Arq. Bras. Oftalmol. 2007; 70 (5): 10.1590/S0004-27492007000500019
Total: 2220
Lucia Miriam Dumont Lucci1; Ana Luisa Höfling-Lima2; Clélia Maria Erwenne3; Emanuela Martins de Toledo Cassano
DOI: 10.1590/S0004-27492007000500019
ABSTRACT
PURPOSE: To compare artificial eye amplitudes in enucleated socket with porous polyethylene either spherical or quad-motility implant and study the characteristics of artificial eyes fit with the two orbital implants. METHODS: A total of 21 patients were prospectively studied who underwent enucleation because of an intraocular melanoma and the randomization defined a porous polyethylene either spherical or quad-motility orbital implant. Measurements of the amplitude of the artificial eye were obtained with prism and digital photos. The software Scion Image analyzed the digital photos (www.scioncorp.com) and the quantitative data were allocated to groups. The measurements (height, length, thickness) and weight of the 21 artificial eyes were analyzed. Student's t-test was performed to determine the significance of difference between groups (p<0.05). RESULTS: There was no statistically significant difference of the artificial eye amplitude analyzed by means of prisms between both orbital implants (p>0.05 for all directions). On analyzing the digital photos, the artificial eye with spherical implant showed higher artificial eye amplitude downward (p=0.009) among patients older than 55 years old, rightward (p=0.036) and downward (p=0.008) among the 9 patients with enucleated right eye. Height and length were similar in the 21 artificial eyes but those artificial eyes fit with quad-motility orbital implants were statistically significant thicker (p<0.001) and heavier (p=0.001). CONCLUSIONS: The similar amplitude of movement of artificial eyes was observed with both spherical and quad-motility orbital implants. Artificial eyes fit with quad-motility orbital implant are significantly thicker and heavier than those fit with spherical orbital implant.
Keywords: Eye enucleation; Orbital implants; Eye, artificial; Polyethelene; Image processing, computer-assisted
RESUMO
OBJETIVOS: Comparar a amplitude de movimento da prótese ocular em cavidade enucleada e com implante orbitário esférico e "quad-motility" e estudar as características das próteses oculares adaptadas com os dois modelos de implantes orbitários. MÉTODOS: Vinte e um pacientes foram prospectivamente estudados após a enucleação devido a melanoma intra-ocular e cuja randomização definiu o implante orbitário de polietileno poroso nos modelos esférico e "quad-motility". Medidas da amplitude da prótese ocular foram obtidas com prisma e fotografia digital. O programa Scion Image analisou as fotos digitais (www.scioncorp.com) e os resultados foram distribuídos por grupos. As medidas (altura, comprimento, espessura) e o peso das 21 próteses também foram analisados. O teste de t foi realizado para determinar a significância da diferença entre os grupos (p<0,05). RESULTADOS: Não houve diferença significante na amplitude do movimento das próteses oculares, analisada com a interposição do prisma em ambos implantes orbitários (p>0,05 em todas as posições). Ao analisar a fotografia digital, as próteses adaptadas com implante esférico apresentaram maior amplitude de movimento na infraversão (p=0,009) para pacientes acima de 55 anos, infraversão (p=0,008) e dextroversão (p=0,036) nos nove pacientes com o olho direito enucleado. Altura e comprimento foram similares nas 21 próteses oculares. Próteses oculares adaptadas com implante "quad-motility" foram significantemente mais espessas (p<0,001) e pesadas (p=0,001). CONCLUSÕES: A amplitude de movimento das próteses oculares foi similar nos implantes esférico e "quad-motility". As próteses oculares adaptadas com implante "quad-motility" são significantemente mais espessas e pesadas do que as adaptadas com implante esférico.
Descritores: Enucleação ocular; Implantes orbitários; Olho artificial; Polietileno; Processamento de imagens assistida por computador
ORIGINAL ARTICLE
Artificial eye amplitudes and characteristics in enucleated socket with porous polyethylene spherical and quad-motility implant
Amplitude de movimento e características das próteses oculares em cavidades enucleadas com implante de polietileno poroso esférico e "quad-motility"
Lucia Miriam Dumont LucciI; Ana Luisa Höfling-LimaII; Clélia Maria ErwenneIII; Emanuela Martins de Toledo CassanoIV
IDoutora; Chefe do Setor de Plástica Ocular do Departamento de Oftalmologia da Faculdade de Medicina do ABC - São Paulo (SP) - Brasil
IIProfessora Titular e Chefe do Departamento de Oftalmologia da Universidade Federal de São Paulo - UNIFESP - São Paulo (SP) - Brasil
IIIDoutora; Orientadora do Curso de Pós-Graduação do Departamento de Oftalmologia da UNIFESP - São Paulo (SP) - Brasil
IVOrtoptista e Tecnóloga Oftálmica - São Paulo (SP) - Brasil
ABSTRACT
PURPOSE: To compare artificial eye amplitudes in enucleated socket with porous polyethylene either spherical or quad-motility implant and study the characteristics of artificial eyes fit with the two orbital implants.
METHODS: A total of 21 patients were prospectively studied who underwent enucleation because of an intraocular melanoma and the randomization defined a porous polyethylene either spherical or quad-motility orbital implant. Measurements of the amplitude of the artificial eye were obtained with prism and digital photos. The software Scion Image analyzed the digital photos (www.scioncorp.com) and the quantitative data were allocated to groups. The measurements (height, length, thickness) and weight of the 21 artificial eyes were analyzed. Student's t-test was performed to determine the significance of difference between groups (p<0.05).
RESULTS: There was no statistically significant difference of the artificial eye amplitude analyzed by means of prisms between both orbital implants (p>0.05 for all directions). On analyzing the digital photos, the artificial eye with spherical implant showed higher artificial eye amplitude downward (p=0.009) among patients older than 55 years old, rightward (p=0.036) and downward (p=0.008) among the 9 patients with enucleated right eye. Height and length were similar in the 21 artificial eyes but those artificial eyes fit with quad-motility orbital implants were statistically significant thicker (p<0.001) and heavier (p=0.001).
CONCLUSIONS: The similar amplitude of movement of artificial eyes was observed with both spherical and quad-motility orbital implants. Artificial eyes fit with quad-motility orbital implant are significantly thicker and heavier than those fit with spherical orbital implant.
Keywords: Eye enucleation; Orbital implants; Eye, artificial; Polyethelene; Image processing, computer-assisted/methods
RESUMO
OBJETIVOS: Comparar a amplitude de movimento da prótese ocular em cavidade enucleada e com implante orbitário esférico e "quad-motility" e estudar as características das próteses oculares adaptadas com os dois modelos de implantes orbitários.
MÉTODOS: Vinte e um pacientes foram prospectivamente estudados após a enucleação devido a melanoma intra-ocular e cuja randomização definiu o implante orbitário de polietileno poroso nos modelos esférico e "quad-motility". Medidas da amplitude da prótese ocular foram obtidas com prisma e fotografia digital. O programa Scion Image analisou as fotos digitais (www.scioncorp.com) e os resultados foram distribuídos por grupos. As medidas (altura, comprimento, espessura) e o peso das 21 próteses também foram analisados. O teste de t foi realizado para determinar a significância da diferença entre os grupos (p<0,05).
RESULTADOS: Não houve diferença significante na amplitude do movimento das próteses oculares, analisada com a interposição do prisma em ambos implantes orbitários (p>0,05 em todas as posições). Ao analisar a fotografia digital, as próteses adaptadas com implante esférico apresentaram maior amplitude de movimento na infraversão (p=0,009) para pacientes acima de 55 anos, infraversão (p=0,008) e dextroversão (p=0,036) nos nove pacientes com o olho direito enucleado. Altura e comprimento foram similares nas 21 próteses oculares. Próteses oculares adaptadas com implante "quad-motility" foram significantemente mais espessas (p<0,001) e pesadas (p=0,001).
CONCLUSÕES: A amplitude de movimento das próteses oculares foi similar nos implantes esférico e "quad-motility". As próteses oculares adaptadas com implante "quad-motility" são significantemente mais espessas e pesadas do que as adaptadas com implante esférico.
Descritores: Enucleação ocular; Implantes orbitários; Olho artificial; Polietileno; Processamento de imagens assistida por computador/métodos
INTRODUCTION
Loss of an eye due to tumor, trauma, or end-stage ocular disease is devastating to persons of any age. Not only is there a loss of binocular vision with reduced peripheral visual field and loss of depth perception causing various job restrictions, but also a sense of facial disfigurement. One's self-image, self-esteem, and self-confidence may be affected. Because eye contact is such an essential part in human interaction, it is extremely important for the artificial eye patient to maintain a natural and normal appearance with the prosthetic eye(1-3).
The ideal orbital implant should be able to correct the orbital volume loss as well as maintain socket motility to achieve maximum cosmesis with the use of prosthesis. In addition, it should have low exposure and migration rates, be economical, technically simple to implant, and applicable for enucleation, evisceration or secondary orbital implantation(4).
Porous polyethylene (PP) is made of synthetic material (high-density polyethylene powder), which is heated below the melting point and molded into specific shapes (Medpor®; Porex Surgical Inc., Fairburn, GA, USA)(5-6). Due to its good molding, tissue tolerance, and stability, porous polyethylene has been used in craniofacial reconstructive surgeries since 1982(5) and in enucleation implant since 1989(6). This material has an extensive pore system that permits fibrovascular ingrowths which has the advantage of preventing migration, extrusion, and infection(6). Attachment of the extra-ocular muscles to the implant in locations mimicking their normal anatomical insertion sites optimizes implant movement without increasing the incidence of exposure(7). Porous implants should be used in those patients who express an interest in later peg insertion, a procedure that primarily improves the amplitude of horizontal prosthetic saccades(8). By 2002, PP implants were the most frequently used after primary enucleation (42.7%)(9).
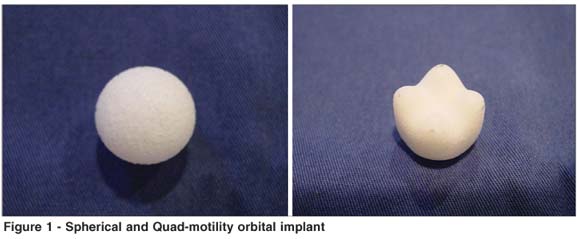
Many shapes of orbital implants have also been developed: the buried implants, magnets, flat anterior surface, tantalum mesh, protruding 4 mounds on the anterior surface(4). PP implants are available in spherical, egg, conical, and mounded shape (quad-motility)(9).
The placement of a peg or screw is often performed as a second procedure several months after initial placement of the orbital implant, but it has been associated with conjunctival breakdown and exposure of the implant, chronic discharge, pyogenic granulation formation, and conjunctival overgrowth(10).
The results of a survey done with active members of the American Society of Ophthalmic Plastic and Reconstructive Surgery (ASOPRS) showed a decline in implant pegging, only 8.1% of all the implants reported were pegged(9).
The motility of a nonintegrated artificial eye may be caused by at least two forces: 1) the rubbing force between the posterior surface of the artificial eye and the conjunctiva that covers the implant may cause the artificial eye to move. Because this force is likely to be approximately equal in all directions, it would cause comparable horizontal and vertical artificial eye amplitudes; 2) an artificial eye usually fits snugly in the conjunctival space (possibly not in the superior fornix). During upgaze and downgaze, the upper and lower eyelids move along with the eye (or implant), albeit with a smaller amplitude. Consequently, the upper and lower fornices also move upward and downward, and thereby contribute to the vertical amplitude of the artificial eye. In contrast, the medial and lateral canthi hardly move during horizontal eye (or implant) movements. Therefore, the medial and lateral conjunctival fornices probably move much less than the upper and lower fornices(11).
The quad-motility implant (Medpor®; Porex Surgical Inc., Fairburn, GA, USA) is a rounded orbital implant with four mounds located anteriorly. The anterior mounds provide projections in the Tenon capsule and conjunctiva that allow coupling of the implant with the ocular prosthesis without penetrating the conjunctiva. These mounds also may partially support the weight of the prosthesis, thereby reducing the amount of weight being supported by the lower eyelid and fornix, which often leads to lower eyelid droop(4).
The quad-motility implant is available in three sizes: small, medium, and large, approximating the volume of a 16-, 18-, and 20- millimeter sphere. The spherical implant is available in four sizes: 16-, 18-, 20-, and 22- millimeter of diameter(4).
Synchronous simultaneous movements of the two eyes in the same direction are called versions. The versions fulfill the first two tasks assigned to the motor system of the eyes: to enlarge the field of view and to bring the object of attention onto the fovea. In this study, prisms were used to evaluate the prosthesis motility based on voluntary version as the patient's only eye was looking to an object located at 1 m of distance. Prisms are able to evaluate the artificial eye amplitude in the central visual field.
To digitalize one image means to give space value (x; y) and the light to the points (pixels) that makes the figure. The image can be analyzed by a specific program that, manipulating mathematics of the pixels, allows to analyze the margins and make the measurements of any parameter(12). Digital photos were taken of each patient in the ocular primary position and at the four main gazes to evaluate the artificial eye amplitude in the external visual field.
In normal individuals there is an age-related decrease in extra-ocular muscle function. Aging anophthalmic patients should exhibit a gradual loss of large-amplitude prosthetic movement, while the animated small-amplitude excursions are preserved. The motility benefits of pegged hydroxyapatite may thus become less significant with advancing age(13).
To evaluate the current assumption that quad-motility orbital implant yields better artificial eye motility than spherical orbital implant, we compared the amplitude and the characteristics of the artificial eye in patients who randomly received either quad-motility or spherical porous polyethylene orbital implant. Prism and digital photos were a quantitative method to analyze the artificial eye amplitude.
METHODS
Patients
Patients from the oncology sector of the Department of Ophthalmology of the Federal University of São Paulo, who underwent enucleation because of an intraocular melanoma, without extrascleral extension on ultrasound examination, were eligible for the study. We excluded patients with a low visual acuity in the remaining eye and patients with a history of strabismus, any eye surgery, or orbital disorders.
A total of 21 patients were eligible for this study. During the surgery, 11 patients received the spherical implant and 10 patients received the quad-motility implant (Figure 1).
The age of the patients ranged from 31 to 80 years. The patients were separated into two groups: under and over 55 years old.
Randomization
The type of implant was selected immediately before surgery by opening an envelope with a previously randomized assignment. The surgeon did not perform the amplitudes of the artificial eye recordings. Until after the artificial eye recordings, the investigators who recorded the eye amplitude, as well as the patients, were unaware of the type of enucleation implant.
Surgical technique
The same surgeon made the 21 surgeries. The patient entered the operation room with a skin mark on the forehead showing the side of the surgery. Enucleation was performed as follows: 1) 360º peritomy, blunt dissection of conjunctiva, under Tenon's capsule and between the rectus muscles; 2) the four rectus muscles were identified with a squint hook and cut from the eye after a 5-0 polyglactin double-armed suture which was passed just posterior to each tendon; 3) the optic nerve was cut with curved scissors; 4) disinsertion of both oblique muscles during the eye removal; 5) hemostasis with finger pressure; 6) implant inserted in the orbit with an implant introducer (the four mounds of the quad-motility implant were located anteriorly); 7) the four rectus muscles were directly sutured on the surface of the orbital implant with 5-0 polyglactin suture; 8) the two oblique muscles were left untagged; 9) the anterior surface of both implants was wrapped with autogenous tissue (deep temporalis fascia); 9) Tenon's capsule and conjunctiva were closed in separate layers with 6-0 polyglactin; and 10) temporary tarsorrhaphy with 4-0 silk.
An algorithm has been developed to determine the appropriate locations for the reattachment of the four rectus muscles (Table 1) on the spherical implant(7). The reattachment of the four rectus muscles on the quad motility was done on the margin of the tunnels among the four mounds.
Follow-up
At the first postoperative visit, the bandage was changed. The second postoperative visit was scheduled 3 days after surgery. At that visit, the bandage and the temporary tarsorrhaphy were removed. The socket was inspected and the patient used topical antibiotics drops four times a day until the 30th postoperative day. The third postoperative visit was 2 weeks after surgery and the conjunctival suture was removed under topical proparacaine hydrochloride 0.5%.
Six weeks after the surgery, the patients were referred to the ocularist to fit the artificial eye. The anterior surface of the artificial eye was made based on the contralateral eye (color of iris, color of sclera, size of pupil) and the posterior surface was made with mold of impression.
The patients returned to the clinic after six weeks for measurements of the amplitude of the artificial eye, which were obtained with a prism and digital photos for primary position, horizontal and vertical movements. The prosthesis was measured using pachymetry (height, length and thickness) and digital balance (weight).
Artificial eye amplitude recordings
Prism was placed in front of the eye and the fixation point was located at one meter. The observer noted the eye and the artificial eye movements. The prismatic dioptria was increased until no improvement in artificial eye motility. The smallest prismatic dioptria that showed the best artificial eye movement, was considered the result.
Photos were taken with digital camera (Sony, Cyber-shot, 3.3 mega pixels) in the primary position and four extreme gaze positions. A standard millimeter ruler was placed close to the artificial eye. The software Scion Image (www.scioncorp.com/scion image_windows.htm) was used to analyze the photos, with a standard way of measurements of the five photos (Figure 2).
Statistical analyses
Statistical analysis was performed with EPI INFO, Version 6.04. Quantitative data for groups (enucleated eye, age and orbital implant) and artificial eyes are presented as mean and standard deviation(14). Student's t-test was performed to determine the significance of differences among groups. The criterion for significance was p<0.05.
RESULTS
Demography
Of a total of 21 patients eligible for this study, 11 were male (52.4%) and 10 were female (47.6%). The age of the patients ranged from 31 to 80 years (mean, 55.3 years), 9 patients being younger than 55 years old and 12 patients older than 55 years old.
Were enucleated 15 OD (71.4%) of which 6 received quad-motility orbital implant and 9 received spherical implant. Among the 6 enucleated OS (28.6%), 4 received quad-motility orbital implant and 2 received spherical implant.
The group who had been fitted with quad-motility orbital implant consisted of 10 patients, 6 males and 4 females. Six patients had the implant in the right orbit and four patients had the implant in the left orbit. The size of the implants was 16 (4 cases), 18 (4 cases) and 20 (2 cases).
The group who had been fitted with spherical implant consisted of 11 patients, 5 males and 6 females. Nine patients had the implant in the right orbit and 2 patients had the implant in the left orbit. The size of the implants was 18 (6 cases) and 20 (5 cases). Size 16 of the spherical implant was not used in this study.
Artificial eye amplitude
Due to the difference of the horizontal versions of the right and left enucleated eyes, the results are shown separated by enucleated eye.
Implant motility appears to decline with age(13) and lower eyelid laxity may decrease the prosthesis motility, because we divided the patients into two groups: younger than 55 years and older than 55 years.
Prisms were used to evaluate the central area of the prosthesis motility and digital photos analyzed the four main extreme gazes.
Prism
The results of the artificial eye motility among the 15 right enucleated eyes and the 6 left enucleated eyes are shown in table 2. No statistically significant difference between the two groups was found for all directions.
The results of the artificial eye motility among the 9 patients younger than 55 years and the 12 older than 55 years are shown in table 3. No statistically significant difference between the two groups was found for all directions.
The results of the artificial eye motility among the 11 spherical orbital implants and the 10 quad-motility orbital implants are shown in table 4. No statistically significant difference between the two groups was found for all directions.
Digital photos
The results of the artificial eye motility among the 15 right enucleated eyes and the 6 left enucleated eyes are shown in table 5. There was a statistically significant difference between the two groups for downward (p=0.008) and rightward (p=0.036) in the 15 right enucleated eyes. No statistically significant difference was found for the other directions.
The results of the artificial eye motility among the patients under and over 55 years are shown in table 6. There was a statistically significant difference between the two groups downward (p=0.009) for patients over 55 years. No statistically significant difference between the two groups was found for any other direction.
The results of the artificial eye motility among the 11 spherical orbital implant and the 10 quad-motility orbital implant are shown in table 7. There was a statistically significant difference between the two groups rightward (p=0.036) and leftward (p=0.036) for patients with spherical orbital implant; leftward (p=0.038) for patients with quad-motility orbital implant. There was no statistically significant difference between the two groups for the others directions.
Artificial eyes measurements
Height and length of both orbital implants are similar. Artificial eyes with quad-motility are thicker (p<0.001) and heavier (p=0.001) than the artificial eyes with spherical orbital implants (Table 8).
DISCUSSION
Soares studied patients with anophthalmic socket for an average follow-up period of 12.5 years. Analyzing the results, he could infer that volume and motility are factors that prevent the contractional process of the anophthalmic socket. The study leads to this conclusion, reinforcing that in order to avoid cavity contraction it is necessary to perform a primary orbital implantation in cases of evisceration or enucleation. It is possible to achieve a good final result by the use of a technically well-fitted artificial eye(15).
Some details of the surgical technique for all patients in this study seem to improve the cosmetic results. The four rectus muscles were directly sutured on the surface of the quad-motility and spherical orbital implant. Other authors have used the same technique(11,16-17), although others have reattached the six muscles(7).
Anderson and co-authors advanced the four extraocular muscles over the front of the implant by suturing the medial and lateral rectus muscle together in the horizontal channel of the implant and suturing the superior and inferior rectus muscles in the vertical channel(4). We believe that this suturing extraocular muscle procedure will block the orbital implant motility. In this study, the suture of the extraocular muscles in the quad-motility was done at the respective margin of each channel. There was no difference of location of the four extraocular muscle sutures in the quad-motility orbital implant like it happens in spherical orbital implants.
The anterior surfaces of both orbital implants were covered with a patch of autogenous material (deep temporalis fascia). A comparative study of bovine pericardium versus homologous sclera as wrapping for hydroxyapatite orbital implants showed a significantly higher incidence of exposure with bovine pericardium(18). The use of banked sclera as a patch may potentially contain human immunodeficiency virus(19) or other infectious agents(20). Temporalis fascia as a patch graft has several advantages. The procedure is safe and may be performed in the same surgical field. As it is an autologous graft, there will no be immunological reaction. There is no risk of disease transmission. The temporalis fascia is a sturdy fibrous tissue thick enough to cover the anterior surface of both orbital implants but thin enough to be concealed, pliable, and easy to work with(21). The placement of unwrapped hydroxyapatite implants after enucleation provides essentially the same motility as wrapped implants(22). The middle path sclera provides the combined advantages of a wrapped implant (additional barrier of protection between the rough surface of the implant and conjunctiva) and an unwrapped implant (better and faster vascularization).
In our study, all patients were referred to the ocularist 6 weeks after surgery. At this postoperative time there was no edema, no conjunctival inflammation or dehiscence. Some authors studied early replacement of the conformer by an ocular prosthesis. It was done in 12 enucleated patients, who were pleased with the cosmetic benefit afforded by the early introduction of the prosthesis(23).
To compare the motility of sclera-covered hydroxyapatite and alloplastic enucleation implants, a retrospective, nonrandomized comparative trial was done with 76 anophthalmic patients, who were examined less than 120 days after surgery. Both orbital implants showed similar movement, although directly coupling hydroxyapatite implants to the prosthesis via the motility peg, provided enhanced prosthetic movement. There appears to be no motility benefit of nonpegged hydroxyapatite over spherical alloplastic implants(24).
By the methodology used in this study, the patients were examined with the artificial eye and the amplitude of movement of the artificial eye was analyzed by two methods: (1) prism and (2) computer program Scion Image. A more detailed statistical analysis was performed of this subset of vertical (up and downward) and horizontal (right and leftward) movement. The enucleated eye was also considered, once right or leftward are done with different muscles when the enucleated eye is the right or the left one.
A randomized trial with the purpose of comparing artificial eye amplitudes in patients who received either a hydroxyapatite or an acrylic, sclera-covered spherical implant after enucleation showed that, when no motility peg is placed, acrylic and hydroxyapatite spherical implants yield comparable saccadic amplitudes of the artificial eye. However, saccadic symmetry did not differ significantly between the acrylic group and the hydroxyapatite group (p>0.1 for any saccadic direction). Artificial eye amplitudes were markedly more restricted horizontally than vertically. In all saccadic directions, the relation between target amplitude and artificial eye amplitude was linear(11).
Larger implants seem to provide improved implant motility, which should result in more dramatic prosthetic movement. Several factors must be considered in choosing the appropriate size of implant for a particular patient. Excessively large implants may increase the risk of extrusion, make prosthesis fitting difficult, or result in patient discomfort. Ideally, sufficient space must remain in the socket to allow fitting of prosthesis with at least 2 ml of volume and approximately 4 mm central thickness(25). In this study, the central thickness of the artificial eye fitted with spherical orbital implant had a mean of 4.5 mm, but with quad-motility orbital implant had a mean of 7.68 mm.
Some authors found that shell volume was broadly related to shell weight, though neither measurement was related to cosmetic result. Those patients without orbital implants had a mean shell weight of 3.1 g, as compared with 2.8 g in those with implants(26). The patients of this study, with spherical orbital implants had a mean artificial eye weight of 1.79 g, as compared with 2.69 g in those with quad-motility orbital implant.
Implant motility appears to decline with age(13). This was demonstrated by our study and it is the reason why patients were divided into two groups of age: younger and older than 55 years, based on the mean age of the 21 patients. In a group of patients younger than 55 years old, there was no difference of artificial eye amplitude for any gaze. In a group of patients older than 55 years, there was statistically significant difference only downward (p=0.009), with spherical orbital implants showing better results.
To evaluate the eyelid position before and after the external prosthesis adaptation, using digital image processing techniques, 18 patients were evaluated at the "Faculdade de Medicina de Botucatu - Universidade Estadual Paulista - UNESP", with and without the external prosthesis. Qualitative and quantitative analysis were made using the Scion Image Program. The image processing allowed objective evaluations of the measures, contributing to the patient follow-up(27). This was also observed in the measurements of this study, which were adequate, simple and reliable in enucleated patients.
Because the image processing was done with extreme gaze in this study, measurements of the prosthesis motility were also obtained with prism, to evaluate central visual field once, in conversational speech ocular movements are limited to low-amplitude saccades within a few degrees of primary position. While tracking objects, the eyes rotate only approximately 10º to 15º before head turn naturally occurs(27). In this study, all results are higher than 15º and artificial eye motility at the central visual field can be considered acceptable for both orbital implants.
Isolated innervations to an extraocular muscle of the eye do not occur, nor can the muscles from one eye alone be innervated. Impulses to perform an eye movement are always integrated, and all ocular movements are associated. Whenever an impulse for the performance of an eye movement is sent out, corresponding muscles of each eye receive equal innervations to contract or relax. In enucleated patients, the only eye is going to focus the object located at 1m of distance and the orbital implant is going to follow the only eye. The eyes move toward the apex of the prisms. If the prisms are placed base-out in front of the eyes, they must converge; if the prisms are placed base-in, the eyes must diverge. If the prisms are placed base-up or base-down, the eyes must perform a vertical movement. The only four main directions were evaluated in this study.
In this study, abduction of the artificial eye is significantly better than adduction for both orbital implant. Others authors compared outcomes of enucleation and evisceration. They concluded that abduction of the orbital implant is also significantly better than adduction in eviscerated eyes and implant motility is greater than prosthesis motility(28).
The efficiency of transmitting movement from the implant to the prosthesis determines the degree of the prosthetic motility. Movement is transmitted from orbital implant through surface tension at the conjunctival-prosthetic interface and movement of the fornices(25). The quad-motility orbital implants have irregularly shaped surfaces that create indirect coupling mechanism between the implant and prosthesis that imparts greater movement to the prosthesis(4,25).
This study showed that spherical and quad motility orbital implants yield comparable artificial eye motility, although the artificial eyes fit with a quad motility orbital implant are thicker and heavier.
REFERENCES
1. Jordan DR, Klapper SR. Surgical techniques in enucleation: the role of various types of implants and the efficacy of pegged and nonpegged approaches. Int Ophthalmol Clin. 2006;46(1):109-32.
2. Amaro TAC, Yazigi L, Erwenne C. Aspectos psicológicos e qualidade de vida em pacientes com melanoma uveal durante o processo de tratamento por remoção do bulbo ocular. Arq Bras Oftalmol. 2006;69(6):889-94.
3. Botelho NLP, Volpini M, Moura EM. Aspectos psicológicos em usuários de prótese ocular. Arq Bras Oftalmol. 2003;66(5):637-46.
4. Anderson RL, Yen MT, Lucci LM, Caruso RT. The quasi-integrated porous polyethylene orbital implant. Ophthal Plast Reconstr Surg. 2002;18(1):50-5.
5. Bilyk JR, Rubin PA, Shore JW. Correction of enophthalmos with porous polyethylene implants. Int Ophthalmol Clin. 1992;32(3):151-6. Review.
6. Karesh JW, Dresner SC. High-density porous polyethylene (Medpor) as a successful anophthalmic socket implant. Ophthalmology. 1994;101(10):1688-95; discussion 1695-6.
7. Custer PL, Trinkaus KM. Volumetric determination of enucleation implant size. Am J Ophthalmol. 1999;128(4):489-94.
8. Custer PL. Enucleation: past, present, and future. Ophthal Plast Reconstr Surg. 2000;16(5):316-21. Comment in: Ophthal Plast Reconstr Surg. 2001;17(3):221-3.
9. Su GW, Yen MT. Current trends in managing the anophthalmic socket after primary enucleation and evisceration. Ophthal Plast Reconstr Surg. 2004; 20(4):274-80.
10. Remulla HD, Rubin PA, Shore JW, Sutula FC, Townsend DJ, Woog JJ, Jahrling KV. Complications of porous spherical orbital implants. Ophthalmology. 1995;102(4):586-93.
11. Colen TP, Paridaens DA, Lemij HG, Mourits MP, van Den Bosch WA. Comparison of artificial eye amplitudes with acrylic and hydroxyapatite spherical enucleation implants. Ophthalmology. 2000;107(10):1889-94.
12. Souza AD, Ruiz EE, Cruz AA. Palpebral fissure morphology segmentation and measurement using image processing. IEEE Eng Med Biol Mag. 2000; 19(1):114-9.
13. Mourits MP, Prummel MF, Wiersinga WM, Koornneef L. Measuring eye movements in Graves ophthalmopathy. Ophthalmology. 1994;101(8):1341-6.
14. Dean AG, Dean JA, Coulombier D, Brendel KA, Smith DC, Burton AH, et al. Epi Info, Version 6.04a: a word processing database, and statistics program for public health on IBM-compatible microcomputers. Atlanta: Centers for Disease Control and Prevention; 1996.
15. Soares EJC. Importância da reconstrução anatômica e funcional da cavidade anoftálmica na prevenção e tratamento do processo de retração dos fórnices conjuntivais [tese]. Minas Gerais: Universidade Federal de Minas Gerais; 1992.
16. Rubin PA, Popham J, Rumelt S, Remulla H, Bilyk JR, Holds J, et al. Enhancement of the cosmetic and functional outcome of enucleation with conical orbital implant. Ophthalmology. 1998;105(5):919-25.
17. Blaydon SM, Shepler TR, Neuhaus RW, White WL, Shore JW. The porous polyethylene (Medpor) spherical orbital implant: a retrospective study of 136 cases. Ophthal Plast Reconstr Surg. 2003;19(5):364-71.
18. Arat YO, Shetlar DJ, Boniuk M. Bovine pericardium versus homologous sclera as a wrapping for hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg. 2003;19(3):189-93.
19. Seiff SR, Chang JS Jr, Hurt MH, Khayam-Bashi H. Polymerase chain reaction identification of human immunodeficiency virus-1 in preserved human sclera. Am J Ophthalmol. 1994;118(4):528-30.
20. Lucci LM, Yu MC, Höfling-Lima AL. Decontamination of human sclera: an in vitro study. Cornea. 1999;18(5):595-8.
21. Pelletier CR, Jordan DR, Gilberg SM. Use of temporalis fascia for exposed hydroxyapatite orbital implants. Ophthal Plast Reconstr Surg. 1998;14(3): 198-203.
22. Long JA, Tann TM 3rd, Bearden WH 3rd, Callahan MA. Enucleation: is wrapping the implant necessary for optimal motility? Ophthal Plast Reconstr Surg. 2003;19(3):194-7.
23. Chin K, Margolin CB, Finger PT. Early ocular prosthesis insertion improves quality of life after enucleation. Optometry. 2006;77(2):71-5.
24. Custer PL, Trinkaus KM, Fornoff J. Comparative motility of hydroxyapatite and alloplastic enucleation implants. Ophthalmology. 1999;106(3):513-6.
25. Tyers AG, Collin JR. Baseball orbital implants: a review of 39 patients. Br J Ophthalmol. 1985;69(6):438-42.
26. Smerdon DL, Sutton GA. Analysis of the factors involved in cosmetic failure following excision of the eye. Br J Ophthalmol. 1988;72(10):768-73.
27. Takahagi RU, Gonçalves F, Schellini SA, Padovani CR, Padovani CRP. Avaliação quantitativa das dimensões óculo-palpebrais em portadores de cavidade anoftálmica em uso de prótese ocular externa. Arq Bras Oftalmol. 2005;68(4): 517-20.
28. Nakra T, Simon GJ, Douglas RS, Schwarcz RM, McCann JD, Goldberg RA. Comparing outcomes of enucleation and evisceration. Ophthalmology. 2006; 113(12):2270-5.
 Address for correspondence:
Address for correspondence:
Lucia Miriam Dumont Lucci
Rua Viradouro, 63 - 3º Andar
São Paulo (SP) - CEP 04538-110
E-mail: [email protected]
Recebido para publicação em 07.11.2006
Última versão recebida em 18.05.2007
Aprovação em 18.07.2007
The authors have no financial interest in any of the proprietary materials discussed in this study.
Nota Editorial: Depois de concluída a análise do artigo sob sigilo editorial e com a anuência do Dr. Davi Araf sobre a divulgação de seu nome como revisor, agradecemos sua participação neste processo.
From the Department of Ophthalmology, Federal University of São Paulo - UNIFESP - São Paulo (SP) - Brasil.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.