Arq. Bras. Oftalmol. 2022;85 (6 )
:565-571
| DOI: 10.5935/0004-2749.20220059
Abstract
Objetivo: Avaliar o curso clínico e o manejo da ceratite infecciosa de interface após ceratoplastia endotelial da membrana de Descemet.
Métodos: Um total de 352 casos submetidos a ceratoplastia endotelial da membrana de Descemet foram revisados retrospectivamente. Pacientes com ceratite infecciosa de interface foram analisados durante o acompanhamento. As análises microbiológicas, o tempo até o início da infecção, os achados clínicos, a duração do acompanhamento, o tratamento e a acuidade visual para longe corrigida pós-tratamento foram registrados.
Resultados: Ceratite infecciosa de interface foi detectada em 8 olhos de 8 casos. Três patógenos fúngicos e três bacterianos foram identificados em todos os casos e receberam tratamento médico de acordo com a sensibilidade da cultura. O tratamento antifúngico foi iniciado em dois casos sem crescimento em cultura, com diagnóstico preliminar de ceratite infecciosa fúngica. Injeções antifúngicas intraestromais foram usadas em todos os casos com infecções fúngicas. O tempo médio para o início da infecção foi de 164 dias (variação: 2-282 dias). A ceratite infecciosa de interface pós-operatória desenvolveu-se no período inicial em dois casos. A duração média do acompanhamento foi de 13,4 ± 6,2 meses (variação: 6-26 meses). A ceratoplastia endotelial de membrana de Descemet foi realizada em dois casos (25%) e ceratoplastia penetrante terapêutica em quatro casos (50%) que não se recuperaram com tratamento médico. A acuidade visual para longe corrigida final foi de 20/40 ou melhor em 5/8 (62,5%) dos pacientes.
Conclusões: O diagnóstico e o tratamento da ceratite infecciosa de interface após ceratoplastia endotelial da membrana de Descemet são difíceis. A intervenção cirúrgica precoce deve ser o procedimento preferido se não houver resposta ao tratamento médico. Melhor sobrevida do enxerto e melhor acuidade visual podem ser alcançadas com ceratoplastia penetrante terapêutica e ceratoplastia endotelial da membrana de Descemet em pacientes com ceratite infecciosa de interface
Keywords: Transplante de Córnea; Lâmina limitante posterior; Sobrevivência de enxerto; Infecções; Injeções; Ceratite; Ceratoplastia penetrante; Acuidade visual
Arq. Bras. Oftalmol. 2021;84 (3 )
:230-234
| DOI: 10.5935/0004-2749.20210037
Abstract
OBJETIVO: Investigar o efeito do uso de uma substância viscoelástica na ruptura da membrana de Descemet em casos de ceratoplastia lamelar anterior profunda em “bolha dupla”.
MÉTODOS: Foram avaliados retrospectivamente prontuários e vídeos de cirurgias de 40 pacientes operados entre janeiro de 2014 e julho de 2015. Os pacientes foram divididos em dois grupos: 20 pacientes nos quais a parede posterior do estroma foi puncionada sem a colocação de nenhuma substância viscoelástica (grupo 1) e 20 pacientes nos quais uma substância viscoelástica foi aplicada sobre o estroma posterior ao ser puncionada a parede posterior do estroma (grupo 2). A taxa de perfuração da membrana de Descemet foi comparada entre os grupos.
RESULTADOS: Observou-se perfuração da membrana de Descemet em 12 casos (60,0%) no grupo 1 e em apenas 3 casos (15,0%) no grupo 2. Essa diferença foi estatisticamente significativa (p=0,003). Apenas um caso (5%) no grupo 2 teve macroperfuração durante o procedimento, sendo a cirurgia então convertida em uma ceratoplastia penetrante. Onze casos (55,0%) no grupo 1 tiveram macroperfuração da membrana de Descemet e essas cirurgias foram convertidas em ceratoplastias penetrantes. Essa diferença entre os grupos foi estatisticamente significativa (p=0,001).
CONCLUSÕES: A aplicação de substância viscoelástica sobre o lado posterior do estroma logo antes da punção é um método eficaz para diminuir o risco de perfuração da membrana de Descemet na ceratoplastia lamelar anterior profunda.
Keywords: Lâmina limitante posterior/cirurgia; Substâncias viscoelásticas; Transplante de córnea; Substância propria; Ceratoplastia penetrante
Arq. Bras. Oftalmol. 2025;88 (6 )
:1-7
| DOI: 10.5935/0004-2749.2025-0120
Abstract
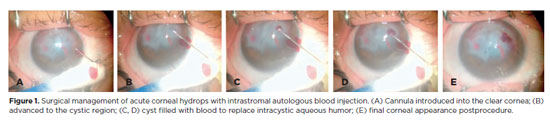
PURPOSE: To describe the technique and outcomes of intrastromal autologous blood injection in patients with severe corneal hydrops.
METHODS: Nineteen patients with corneal hydrops underwent intrastromal autologous blood injection. Postoperative assessments included best-corrected visual acuity and time to resolution of corneal edema
RESULTS: Corneal edema resolved within 1 week in 5 patients, within 1 month in 11, and within 3 months in 3. The mean duration of edema persistence was 37.94 ± 33.05 days (range, 6–124). Corneal thickness decreased from 2.06 ± 0.71-mm preoperatively to 1.34 ± 0.65-mm at day 7, 0.85 ± 0.56-mm at day 30, and 0.57 ± 0.13-mm at day 90 (p<0.001). Descemet’s membrane (DM) detachment decreased from 1.01 ± 0.75-mm to 0.44 ± 0.57-mm, 0.24 ± 0.36-mm, and 0.08 ± 0.11-mm on postoperative days 7, 30, and 90, respectively (p<0.001). DM break size decreased from 1.12 ± 1.19-mm to 0.62 ± 0.84-mm at 3 months (p<0.005). Three patients developed hematocornea; no other major complications were observed. At 3 months, mean best-corrected visual acuity improved from 2.37 ± 0.66 to 0.41 ± 0.17 logMAR with hard contact lenses (p<0.001).
CONCLUSIONS: Intrastromal autologous blood injection is an effective treatment for severe corneal hydrops, promoting faster edema resolution and visual improvement with minimal complications.
Keywords: Corneal edema; Corneal diseases; Edema; Visual acuity; keratoconus.
Arq. Bras. Oftalmol. 2026;89 (4 )
:1-9
| DOI: 10.5935/0004-2749.2025-0034
Abstract
PURPOSE: To evaluate the impact of the COVID-19 pandemic and characterize the serological profile of discarded corneal donations in the coverage area of the Banco de Olhos de Londrina, through reverse transcription-polymerase chain reaction testing for COVID-19 and serological screening of cornea donors excluded because of positive test results.
METHODS: This observational retrospective study included 776 cornea donors who’s serological and reverse transcription-polymerase chain reaction test results were processed at the Hospital of Universidade Estadual de Londrina between May 2020 and 2022. The number of corneal donations and tissue utilization rates throughout the years of operation of the Banco de Olhos de Londrina were also analyzed.
RESULTS: The mean donor age was 53.14 years; 332 donors (43%) were female, and 444 (57%) were male. Positive results were identified in 15.76% of donors for hepatitis B core antibody antibodies, 0.65% for hepatitis B surface antigen, 1.03% for hepatitis C antibodies, and 0.52% for human immunodeficiency virus and human T-lymphotropic vírus. Positive reverse transcription-polymerase chain reaction results for SARS-CoV-2 were observed in 2.7% of cases. Older adults were 2.6 times more likely to test positive for SARS-CoV-2 (95% CI, 1.06-6.34) and 3.0 times more likely to test positive for hepatitis B core antibody (95% CI, 1.95-4.41) than younger individuals. A 75.2% reduction in corneal donations was observed in 2020 compared with 2019, accompanied by a 5% increase in tissue utilization, possibly associated with the effectiveness of donor screening during the pandemic.
CONCLUSION: The COVID-19 pandemic had a profound impact on the number of corneal transplants worldwide, in Brazil, and at the Banco de Olhos de Londrina because of the substantial decline in donations during this period. Hepatitis B was the leading cause of corneal tissue discard due to positive serology in both this study and previous reports, highlighting the importance of prevention programs and improved vaccination coverage. Strict legislation, comprehensive serological screening, and appropriate processing of donated tissue remain essential to eliminate potential sources of infection and ensure transplantation safety.
Keywords: Cornea; Corneal transplantation; COVID-19; Eye banks; Serology
Arq. Bras. Oftalmol. 2025;88 (3 )
:1-7
| DOI: 10.5935/0004-2749.2023-0309
Abstract
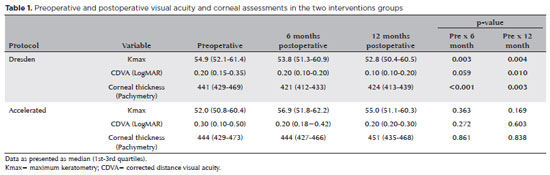
PURPOSE: Keratoconus presents certain peculiarities in pediatric patients when compared with adults. The greatest challenge in children is that the disease is more severe and faster in progression. In this retrospective study, we aimed to compare the accelerated and Dresden protocols for corneal crosslinking in patients aged <18 years who were followed-up for at least 12 months.
METHODS: A total of 36 eyes from 27 patients were included in the study. The best corrected and uncorrected visual acuity, maximal keratometry, corneal thickness, foveal thickness, and endothelial microscopy findings were evaluated at baseline and during the postoperative period at one, three, and six months. Thereafter, the patients were evaluated at one, three, six and twelve months postoperative. Corneal crosslinking was performed in all patients via the Dresden protocol (n=21 eyes) or the accelerated protocol (n=15 eyes). Data between the two groups were compared and XY statistical analysis was used.
RESULTS: Both protocols were effective in halting keratoconus progression. No patient had progression at the 12-month follow-up. A significant reduction in Kmax and improvement in the corrected distance visual acuity were observed only in the Dresden protocol group. Although the Dresden protocol was superior to the accelerated protocol in reducing Kmax (p=0.002), there was no significant difference in corrected distance visual acuity between the two groups.
CONCLUSION: The accelerated protocol is as efficient as the Dresden protocol in stabilizing keratoconus progression. Although the Dresden protocol was superior to the accelerated protocol in reducing the Kmax, it did not produce better clinical results. Thus, the accelerated protocol is an efficient option. Furthermore, considering the advantages of reduced surgical time, the accelerated protocol is effective in halting keratoconus progression in the pediatric age group.
Keywords: Keratoconus; Corneal diseases; Ultraviolet rays; Cross-linking reagents; Visual acuity
Arq. Bras. Oftalmol. 2024;87 (4 )
:1-6
| DOI: 10.5935/0004-2749.2022-0128
Abstract
Objetivo: Relatar um experimento projetado para determinar alterações anatômicas em córneas porcinas após a colocação de um novo implante depolímero na córnea.
Métodos: Foi utilizado olho de porco ex vivo. Um novo agente modelador biocompatível, de colágeno tipo 1, com 6mm de diâmetro foi moldado com excimer laser em sua face posterior, para criar três formatos planocôncavos. Os implantes foram inseridos dentro de um bolsão, dissecado manualmente, a 200 micrômetros (µm). Foram definidos três grupos de tratamento: grupo A (n=3), teve a profundidade máxima de ablação de70 µm; o grupo B (n=3), profundidade máxima de ablação de 64 µm; e o grupo C (n=3), profundidade máxima de ablação de 104 µm, com buraco central. O grupo controle, D (n=3), foi incluído, com a criação do bolsão estromal, porém sem inserir o material. A avaliação desses olhos foi realizada por tomografia de coerência óptica (OCT) e por tomografia corneana.
Resultados: A tomografia corneana mostrou uma tendência para diminuição da ceratometria média em todos os 4 grupos. A tomografia de coerência óptica mostrou córneas com implantes localizados no estroma anterior e aplanamento visível, enquanto as córneas não mudaram qualitativamente o formato no grupo controle.
Conclusões: O novo implante de biomaterial planocôncavo descrito aqui foi capaz de remodelar a córnea em modelo de animal ex vivo, resultando no aplanamento corneano. Novos estudos são necessários usando modelos animais in vivo para confirmar tais achados.
Keywords: Córnea; Cirurgia da córnea a laser; Substância própria; Proteses e implantes; Lasers de excimer; Materiais biocompatíveis; Animais; Suínos
Arq. Bras. Oftalmol. 2024;87 (3 )
:1-7
| DOI: 10.5935/0004-2749.2023-0049
Abstract
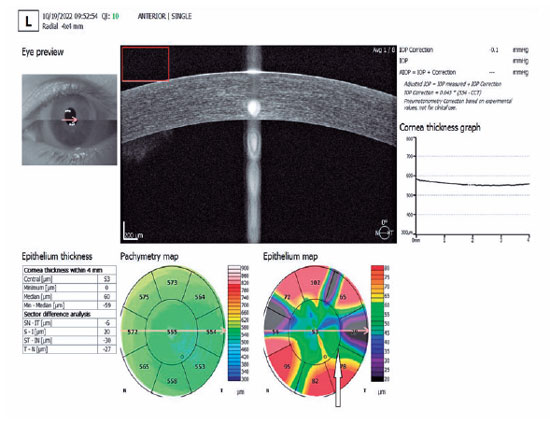
PURPOSE: To investigate the association of pre-photorefractive keratectomy Schirmer-1 test value with post-photorefractive keratectomy central corneal epithelial thickness, ocular surface disease index score, and uncorrected distance visual acuity.
METHODS: Patients were categorized according to preoperative Schirmer-1 value: the normal Schirmer Group (n=54; Schirmer-1 test value, >10 mm) and the low Schirmer Group (n=52; Schirmer-1 test value, between 6 and 10 mm). We analyzed ablation depth, visual acuity, result of Schirmer-1 test (with anesthesia), tear film break-up time, ocular surface disease index score, central corneal epithelial thickness, and spherical equivalent refraction.
RESULTS: We found significant differences between the groups in Schirmer-1 test value, tear film break-up time, and ocular surface disease index score, both preoperatively and postoperatively (p<0.001). The preoperative central corneal epithelial thicknesses of the two groups were similar (p>0.05). After photorefractive keratectomy, the Schirmer-1 test value and spherical equivalent refraction decreased in both groups (p<0.05), and ocular surface disease index scores and central corneal epithelial thickness values increased in the low Schirmer Group (p<0.001) but not in the normal Schirmer Group (p>0.05). The postoperative central corneal epithelial thicknesses of the low Schirmer Group were significantly higher than those of the normal Schirmer Group (p<0.001). Postoperative uncorrected distance visual acuity did not differ significantly between the two groups (p>0.05).
CONCLUSIONS: In patients with low Schirmer-1 test values before photorefractive keratectomy, the corneal epithelium thickened and ocular surface complaints increased during the postoperative period. However, changes in the corneal epithelium did not affect the postoperative uncorrected distance visual acuity. To reduce postoperative problems on the ocular surface in these patients, we recommend that dry eye be treated before photorefractive keratectomy.
Keywords: Epithelium, corneal; Cornea; Photorefractive keratectomy; Schirmer test; Visual acuity
Arq. Bras. Oftalmol. 2024;87 (3 )
:1-8
| DOI: 10.5935/0004-2749.2023-0109
Abstract
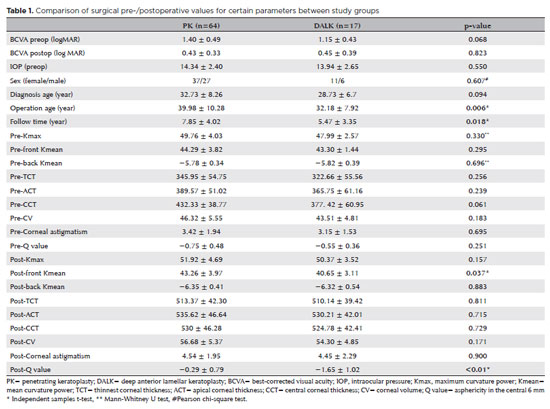
PURPOSES: This study aims to assess and compare the postoperative visual and topographic outcomes, complications, and graft survival rates following deep anterior lamellar keratoplasty and penetrating keratoplasty in patients with macular corneal dystrophy.
METHODS: In this study we enrolled 59 patients (23 male; and 36 female) with macular corneal dystrophy comprising 81 eyes. Out of these, 64 eyes underwent penetrating keratoplasty, while 17 eyes underwent deep anterior lamellar keratoplasty. The two groups were analyzed and compared based on best-corrected visual acuity, corneal tomography parameters, pachymetry, complication rates, and graft survival rates.
RESULTS: After 12 months, 70.6% of the patients who underwent deep anterior lamellar keratoplasty (DALK) and 75% of those who had penetrating keratoplasty (PK) achieved a best-corrected visual acuity of 20/40 or better (p=0.712). Following surgery, DALK group showed lower front Kmean (p=0.037), and Q values (p<0.01) compared to the PK group. Postoperative interface opacity was observed in seven eyes (41.2%) in the DALK group. Other topography values and other complications (graft rejection, graft failure, cataract, glaucoma, microbial keratitis, optic atrophy) did not show significant differences between the two groups. The need for regrafting was 9.4% and 11.8% in the PK and DALK groups, respectively (p=0.769). Graft survival rates were 87.5% and 88.2% for PK and DALK; respectively (p=0.88 by Log-rank test).
CONCLUSION: Both PK and DALK are equally effective in treating macular corneal dystrophy, showing similar visual, topographic, and survival outcomes. Although interface opacity occurs more frequently after DALK the visual results were comparable in both groups. Therefore, DALK emerges as a viable surgical choice for patients with macular corneal dystrophy without Descemet membrane involvement is absent.
Keywords: Macular corneal dystrophy; Corneal dystrophies; Hereditary; Keratoplasty; Penetrating; Corneal transplantation
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
02-tab01tb.jpg)
06-fig01.jpg)

09-fig01.jpg)
02-fig01.jpg)
08-fig01.jpg)
01-fig01.jpg)
09-fig01.jpg)