

Elif Ertan1; Reşat Duman2; Rahmi Duman3; Mustafa Doğan2
DOI: 10.5935/0004-2749.20200065
ABSTRACT
This report describes the therapeutic effects and outcomes of an accidental injection of an intralenticular sustained-release dexamethasone implant (Ozurdex®) in three patients with diabetic macular edema. All three patients underwent accidental injections of sustained-release intravitreal dexamethasone implants into the crystalline lens by the same surgeon. After the accidental injection of Ozurdex® into the crystalline lens, a remarkable reduction in the macular edema and an improvement in visual acuity were observed, suggesting that a positive outcome can be achieved without immediate surgery.
Keywords: Macular edema; Diabetic retinopathy; Dexamethasone/administration & dosage; Intravitreal injections; Lens, crystalline; Drug implants; Visual acuity; Humans
RESUMO
Este estudo descreve os efeitos terapêuticos e os resultados de uma injeção acidental de implante intralenticular de dexametasona de liberação sustentada (Ozurdex®) em três pacientes com edema macular diabético. Todos os três pacientes foram submetidos a injeções acidentais de implantes intravítreos de dexametasona de liberação sustentada na lente do cristalino pelo mesmo cirurgião. Após a injeção acidental de Ozurdex® na lente do cristalino, observou-se uma redução notável no edema macular e uma melhora na acuidade visual, sugerindo que um resultado positivo pode ser alcançado sem cirurgia imediata.
Descritores: Edema macular; Retinopatia diabética; Dexametasona/administração & dosagem; Injeções intravítreas; Cristalino; Implantes de medicamentos; Acuidade visual; Humanos
INTRODUCTION
Ozurdex® (Allergan, Inc., Irvine, CA, USA) is a dexamethasone implant that is approved for the treatment of macular edema due to branch or central retinal vein occlusion, diabetic macular edema (DME), and noninfectious uveitis affecting the posterior segment(1). Ozurdex® is associated with ocular side effects, including conjunctival hemorrhage, endophthalmitis, cataracts, glaucoma, and retinal detachment(2). Accidental injections of Ozurdex® into the crystalline lens have rarely been described in the literature(3,4). In this report, we describe the cases of three patients who experienced lens damage following the injection of a dexamethasone implant for the treatment of DME.
CASE REPORT
Case 1
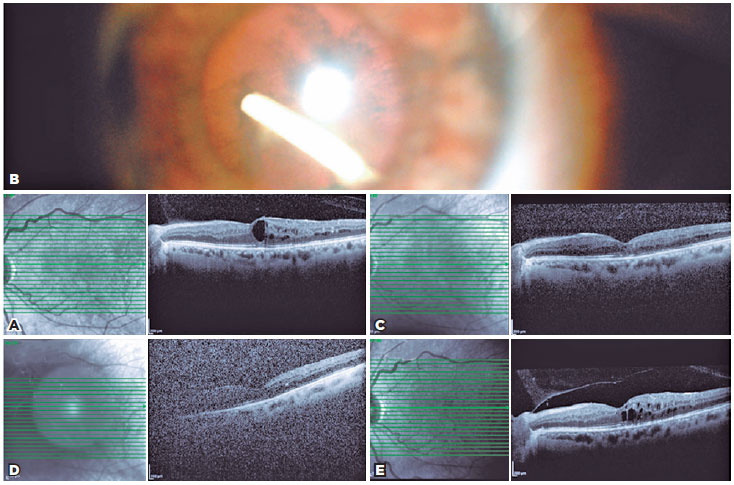
A 56-year-old woman presented with DME. Her best-corrected visual acuity (BCVA) measured 20/200, intraocular pressure (IOP) was 13 mmHg, and central macular thickness (CMT) was 400 µm in the left eye (Figure 1A). She had undergone five previous intravitreal injections of ranibizumab for her DME. Ozurdex® implant injection was performed owing to the presence of persistent DME. Following topical anesthesia with proparacaine, the implant was injected via the pars plana route 3.5 mm from the limbus. At one month after injection, slit-lamp examination revealed that the implant was located in the inferotemporal quadrant of the lens (Figure 1B) and that macular edema had resolved. Optical coherence tomography (OCT) scanning showed that the CMT had regressed from 400 to 266 µm (Figure 1C). Additionally, her BCVA measured 20/100 and IOP was 18 mmHg in the left eye. Conservative management was continued in order to determine whether the implant could be effective in the treatment of her macular edema. At three months after injection, the CMT increased from 266 to 320 µm (Figure 1D) and her BCVA decreased from 20/100 to 20/200. Surgery was planned because of cataract progression. Phacoemulsification surgery was performed at three months after injection. During phacoemulsification, Ozurdex® was divided with the crystalline lens and aspirated with a hacoemulsification probe. During phacoemulsification, posterior capsulorhexis was performed and a monofocal hydrophobic 24.00 D intraocular lens (IOL) was placed in the bag. The IOL was well centered at one week postoperatively, and the IOP was within the normal limit. At one month postoperatively, her BCVA measured 20/125, IOP was 16 mmHg, and CMT was 341 µm in the left eye (Figure 1E).
Case 2
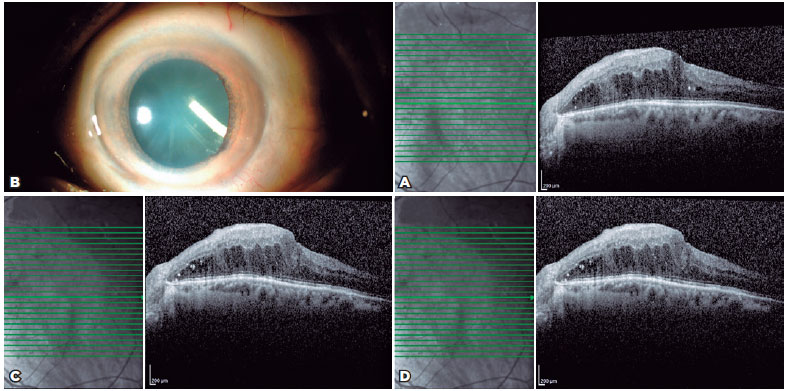
A 78-year-old man presented with DME. His BCVA measured 20/100, IOP was 18 mmHg, and CMT was 506 µm in the left eye (Figure 2A). He had previously received 10 intravitreal injections of ranibizumab for his DME. Owing to the presence of recurrent DME, Ozurdex® implant injection was performed. The implant was injected via the pars plana route 3.5 mm from the limbus, following topical anesthesia with proparacaine. At one month after injection, slit-lamp examination revealed that the implant was located in the inferotemporal quadrant of the lens (Figure 2B). Furthermore, his BCVA measured 20/125 and CMT did not decrease (Figura 2C). At the two-month follow-up, cataract progression requiring intervention was observed and his macular edema remained unresolved. His preoperative BCVA measured 20/160 and CMT was 454 µm. During phacoemulsification, Ozurdex® was divided with the crystalline lens and aspirated with a phacoemulsification probe. A monofocal hydrophobic 19.00 D IOL was placed in the bag. One day postoperatively, the IOL was well centered and the IOP was within the normal limit. At one month postoperatively, his BCVA measured 20/160 and CMT was 460 µm (Figure 2D).
Case 3
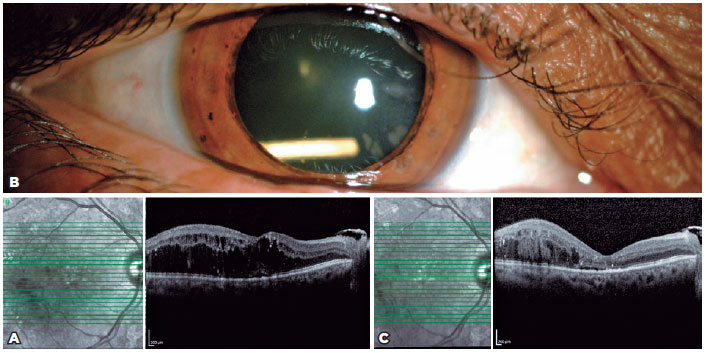
A 57-year-old woman presented with DME (Figure 3A). Her BCVA measured 20/200 and IOP was 19 mmHg in the right eye. She had received 13 previous intravitreal injections of ranibizumab for her DME. Ozurdex® implant injection was performed owing to the presence of recurrent DME. The implant was injected via the pars plana route 3.5 mm from the limbus, following topical anesthesia with proparacaine. At one month postoperatively, slit-lamp examination revealed that the implant was located in the inferotemporal quadrant of the lens (Figure 3B). Moreover, her macular edema had resolved and OCT scanning revealed that her CMT had decreased from 560 to 237 µm (Figure 3C), with the IOP being within the normal limit. Conservative management was continued to determine the effectiveness of the implant. At five months after injection, her CMT had increased from 237 to 353 µm, BCVA measured 20/400, and IOP was 20 mmHg. There was significant cataract progression; therefore, phacoemulsification surgery was performed at five months post-after injection. During phacoemulsification, posterior capsulorhexis and anterior vitrectomy were performed and a three-piece hydrophobic 21.00 D IOL (AR40E, AMO; Abbott) was placed in the sulcus. The IOL was well centered at one day postoperatively, and her IOP was within the normal limit. At one month postoperatively, her BCVA measured 20/200 and CMT was 353 µm.
DISCUSSION
Accidental injection of a sustained-release intravitreal dexamethasone implant into the crystalline lens is an uncommon complication that may be due to inexperience, using an improper technique, and/or uncontrolled head movement during injection. There have been a few case reports regarding this complication(5,6). Fasce et al. described two patients who experienced lens damage following the injection of dexamethasone implants for the treatment of macular edema associated with central retinal vein occlusion. At one week after injection, cataract extraction was performed in the first patient(7). Phacoemulsification surgery was performed at two months after injection in the second patient.
In our second patient, the macular edema was unresolved, presumably because the dexamethasone implant had not protruded as far into the vitreous cavity as it had in the first and third patients. Abdolrahimzadeh et al. reported the intralenticular retention of a dexamethasone implant in a patient who demonstrated resolution of macular edema and lack of cataract progression within the eight-month follow-up period(8). Sekeroglu et al. reported the accidental injection of a sustained-release intravitreal dexamethasone implant into the crystalline lens in one patient; notably, the patient underwent phacoemulsification surgery at seven months after injection(5). These reports provide evidence of the therapeutic efficacy of inadvertent intralenticular injection of Ozurdex®. In our first and third cases, the macular edema had resolved, presumably because the dexamethasone implant was only partially inside the lens and protruded into the vitreous cavity; therefore, the implants continued to be effective in the eye. In the first patient, phacoemulsification surgery was performed at three months after injection because of cataract progression. In the third patient, phacoemulsification surgery was performed at five months after injection, also because of cataract progression.
A frequent treatment using intralenticular Ozurdex® is to perform immediate phacoemulsification with IOL implantation and then reposition the Ozurdex® into the vitreous cavity(4). An alternative approach is conservative management, in which phacoemulsification is not immediately performed if there is no significant decrease in the macular edema and an improvement in visual acuity is observed.
Here, we have described three patients who experienced an accidental injection of sustained-release intravitreal dexamethasone implants into the crystalline lens by the same surgeon; this complication was a result of the surgeon’s inexperience. Importantly, this type of complication can be prevented by thorough technical training on a reassured patient. After an accidental injection of Ozurdex® into the crystalline lens, a remarkable reduction in macular edema and an improvement in visual acuity may also be achieved without immediate surgery.
REFERENCES
1. Haller JA, Bandello F, Belfort R Jr, Blumenkranz MS, Gillies M, Heier J, Loewenstein A, Yoon YH, Jacques ML, Jiao J, Li XY, Whitcup SM; OZURDEX GENEVA Study Group. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology. 2010;117(6):1134-1146.e3. Comment in: Ophthalmology. 2010; 117(6):1061-3.
2. Schmitz K, Maier M, Clemens CR, Höhn F, Wachtlin J, Lehmann F, Bertelmann T,Rüdiger K, Horn M, Bezatis A, Spital G, Meyer CH; German Retinal Vein Occlusion Group. [Reliability and safety of intravitreal Ozurdex injections. The ZERO study]. Ophthalmologe. 2014;111(1):44-52.German.
3. Berarducci A, Sian IS, Ling R. Inadvertent dexamethasone implant injection into the lens body management.Eur J Ophthalmol. 2014;24(4):620-2. Comment in: Eur J Ophthalmol. 2015;25(5): e101-2.
4. Munteanu M, Rosca C. Repositioning and follow-up of intralenticular dexamethasone implant. J Cataract Refract Surg. 2013; 39(8):1271-4.
5. Sekeroglu MA, Anayol MA, Koc F, Tirhis H, Ozkan SS, Yimazbas P. Intralenticularsustained-release dexamethasone implant: is it still effective on macular edema? Case Rep Ophthalmol. 2016;7(1):85-9.
6. Chhabra R, Kopsidas K, Mahmood S. Accidental insertion of dexamethasone implant into the crystalline lens 12 months follow-up. Eye (Lond). 2014;28(5):624-5. Comment in: Eye (Lond). 2014;28(12):1523-4. Eye (Lond). 2014;28(12):1524-5.
7. Fasce F, Battaglia Parodi M, Knutsson KA, Spinelli A, Mauceri P, Bolognesi G, et al. Accidental injection of dexamethasone intravitreal implant in the crystalline lens. ActaOphthalmol. 2014;92(4):e330-1.
8. Abdolrahimzadeh S, Plateroti P, Scarinci F, Plateroti AM. Accidental intralenticular dexamethasone intravitreal implant with the resolution of macular oedema in central retinal vein occlusion. ActaOphthalmol. 2016;94(8):e810-e811.
Submitted for publication:
May 20, 2019.
Accepted for publication:
August 15, 2019.
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Informed consent was obtained from all patients included in this study.
© 2024 - All rights reserved - Conselho Brasileiro de Oftalmologia
![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
