Arq. Bras. Oftalmol. 2009; 72 (1): 10.1590/S0004-27492009000100013
Total: 1466
Leão Gabbay Serruya1; Daniel Cruz Nogueira1; Richard Yudi Hida2
DOI: 10.1590/S0004-27492009000100013
ABSTRACT
PURPOSE: To analyze the difference between measurements of Schirmer test I (ST I) and basal Schirmer test (STB) with open and closed eyes. METHODS: Sixty eyes of 30 normal volunteers, 12 males and 18 females aged 28 ± 9 years were recruited for the study. All ST were carried out in a closed environment with the absence of airflow (humidity 60 ± 2.34% and temperature 20.72 ± 1.52ºC). ST I and ST B were performed with the individuals' both eyes open and closed with an interval of 6 hours. All ST were conducted in 5 minutes. For statistical analysis, the ST strip's wetting velocity (ST V) (in millimeters per minute) was calculated, dividing the ST values by its wetting time. If ST values were 35mm before 5 minutes, wetting time was recorded to obtain ST V. RESULTS: ST V measurements of ST I performed with closed eyes (10.30 ± 11.55) were statistically different from those performed with open eyes (18.85 ± 17.88) and ST V measurements of STB performed with closed eyes (3.74 ± 3.14) were statistically different from those performed with open eyes (6.19 ± 5.86). CONCLUSION: ST performed with open or closed eyes can have an important influence in the results of ST I and STB in normal individuals.
Keywords: Dry eye syndromes; Tears; Diagnostic techniques, ophthalmological; Cornea; Keratitis
RESUMO
OBJETIVO: Analisar a diferença das medidas dos testes de Schirmer I e Schirmer basal realizados com os olhos abertos e olhos fechados. MÉTODOS: Foram analisados 60 olhos de 30 indivíduos normais com idade média de 28 ± 9 anos. A umidade média do ar foi de 60 ± 2,34% e a temperatura média de 20,72 ± 1,52ºC. No primeiro dia, foi feito o teste de Schirmer I com os olhos abertos. Após um intervalo de 6 horas, foi realizado o teste de Schirmer I com os olhos fechados. No segundo dia, foi realizado o mesmo procedimento com o teste de Schirmer basal. Para fins de comparação, as medidas das tiras de papel foram divididas pelo tempo de umedecimento das tiras (velocidade) para análise estatística. RESULTADOS:No teste de Schirmer I realizado com os olhos abertos, a medida de umedecimento das tiras mostrou ser estatisticamente maior quando comparado com a medida do mesmo teste realizado com olhos fechados (p<0,0001). No teste de Schirmer basal realizado com os olhos abertos, a medida de umedecimento das tiras mostrou ser estatisticamente maior quando comparado com a medida do mesmo teste realizado com olhos fechados (p<0,0001). CONCLUSÕES: As medidas do teste de Schirmer I com olhos fechados foram estatisticamente diferentes do realizado com olhos abertos. As medidas do teste de Schirmer basal com olhos fechados foram estatisticamente diferentes do realizado com olhos abertos.
Descritores: Síndromes do olho seco; Lágrimas; Técnicas de diagnóstico oftalmológico; Córnea; Ceratite
ORIGINAL ARTICLE
Schirmer test performed with open and closed eyes: variations in normal individuals
Comparação entre os testes de Schirmer em olhos abertos e fechados em indivíduos normais
Leão Gabbay SerruyaI; Daniel Cruz NogueiraII; Richard Yudi HidaIII
IEstagiário em Retina e Vítreo da Santa Casa de Misericórdia de São Paulo - São Paulo (SP) - Brasil
IIEstagiário em Retina e Vítreo da Santa Casa de Misericórdia de São Paulo - São Paulo (SP) - Brasil
IIIDoutorando pela Keio University, Tóquio-Japão; Médico Assistente do Setor de Córnea e Doenças Externas do Departamento de Oftalmologia da Santa Casa de São Paulo - São Paulo (SP) - Brasil; Médico voluntário do Setor de Superfície Ocular do Hospital das Clínicas da Universidade de São Paulo - USP - São Paulo (SP) - Brasil
ABSTRACT
PURPOSE: To analyze the difference between measurements of Schirmer test I (STI) and basal Schirmer test (STB) with open and closed eyes.
METHODS: Sixty eyes of 30 normal volunteers, 12 males and 18 females aged 28 ± 9 years were recruited for the study. All ST were carried out in a closed environment with the absence of airflow (humidity 60 ± 2.34% and temperature 20.72 ± 1.52ºC). STI and STB were performed with the individuals' both eyes open and closed with an interval of 6 hours. All ST were conducted in 5 minutes. For statistical analysis, the ST strip's wetting velocity (STV) (in millimeters per minute) was calculated, dividing the ST values by its wetting time. If ST values were 35mm before 5 minutes, wetting time was recorded to obtain STV.
RESULTS: STV measurements of STI performed with closed eyes (10.30 ± 11.55) were statistically different from those performed with open eyes (18.85 ± 17.88) and STV measurements of STB performed with closed eyes (3.74 ± 3.14) were statistically different from those performed with open eyes (6.19 ± 5.86).
CONCLUSION: ST performed with open or closed eyes can have an important influence in the results of STI and STB in normal individuals.
Keywords: Dry eye syndromes/diagnosis; Tears/secretion; Diagnostic techniques, ophthalmological; Cornea; Keratitis
RESUMO
OBJETIVO: Analisar a diferença das medidas dos testes de Schirmer I e Schirmer basal realizados com os olhos abertos e olhos fechados.
MÉTODOS: Foram analisados 60 olhos de 30 indivíduos normais com idade média de 28 ± 9 anos. A umidade média do ar foi de 60 ± 2,34% e a temperatura média de 20,72 ± 1,52ºC. No primeiro dia, foi feito o teste de Schirmer I com os olhos abertos. Após um intervalo de 6 horas, foi realizado o teste de Schirmer I com os olhos fechados. No segundo dia, foi realizado o mesmo procedimento com o teste de Schirmer basal. Para fins de comparação, as medidas das tiras de papel foram divididas pelo tempo de umedecimento das tiras (velocidade) para análise estatística.
RESULTADOS:No teste de Schirmer I realizado com os olhos abertos, a medida de umedecimento das tiras mostrou ser estatisticamente maior quando comparado com a medida do mesmo teste realizado com olhos fechados (p<0,0001). No teste de Schirmer basal realizado com os olhos abertos, a medida de umedecimento das tiras mostrou ser estatisticamente maior quando comparado com a medida do mesmo teste realizado com olhos fechados (p<0,0001).
CONCLUSÕES: As medidas do teste de Schirmer I com olhos fechados foram estatisticamente diferentes do realizado com olhos abertos. As medidas do teste de Schirmer basal com olhos fechados foram estatisticamente diferentes do realizado com olhos abertos.
Descritores: Síndromes do olho seco/diagnóstico; Lágrimas/secreção; Técnicas de diagnóstico oftalmológico; Córnea; Ceratite
INTRODUCTION
According to the International Dry Eye Workshop(1-2), dry eye is a multifatorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface. According to many authors, dry eye is one of the most frequent conditions in ophthalmologic practice(3), affecting between 15 and 40% of general population. Dry eye often provokes variable symptoms, from light ocular discomfort to incapacity in keeping the eyes open(4-5). Dry eye syndrome is included in the differential diagnosis of every patient presenting any of those symptoms.
Dry eye diagnosis is based on the clinical features and some diagnostic tests. Schirmer test (ST) is one of the most used diagnostic tools in evaluating ocular surface status. Other tests like red phenol thread, break-up-time, rose bengal, fluorescein, lissamine green, impression cytology, biochemist analysis of the tear, interferometry, meniscometry and osmolarity measurement are also used(6-10).
ST was first described by Otto Schirmer in 1903 and consists of the use of a Whatman number 41 special strip, with 5 mm width and 35 mm length placed in lower eyelid. ST without anesthesia or Schirmer I (STI) is a well-standardized test that measures the basal tear secretion with the conjunctival-lacrimal trigeminal reflex(7,11). Basal Schirmer test (STB) is performed with anesthesia and measures the basal lacrimal secretion. Other variations of the ST are not frequently used(6,10).
Schirmer originally described the test to be conducted with the patient seated, with open eyes, blinking freely. Various authors have published articles using the test with the patients remaining with closed eyes(12-15), however, no study found evidence that such results are equivalents to the originally described tests by Schirmer. Recently, according to the 2007 Report of the International Dry Eye Workshop (DEWS), suggested to perform the Schirmer test with the patient's eyes closed(1).
The purpose of this study is to analyze the difference between measurements of STI and STB with open and closed eyes.
METHODS
Sixty eyes of 30 normal volunteers, 12 males and 18 females aged 28 ± 9 years were used for the study. Informed consent was obtained from all subjects. Study methods conformed to the Declaration of Helsinki and the review board of our institution.
All individuals underwent a routine ocular evaluation. Individuals with previous eye surgery, any ocular (dry eye, lid abnormalities, chalasis, meibomitis, blepharitis, corneal scars) or systemic condition that could interfere in the stability of the lacrimal film were excluded from this study. Contact lens users or individuals undergoing any kind of ocular medication were also excluded.
All ST were carried out by the author (LGS) in a closed environment with the absence of airflow. The room was optimized with 60 ± 2.34% humidity and 20.72 ± 1.52ºC temperature to minimize variation. The examination was performed on two days.
On the first day, STI were performed with the individuals' both eyes open and closed with an interval of 6 hours.
On the second day, STB were also performed with the individuals' eyes open and closed with an interval of 6 hours. They were performed using one drop of 0.5% proxymetacaine chloride (Anestalcon®, Alcon) in both eyes, 5 minutes prior to the test. All ST were conducted in 5 minutes.
For statistical analysis, the ST strip's wetting velocity (STV) (mm/min) was calculated, dividing the ST values (mm) by its wetting time (min). If ST values were 35 mm before 5 minutes, wetting time was recorded to obtain STV.
The results were analyzed using Wilcoxon statistical test (95% interval and p<0.05).
RESULTS
Chart 1 shows the mean and standard deviation of STV (mm/min) of STI and STB, with open and closed eyes (Chart 1).
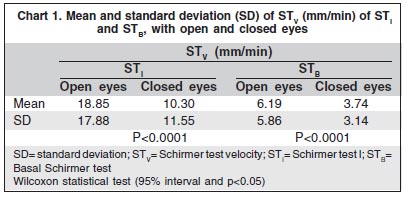
Note that the average STV measurements of STI performed with closed eyes were statistically different from those performed with open eyes (p<0.0001) and measurements of STB performed with closed eyes were statistically different from those performed with open eyes (p<0.0001).
Also note that the average STV performed with closed eyes was reduced in STI (54.64%) and STB (60.42%) when compared to STV performed with open eyes.
DISCUSSION
Some authors, including Otto Schirmer, suggested ST normal wetting length values greater than 15 mm and abnormal when values were less than 6 mm. However, it is not mentioned if test is performed with open or closed eyes(4,6,11). It was originally described with open eyes, allowing the patient to blink freely(4,6-7,11). Some authors affirm that the results of the test do not differ when carried out with open or closed eyes(7-8). However, most studies do not mention which method was used in the tests (open or closed eyes)(16-21) and there are no studies comparing both methods. Many authors have published their results using the test with closed eyes (4,13-15).
In our study, we note that ST values with closed eyes reduced their value by 54.64% for STI and 60.42% for STB. Therefore, it is necessary to accomplish other comparative studies in patients with dry eye, to determine values without the influence of open or closed eyes. There may be a possibility of increasing false-positive rates of dry eye syndrome.
STV was used in this study to allow comparison of values greater that 35 mm and to decrease the possibility of a statistical error. STV may have higher values in the first minutes and diminish gradually during the tests(22-24). STV can also be a parameter for tear volume in humans, but further research should be carried out.
ST has been found to give poor reproducibility for detecting aqueous tear deficiency because it is directly influenced by temperature, humidity, evaporation, reflex tearing. However, it is one of the most common diagnostic tests used worldwide to diagnose aqueous deficiency because it is easy to perform (6-7,11,21,24-25)
CONCLUSION
Schirmer wetting values with open eyes showed significantly higher values when compared to closed eyes. This could probably be explained by the influence of the strip on reflex tearing during blinking. So ST performed with closed eye could diminish variations of humidity, evaporation and specially reflex tearing. Other factors that could have an influence on the ST results, such as head positioning, illumination, position of the strip, corneal condition, humidity and temperature must be analyzed to accomplish standardization of this important diagnostic tool.
The authors believe that the Schirmer test performed with closed eyes could eliminate environmental factors like evaporation and humidity. Therefore, it might be more reproducible, however, other studies are being carried out to clarify such facts.
REFERENCES
1. Research in dry eye: Report of the Research Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):179-93.
2. Design and conduct of clinical trials: Report of the Clinical Trials Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):153-62.
3. Brewitt H, Sistani F. Dry eye disease: the scale of the problem. Surv Ophthalmol. 2001;45(Suppl 2):S199-202.
4. Lemp MA. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. 1995;21(4):221-32.
5. Gilbard JP, Rossi SR, Azar DT, Heyda KG. Effect of punctal occlusion by Freeman silicone plug insertion on tear osmolarity in dry eye disorders. Clao J. 1989;15(3):216-8.
6. Cho P, Yap M. Schirmer test II. A clinical study of its repeatability. Optom Vis Sci. 1993;70(2):157-9.
7. Hida RY, Mascaro VL, Hofling-Lima AL, Goto E, Tsubota K, Gomes JA. Métodos Diagnósticos. In: Gomes JA, Alves MR, editores. Superfície ocular. Rio de Janeiro: Cultura Médica; 2006.
8. Hida RY, Nishiwaki-Dantas MC, Hida MM, Tsubota K. [Quantitative tear study using the red phenol test in the Brazilian population]. Arq Bras Oftalmol. 2005;68(4):433-7. Portuguese.
9. Korb DR. Survey of preferred tests for diagnosis of the tear film and dry eye. Cornea. 2000;19(4):483-6.
10. Nishiwaki-Dantas MC. Olho seco. Arq Bras Oftalmol. 1999;62(1):101-5.
11. Cho P, Yap M. Schirmer test I. A review. Optom Vis Sci. 1993;70(2):152-6.
12. Nichols KK, Mitchell GL, Zadnik K. The repeatability of clinical measurements of dry eye. Cornea. 2004;23(3):272-85.
13. Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004;23(8):762-70.
14. Nichols KK, Nichols JJ, Lynn Mitchell G. The relation between tear film tests in patients with dry eye disease. Ophthalmic Physiol Opt. 2003;23(6):553-60.
15. Lemp MA. Recent developments in dry eye management. Ophthalmology. 1987; 94(10):1299-304.
16. Bawazeer AM, Hodge WG. One-minute Schirmer test with anesthesia. Cornea. 2003;22(4):285-7. Comment in: Cornea. 2004;23(3):318-9; author reply 319.
17. Lima CG, Siqueira GB, Cardoso IH, Sant'Anna AE, Osaki MH. [Evaluation of dry eye in the preoperative and postoperative period of blepharoplasty]. Arq Bras Oftalmol. 2006;69(3):327-82. Portuguese.
18. Ogawa Y, Okamoto S, Wakui M, Watanabe R, Yamada M, Yoshino M, et al. Dry eye after haematopoietic stem cell transplantation. Br J Ophthalmol. 1999; 83(10):1125-30.
19. Shimazaki J, Shimmura S, Fujishima H, Tsubota K. Association of preoperative tear function with surgical outcome in severe Stevens-Johnson syndrome. Ophthalmology. 2000;107(8):1518-23.
20. Toda I, Asano-Kato N, Komai-Hori Y, Tsubota K. Dry eye after laser in situ keratomileusis. Am J Ophthalmol. 2001;132(1):1-7.
21. Tsubota K. Tear dynamics and dry eye. Prog Retin Eye Res. 1998;17(4):565-96.
22. Xu KP, Tsubota K. Correlation of tear clearance rate and fluorophotometric assessment of tear turnover. Br J Ophthalmol. 1995;79(11):1042-5.
23. Holly FJ, Lamberts DW, Esquivel ED. Kinetics of capillary tear flow in the Schirmer strip. Curr Eye Res. 1982;2(1):57-70.
24. Clinch TE, Benedetto DA, Felberg NT, Laibson PR. Schirmer's test. A closer look. Arch Ophthalmol. 1983;101(9):1383-6.
25. Tsubota K. The importance of the Schirmer test with nasal stimulation. Am J Ophthalmol. 1991;111(1):106-8.
 Endereço para correspondência:
Endereço para correspondência:
Leão Gabbay Serruya
Rua Dr. Gabriel dos Santos, 179 - Apto. 12
São Paulo (SP) CEP 01231-011
E-mail: [email protected]
Recebido para publicação em 20.10.2008
Última versão recebida em 02.11.2008
Aprovação em 08.12.2008
Trabalho realizado no Departamento de Oftalmologia da Faculdade de Ciências Médicas da Santa Casa de Misericórdia de São Paulo (FCMSCSP) - São Paulo (SP) - Brasil.
Trabalho de conclusão do curso de Especialização em Oftalmologia do Departamento de Oftalmologia da Santa Casa de Misericórdia de São Paulo - São Paulo (SP) - Brasil.
Nota Editorial: Depois de concluída a análise do artigo sob sigilo editorial e com a anuência do Dr. Procópio Miguel dos Santos sobre a divulgação de seu nome como revisor, agradecemos sua participação neste processo.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.