

Mário Luiz Ribeiro Monteiro1
DOI: 10.1590/S0004-27492013000500018
LETTERS TO THE EDITOR CARTAS AO EDITOR
Reply: Fibrin-like material in the retinal arterioles and fluorescein angiography findings in Susac syndrome
Material semelhante à fibrina em arteríolas retínicas e achados de angiografia fluoresceínica na síndrome de Susac
Mário Luiz Ribeiro Monteiro
Physician, Medical School, University of São Paulo, USP - São Paulo (SP), Brazil
We thank Dr. Egan for his comments regarding our paper(1) and for the opportunity to further discuss Susac syndrome (SS), a unique condition which has held our greatest interest for many years. Soon after the first two cases reported by Susac et al.(2), we examined four cases reported in two sequential publications(3,4) that allowed its characterization as "A microangiopathic syndrome of encephalopathy, hearing loss, and retinal arteriolar occlusions"(4). We would like to point out that, as a fellow of Dr. W. F. Hoyt, we shared cases with him and significantly influenced him in naming the condition SS at a Symposium in 1986 when another case was presented to him for discussion by Susac(5). Interestingly, very little has changed in our understanding of the disease for more than three decades. Dr. Egan discussed topics in which our knowledge has advanced, the main one being the findings on magnetic resonance imaging (MRI). While MRI abnormalities were initially observed(4), subsequent advances in technology allowed to identify typical lesions in the corpus callosum(6), which are extremely important in the differential diagnosis and of which our recent case is an example(1). He also shares our point that central retinal artery occlusion is in very unusual and a more recently observed occurrence as the disease preferentially affects arterioles in the periphery of the retina(3,4).
As for the observation regarding the material presented in the arteries of our case (Figure 1A, B and E), although we admit that it was somewhat larger than usual, we do not think it argues against SS. In fact, early on we observed that "the blood column reflex of several arterioles was partially or totally substituted by long segments of fibrin-like white material" (see figure 2 in Monteiro et al.(4)). We have seen similar findings in other cases and it is our understanding that these segments of fibrin-like material are also characteristic of SS and differ from platelet emboli mainly because they are located along the arteriole and not at its bifurcation. These fibrin-like material frequently decreases in size or disappear during follow-up, as observed in our case (Figure 1C, D, F and Gs), sometimes resembling the small Gass plaques reported by Egan et al.(7), and suggesting that the two findings lie within a spectrum of the same phenomenon in SS.
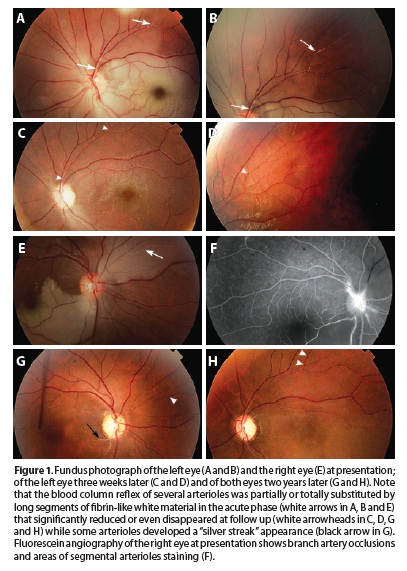
We agree that fluorescein angiography is important not only to show arteriolar occlusions but also to show segmental arteriolar staining(8), as observed in our current case (Figure 1 F). This finding, supports our initial suggestion that SS was an autoimmune disease against some unknown antigen present in the endothelium which has a blood-tissue barrier mechanism, as observed in the retina, cochlea and brain(3,4). Finally, we did not observe abnormalities in the initially unaffected eye of our case but unfortunately a fluorescein angiography was not performed until the second eye was involved; nor did we test the patient for recently described anti-endothelial cell antibodies. On the other hand, we do share Dr. Egan's interest in knowing whether arteriolar staining on fluorescein angiography or Gass plaques on fundus observation could precede retinal arterial occlusions and certainly hope that further studies will be able to clarify this issue.
REFERENCES
1. Apostolos-Pereira SL dos, Kara-Jose LB, Marchiori PE, Monteiro ML. Unilateral central retinal artery occlusion as the sole presenting sign of Susac syndrome in a young man: case report. Arq Bras Oftalmol. 2013;76(3):192-4.
2. Susac JO, Hardman JM, Selhorst JB. Microangiopathy of the brain and retina. Neurology. 1979;29(3):313-6.
3. Coppeto JR, Currie JN, Monteiro ML, Lessell S. A syndrome of arterial-occlusive retinopathy and encephalopathy. Am J Ophthalmol. 1984;98(2):189-202.
4. Monteiro ML, Swanson RA, Coppeto JR, Cuneo RA, DeArmond SJ, Prusiner SB. A microangiopathic syndrome of encephalopathy, hearing loss, and retinal arteriolar occlusions. Neurology. 1985;35(8):1113-21.
5. Susac JO. Susac's syndrome: the triad of microangiopathy of the brain and retina with hearing loss in young women. Neurology. 1994;44(4):591-3.
6. Susac JO, Murtagh FR, Egan RA, Berger JR, Bakshi R, Lincoff N, et al. MRI findings in Susac's syndrome. Neurology. 2003;61(12):1783-7. Comment in: Neurology. 2004; 63(4):761; author reply 761.
7. Egan RA, Ha Nguyen T, Gass JD, Rizzo JF 3rd, Tivnan J, Susac JO. Retinal arterial wall plaques in Susac syndrome. Am J Ophthalmol. 2003;135(4):483-6.
8. Egan RA, Hills WL, Susac JO. Gass plaques and fluorescein leakage in Susac Syndrome. J Neurol Sci. 15 2010;299(1-2):97-100.
 Correspondence address:
Correspondence address:
Mário Luiz Ribeiro Monteiro.
Neuro-Ophthalmology Service. Escola de Medicina da Universidade de São Paulo.
Av. Angélica, 1.757 - Conj. 61 - São Paulo (SP) - 01227-200 - Brazil
E-mail: [email protected]
Submitted for publication: September 16, 2013
Accepted for publication: October 1, 2013
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: M.L.R.Monteiro, None.
© 2024 - All rights reserved - Conselho Brasileiro de Oftalmologia
![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Scielo
Scielo
 Pocket
Pocket
