

Teissy Osaki1; Midori Hentona Osaki2; Tammy Hentona Osaki3
DOI: 10.1590/S0004-27492010000200004
ABSTRACT
PURPOSE: To evaluate the use of octyl-2-cyanoacrylate liquid bandage (Band-Aid liquid®, Ethicon, Johnson & Johnson, New Jersey, USA) as a temporary treatment in patients awaiting surgical repair for involutional entropion. METHODS: Thirteen patients (15 eyelids) with involutional entropion were evaluated while they waited for surgical intervention. The lids were repositioned by the application of octyl-2-cyanoacrylate liquid bandage in the malar fold. Patients were followed-up at days 1, 7 and 15. Assessment and duration of correction were recorded. RESULTS: All the patients presented successful correction at day 1, with significant improvements in signs and symptoms. The mean duration of action of the octyl2-cyanoacrylate liquid bandage was three days. No ocular or dermatological reactions were noted. CONCLUSION: Octyl-2-cyanoacrylate liquid bandage showed to be a simple, safe and effective option to temporarily treat involutional entropion, while patients waited for surgical intervention.
Keywords: Entropion; Tissue adhesives; Eyelids diseases
RESUMO
OBJETIVO: Avaliar o uso de octil-2-cianoacrilato (Band-Aid liquid®, Ethicon, Johnson & Johnson, New Jersey, EUA) como tratamento temporário em pacientes com entrópio involucional, enquanto aguardam cirurgia. MÉTODOS: Foram avaliados treze pacientes (15 pálpebras) com entrópio involucional enquanto aguardavam tratamento cirúrgico definitivo. As pálpebras foram reposicionadas através da aplicação de octil-2-cianoacrilato na prega malar. Os pacientes foram avaliados nos dias 1, 7 e 15. Foram descritos os resultados e duração da aplicação. RESULTADOS: Todos os pacientes apresentaram melhora satisfatória da posição palpebral no dia 1, com melhora significativa dos sinais e sintomas. A média de duração da ação do octil-2-cianoacrilato foi de três dias. Não foram observadas reações dermatológicas ou oculares. CONCLUSÃO: Octil-2-cianoacrilato mostrou-se como uma alternativa simples, segura e eficaz para o tratamento temporário do entrópio involucional, enquanto os pacientes aguardavam a realização do tratamento cirúrgico.
Descritores: Entrópio; Adesivos teciduais; Doenças palpebrais
ORIGINAL ARTICLE
Temporary management of involutional entropion with octyl-2-cyanoacrylate liquid bandage application
Tratamento temporário do entrópio involucional com octil-2-cianoacrilato
Teissy OsakiI; Midori Hentona OsakiII; Tammy Hentona OsakiIII
IResident at the Vision Institute - UNIFESP - São Paulo (SP) - Brazil
IIHead of the Oculoplastic Surgery Sector, Vision Institute - UNIFESP - São Paulo (SP) - Brazil
IIIPostgraduate student, Oculoplastic Surgery Sector, Vision Institute - UNIFESP - São Paulo (SP) - Brazil
ABSTRACT
PURPOSE: To evaluate the use of octyl-2-cyanoacrylate liquid bandage (Band-Aid liquid®, Ethicon, Johnson & Johnson, New Jersey, USA) as a temporary treatment in patients awaiting surgical repair for involutional entropion.
METHODS: Thirteen patients (15 eyelids) with involutional entropion were evaluated while they waited for surgical intervention. The lids were repositioned by the application of octyl-2-cyanoacrylate liquid bandage in the malar fold. Patients were followed-up at days 1, 7 and 15. Assessment and duration of correction were recorded.
RESULTS: All the patients presented successful correction at day 1, with significant improvements in signs and symptoms. The mean duration of action of the octyl2-cyanoacrylate liquid bandage was three days. No ocular or dermatological reactions were noted.
CONCLUSION: Octyl-2-cyanoacrylate liquid bandage showed to be a simple, safe and effective option to temporarily treat involutional entropion, while patients waited for surgical intervention.
Keywords: Entropion/therapy; Tissue adhesives/therapeutic use; Eyelids diseases/therapy
RESUMO
OBJETIVO: Avaliar o uso de octil-2-cianoacrilato (Band-Aid liquid®, Ethicon, Johnson & Johnson, New Jersey, EUA) como tratamento temporário em pacientes com entrópio involucional, enquanto aguardam cirurgia.
MÉTODOS: Foram avaliados treze pacientes (15 pálpebras) com entrópio involucional enquanto aguardavam tratamento cirúrgico definitivo. As pálpebras foram reposicionadas através da aplicação de octil-2-cianoacrilato na prega malar. Os pacientes foram avaliados nos dias 1, 7 e 15. Foram descritos os resultados e duração da aplicação.
RESULTADOS: Todos os pacientes apresentaram melhora satisfatória da posição palpebral no dia 1, com melhora significativa dos sinais e sintomas. A média de duração da ação do octil-2-cianoacrilato foi de três dias. Não foram observadas reações dermatológicas ou oculares.
CONCLUSÃO: Octil-2-cianoacrilato mostrou-se como uma alternativa simples, segura e eficaz para o tratamento temporário do entrópio involucional, enquanto os pacientes aguardavam a realização do tratamento cirúrgico.
Descritores: Entrópio/terapia; Adesivos teciduais/uso terapêutico; Doenças palpebrais/terapia
INTRODUCTION
Entropion is defined as an inward rotation of the eyelid margin. Four main types of entropion have been described: congenital, acute spastic, cicatricial and involutional. Involutional entropion is the most commonly encountered type of entropion. It affects the inferior eyelid and is a relatively common problem in the elderly population(1-2).
Involutional entropion may occur unilaterally or bilaterally and may be obvious or subclinical at presentation. During the closure of the eyes, the lower lid margin rolls inward, causing keratopathy (keratitis, corneal deepithelialization and eventually corneal ulcers) due to the rubbing of the lashes and consequently foreign body sensation, tearing and ocular irritation(1,3). Involutional entropion is associated with several causative factors, including: (1) loss of horizontal lid support with canthal tendon laxity; (2) loss of vertical lid support with tarsal plate thinning; (3) attenuation, dehiscence, or disinsertion of the lower lid retractors; (4) orbicularis muscle dysfunction with the preseptal portion overriding the pretarsal portion and (5) enophthalmos caused by orbital fat atrophy(1-5).
It was observed that tarsal plates are smaller than age-normal in involutional entropion, suggesting atrophy or shrinkage of the tarsus with age, more marked in women, which contributes to involutional entropion. This eyelid malposition can also result from the mechanical effect of an atrophied or smaller-than-age tarsal plate being overcome by the normal or increased tone of the preseptal/pretarsal orbicularis muscle(5).
Surgery remains the best option for permanent treatment of involutional entropion. There are several surgical techniques described in the literature. The technique that consists in retractors plication in tarsus gives the best results in terms of improvement of horizontal lid laxity. This technique presents a low incidence of entropion recurrence. It can be performed either cutaneously or transconjunctivally and sometimes needs to be associated with the tarsal strip technique(1-2,4,6-9).
Cyanoacrylates are liquid monomers that can polymerize rapidly to form a strong adhesive(10). These polymers have been used with apparent safety and efficacy in ophthalmologic applications for more than 30 years(11). During this time, numerous reports have described their use in the cornea, sclera, eyelid skin grafts, mucous membrane grafts in socket reconstruction and daily application to treat severe blepharoptosis(12-15).
This case series was designed to evaluate the use of octyl-2cyanoacrylate liquid bandage as a temporary and innovative treatment in patients awaiting surgical repair for involutional entropion.
METHODS
This study was approved by the Ethics Committee of the Federal University of São Paulo and follows the tenets of the Declaration of Helsinki. Signed informed consent was obtained from all patients.
Thirteen consecutive patients (15 lower eyelids) with involutional entropion were evaluated from February to September 2008, while they were waiting for surgical intervention. Of these thirteen patients, eight were female. The average age was 73.6 ± 6.2 (range: 65 to 87) years old. All patients were functionally symptomatic at the time of presentation with some combination of the following: foreign body sensation, excessive tearing and ocular hyperemia. Patients with previous entropion surgery, other entropion types or any other conjunctival or skin pathology were excluded.
Procedure
Octyl-2-cyanoacrylate liquid bandage (Band-Aid liquid®, Ethicon, Johnson & Johnson, New Jersey, NJ, USA) is a topical skin treatment for minor cuts and abrasions. This product creates a polymeric layer which binds to the skin. Patients underwent treatment with this product to relieve symptoms caused by involutional entropion. It was applied with a swab at the malar fold and allowed to set for 1 minute. After 1 minute, an eyelid sulcus was induced using a plastic 'Y-shaped' stick, resulting in shortening of the anterior lamella. This kind of stick is available in stores that feature Asian products, where it is sold with a product used by Asian women to temporarily create an upper eyelid crease. To induce a crease and temporarily reposition the lower eyelid after the application of the liquid bandage, blunt-tipped tweezers may be used instead of the 'Y-shaped' stick.
After application, the liquid bandage was capable of providing a suitable eyelid position for approximately 3 days, but if necessary, it could be removed at any time with mineral oil, followed by washing the region with soap and water. Patients were directed to re-apply the product in case of adhesion breakage.
During the treatment period, patients were evaluated at days 1, 7 and 15. They were questioned about ocular comfort and were examined at the slit lamp for: eyelid position (in primary position of gaze and after forced closure of the eyes); lower eyelid skin aspect (to verify if the patient did not present any kind of allergic reaction), and corneal keratopathy, using fluorescein drops. Photographs of the patients (Sony Cyber-shot DSC-TX1/H digital camera) were taken in primary position of gaze and after forced closure of the eyes before and after treatment. One of the authors (MHO) evaluated all the patients during the studied period and was also responsible for taking the photographs. Patients were advised to return at any time between the scheduled visits if they experienced any kind of local cutaneous irritation.
RESULTS
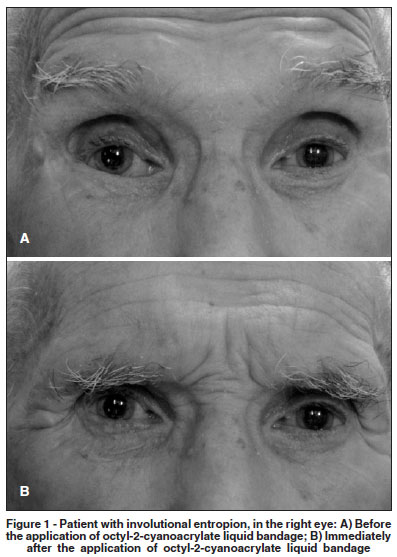
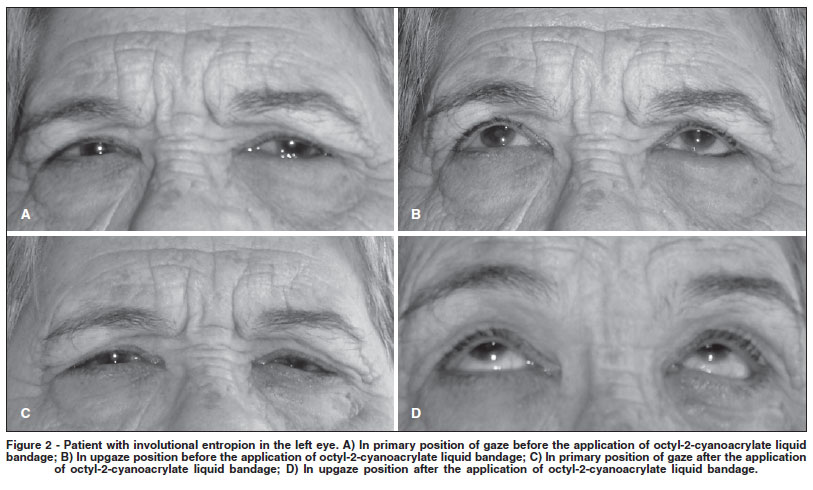
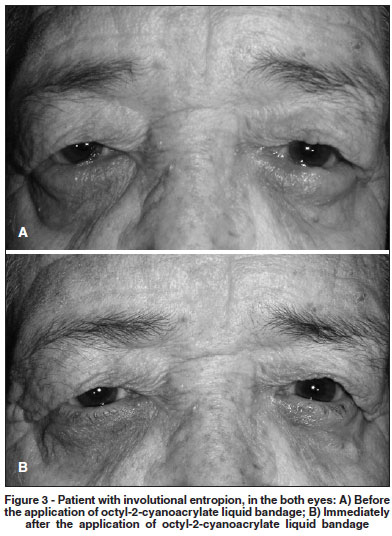
All patients presented successful correction at day 1 and reported significant improvements in signs and symptoms (Figures 1, 2 and 3). One patient reported early adhesion breakage (in the second day), probably due to excessive manipulation of the lower eyelid region. All patients returned in the scheduled dates and the average duration of action of the octyl-2-cyanoacrylate liquid bandage reported by the patients was 3.1 ± 0.9 (range: 2 to 5) days. No ocular or dermatological reactions were noted and the patients were satisfied with the temporary results. No patient reported ocular discomfort or lagophthalmos after the product application.
DISCUSSION
Involutional entropion affects elderly patients preferentially, who often experience many medical and social problems(9). Therefore, until these patients are clinically stabilized such that they are able to undergo a surgical procedure, the application of octyl-2-cyanoacrylate liquid bandage offers temporary correction of eyelid position and relief of symptoms.
In addition, for some patients, surgery is contraindicated if they do not present the required clinical conditions to be subjected to a surgical procedure (patients who cannot stop anticoagulation therapy, for example). In these cases, the application of the liquid bandage is also a good option for treatment.
Quickert everting sutures, which plicate the attenuated lid retractors and transfer their pull to the anterior surface of the tarsal plate, are also an alternative for debilitated patients(16-18). Although it is a simple procedure, it is not as easy as the application of the liquid bandage and requires hospitalization to be performed.
Taping using adhesive tapes (MicroporeTM) and its modification associated with instillation of lubricants have been the traditional management for the intervening period. However, it is neither cosmetically acceptable nor gives constant and reproducible results. Allergic reactions to the material and corneal abrasions secondary to corneal irritation from the edge of the patch limit its use(19-20).
Some authors evaluated the use of botulinum toxin as a temporary treatment in patients awaiting surgical repair for involutional entropion and observed improvements in signs and symptoms(21). However, the botulinum toxin is an expensive product and its application has to be performed by an ophthalmologist, as opposed to the liquid bandage, which application can be performed by any person.
The use of a cyanoacrylate glue using a blunt 20-G cannula to temporarily manage involutional entropion was described. However, the kind of cyanoacrylate is not described and the technique described to apply the product requires a physician or at least a technician, as opposed to the liquid bandage(20).
Octyl-2-cyanoacrylate liquid bandage has the advantage that it can be applied by the patient him/herself or by the person who takes care of him/her (in case of debilitated patients) and is a very simple procedure. They only have to be warned not to get glue in the eye or on the eyelash. In addition, it not only restores normal lid function, but also provides an excellent cosmetic outcome with practically no complications, as the product is hypoallergenic. Also, if necessary, it can be easily removed at any time with mineral oil.
CONCLUSIONS
Octyl-2-cyanoacrylate showed promising results as an innovative, easy-to-apply and effective alternative to temporarily treat involutional entropion patients, while they are waiting for definitive surgical repair (sometimes it may take up to weeks). It is a safe, non-allergenic and economic product that can be recommended to these patients.
REFERENCES
1. Erb MH, Uzcategui N, Dresner S. Efficacy and complications of the transconjunctival entropion repair for lower eyelid involutional entropion. Ophthalmology. 2006;113(12):2351-6.
2. Altieri M, Iester M, Harman F, Bertagno R, Capris P, Venzano D, et al. Comparison of three techniques for repair of involutional lower lid entropion: a three year follow-up study. Ophthalmologica. 2003;217(4):265-72. Comment in: Ophthalmologica. 2004;218(3):219; author reply 220.
3. Rougraff PM, Tse DT, Johnson TE, Feuer W. Involutional entropion repair with fornix sutures and lateral tarsal strip procedure. Ophthal Plast Reconstr Surg. 2001;17(4):281-7.
4. Kakizaki H, Zako M, Kinoshita S, Iwaki M. Posterior layer advancement of the lower eyelid retractor in involutional entropion repair. Ophthal Plast Reconstr Surg. 2007;23(4):292-5.
5. Bashour M, Harvey J. Causes of involutional ectropion and entropion-age-related tarsal changes are the key. Ophthal Plast Reconstr Surg. 2000;16(2):131-41.
6. Jones LT, Reeh MJ, Wobig JL. Senile entropion. A new concept for correction. Am J Ophthalmol. 1972;74(2):327-9.
7. Jordan DR, Anderson RL. The lateral tarsal strip revisited. The enhanced tarsal strip. Arch Ophthalmol. 1989;107(4):604-6.
8. Skorin L Jr. A review of entropion and its management. Cont Lens Anterior Eye. 2003;26(2):95-100.
9. Olver JM, Barnes JA. Effective small-incision surgery for involutional lower eyelid entropion. Ophthalmology. 2000;107(11):1982-8.
10. Handschel JG, Depprich RA, Dirksen D, Runte C, Zimmermann A, Kübler NR. A prospective comparison of octyl-2-cyanoacrylate and suture in standardized facial wounds. Int J Oral Maxillofac Surg. 2006;35(4):318-23.
11. Meskin SW, Ritterband DC, Shapiro DE, Kusmierczyk J, Schneider SS, Seedor JA, Koplin RS. Liquid bandage (2-octyl cyanoacrylate) as a temporary wound barrier in clear corneal cataract surgery. Ophthalmology. 2005;112(11):2015-21.
12. Shepler TR, Seiff SR. Use of isobutyl cyanoacrylate tissue adhesive to stabilize external eyelid weights in temporary treatment of facial palsies. Ophthal Plast Reconstr Surg. 2001;17(3):169-73.
13. Taravella MJ, Chang CD. 2-Octyl cyanoacrylate medical adhesive in the treatment of a corneal perforation. Cornea. 2001;20(2):220-1.
14. Suhr MA, Günther M, Springer IN. Ptosis relief after botox injection using dermabond. Plast Reconstr Surg. 2004;114(1):262-3.
15. Osaki TH, Osaki MH, Belfort R Jr, Osaki T, Sant'Anna AE, Haraguchi DK. Management of progressive myopathic blepharoptosis with daily application of octyl-2-cyanoacrylate liquid bandage. Ophthal Plast Reconstr Surg. 2009; 25(4):264-6.
16. Quickert MH, Rathbun E. Suture repair of entropion. Arch Ophthalmol. 1971;85(3):304-5.
17. Wright M, Bell D, Scott C, Leatherbarrow B. Everting suture correction of lower lid involutional entropion. Br J Ophthalmol. 1999;83(9):1060-3.
18. Meadows AE, Reck AC, Gaston H, Tyers AG. Everting sutures in involutional entropion. Orbit. 1999;18(3):177-81.
19. Irvine S, Francis IC, Bishop AE, Baxter J. The entropion patch: a method of temporarily correcting involutional entropion with adhesive tape. Ophthalmic treatment of involutional lower lid entropion: a clinical and morphological study. Surg. 1994;25(9):604-6.
20. Puri P. Tissue glue aided lid repositioning in temporary management of involutional entropion. Eur J Ophthalmol. 2001;11(3):211-4.
21. Steel DH, Hoh HB, Harrad RA, Collins CR. Botulinum toxin for the temporary Eye (Lond). 1997;11(Pt 4):472-5.
 Correspondence address:
Correspondence address:
Teissy Osaki
R. Vergueiro, 2.045 - Cj. 1.009 - São Paulo (SP)
CEP 04101-000
Email: [email protected]
Recebido para publicação em 08.09.2009
Última versão recebida em 14.03.2010
Aprovação em 15.03.2010
Work carried out at the Ophthalmology Department of the Federal University of São Paulo - UNIFESP.
© 2024 - All rights reserved - Conselho Brasileiro de Oftalmologia
![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Scielo
Scielo
 Pocket
Pocket

{kind=link}
{kind=link}