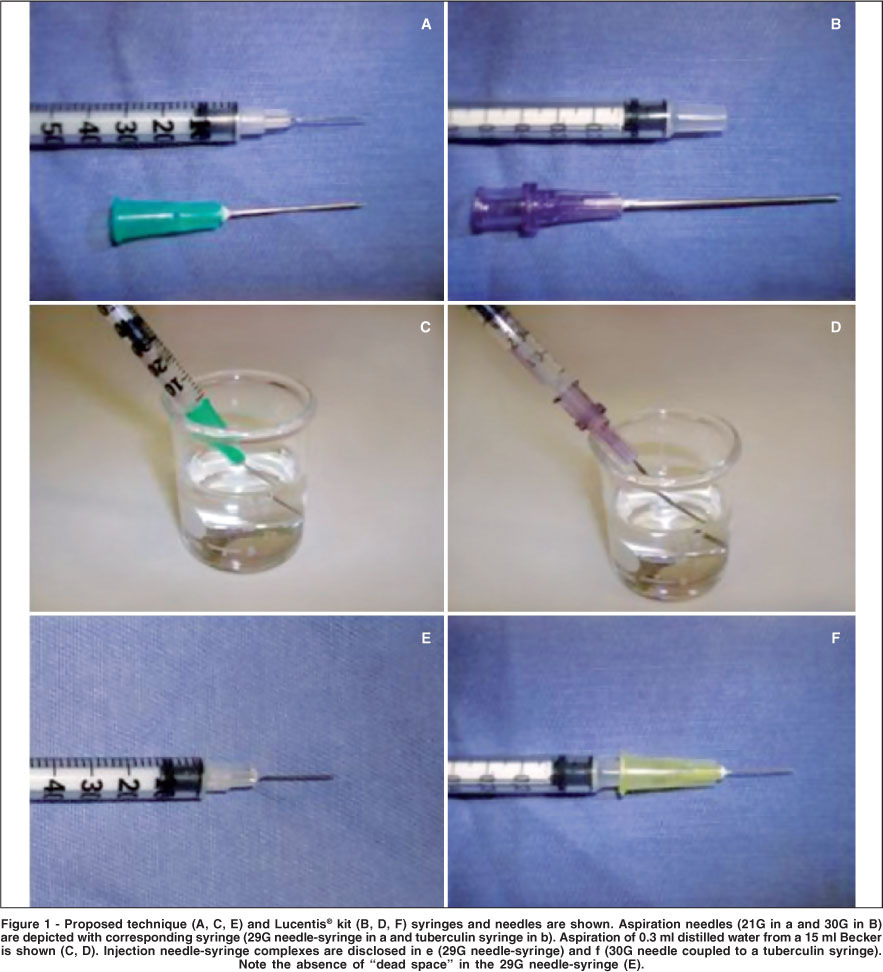
In the proposed technique (PT), a 21 gauge (G) needle (BD PrecisionGlide® 21G; 0.80 mm x 25 mm) was attached over a 29G needle-syringe (BD Ultra-Fine® 29G, Becton Dickinson & Co., Franklin Lakes, NJ) for compound aspiration (Figure 1). After aspiration of 0.3 ml of distilled water from a 5 ml-beaker, the 21G aspiration needle was removed. Subsequently, the water was displaced from the 29G needle-syringe (29GN syringe) with a gentle push of the syringe plunger to the end of the syringe.
Using the Lucentis® technique (LK), an 18G needle was coupled to a tuberculin syringe and 0.3 ml of distilled water was aspirated from a 15 ml-beaker. After aspiration, the 18G needle was removed, a 30G needle was attached to the tuberculin syringe, and water was displaced from the syringe-needle complex with a gentle push of the syringe plunger to the end of the syringe.
Determination of aspiration needles compound loss
Before and after distilled water aspiration, the aspiration needles (21G for the PT; 18G for the LK), without the syringes, were weighed (net weight) using a precision balance (Sartorius® BP 211D, Goettingen, Germany). The difference in weight before and after aspiration was obtained in grams and directly converted into milliliters.
Determination of needle-syringe compound loss
The 29G needle-syringe (BD Ultra-Fine®, Becton Dickinson & Co., Franklin Lakes, NJ) was weighed before distilled water aspiration and again after the distilled water was expressed from the needle-syringe. The same procedure was performed for the 30G needle-tuberculin syringe complex. The difference in weight before aspiration and after emptying was obtained in grams and directly converted into milliliters.
RESULTS
Aspiration needles compound loss
The mean (±SD) residual volume inside aspiration needles (21G for PT; 18G for LK) was 0.0034 ± 0.0016 ml and 0.0579 ± 0.0011 ml, respectively, which corresponds to an average difference of 0.0545 ml (p<0.01). Thus, using the proposed technique one can save approximately 0.05 ml of the compound per injection due to aspiration needles residual mass.
Syringe-needle compound loss
The mean ± SD residual volume inside the combination syringe/needle was 0.0056 ± 0.0011 ml using BD Ultra-fine® 29G, and 0.0906 ± 0.003 ml using the Lucentis® kit, which corresponds to an average difference of 0.0895 ml (p<0.01).
Total compound loss
Thus, using the proposed technique one can save approximately 0.09ml of the compound per injection due to the residual mass in the syringe-needle complex which may represent a total saving of 0.14ml per injection, when also considering the volume saving associated with a change in the aspiration needles.
DISCUSSION
The cost of anti-VEGF drugs may be substantial in the long-term management of patients with age-related macular degeneration. Therefore, an injection technique involving minimal drug waste is important. Syringes with removable needles have a "dead space" in their tip, i.e., space inside the needle where residual compound might accumulate. For example, it has been shown that insulin syringes may retain 0.05 ml of insulin after injection(10).
The mean residual volume left in the needle-syringe complex with the proposed technique (PT) was approximately 0.09 ml less than that left in the needle-syringe complex when using the materials provided in the Lucentis® kit (LK). Further, the residual volume in the aspiration needles was 0.05 ml less with PT than with LK.
Thus, the proposed technique requires a smaller drug volume to be aspirated before the injection of a determined dose due to its reduced medication loss. Also, the use of a 21G needle over the 29G needle-syringe avoids direct contact of the injection needle with drug bottle, preventing damage to the injection needle tip.
CONCLUSION
The technique presented can be implemented easily and may be a reasonable alternative for minimizing medication waste during intravitreal injection of drugs.
The authors would like to thank Professor Fernando de Queiros Cunha and his technician, Sergio Roberto Rosa, for their assistance performing the measurements described in this report.
REFERENCES
1. Aiello LP, Brucker AJ, Chang S, Cunningham ET Jr, D'Amico DJ, Flynn HW Jr, et al. Evolving guidelines for intravitreous injections. Retina. 2004;24(5): S3-19. Comment in: Retina. 2005;25(7):949-50; author reply 950.
2. Bonini-Filho MA, Jorge R, Barbosa JC, Calucci D, Cardillo JA, Costa RA. Intravitreal injection versus sub-Tenon's infusion of triamcinolone acetonide for refractory diabetic macular edema: a randomized clinical trial. Invest Ophthalmol Vis Sci. 2005;46(10):3845-9.
3. Jaissle GB, Szurman P, Bartz-Schmidt KU; German Retina Society; German Society of Ophthalmology; German Professional Association of Ophthalmologists. [Recommendation for the implementation of intravitreal injections-statement of the German Retina Society, the German Society of Ophthalmology (DOG) and the German Professional Association of Ophthalmologists (BVA)]. Klin Monatsbl Augenheilkd. 2005;222(5):390-5. German.
4. Costa RA, Jorge R, Calucci D, Melo LA Jr, Cardillo JA, Scott IU. Intravitreal bevacizumab (Avastin) for central and hemicentral retinal vein occlusions: IBeVO study. Retina. 2007;27(2):141-9.
5. Costa RA, Jorge R, Calucci D, Cardillo JA, Melo LA Jr, Scott IU. Intravitreal bevacizumab for choroidal neovascularization caused by AMD (IBeNA Study): results of a phase 1 dose-escalation study. Invest Ophthalmol Vis Sci. 2006; 47(10):4569-78.
6. Takeda AL, Colquitt J, Clegg AJ, Jones J. Pegaptanib and ranibizumab for neovascular age-related macular degeneration: a systematic review. Br J Ophthalmol. 2007;91(9):1177-82.
7. Fung AE, Rosenfeld PJ, Reichel E. The International Intravitreal Bevacizumab Safety Survey: using the internet to assess drug safety worldwide. Br J Ophthalmol. 2006;90(11):1344-9. Comment in: Br J Ophthalmol. 2006;90(11):1333-4; Br J Ophthalmol. 2006;90(11):1440.
8. Apte RS. Pegaptanib sodium for the treatment of age-related macular degeneration. Expert Opin Pharmacother. 2008;9(3):499-508.
9. Novartis. Lucentis [bula on Internet]. Switzerland: Novartis. [cited 2009 Jan 12]. Available from: http://www.medicinanet.com.br/bula/3194/lucentis.htm
10. Souza CR, Zanetti ML. Administração de. insulina: uma abordagem fundamental na educação em diabetes. Rev Esc Enferm USP 2000;34(3):264-70.
 Address for correspondence:
Address for correspondence:
Rodrigo Jorge
Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo
Av. Bandeirantes, 3.900 - 12o andar do Hospital das Clínicas
Campus USP - Ribeirão Preto (SP) - CEP 14049-900
E-mail: [email protected]
Recebido para publicação em 27.05.2009
Aprovação em 20.07.2009
Institution: Ribeirão Preto School of Medicine University of São Paulo - Ribeirão Preto (SP) - Brazil.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
{kind=link}