Arq. Bras. Oftalmol. 2022;85 (4 )
:370-376
| DOI: 10.5935/0004-2749.20220032
Abstract
Objetivos: Investigar a incidência, fatores de risco e desfechos visuais do desenvolvimento da membrana epirretiniana após reparo do descolamento regmatogênico da retina.
Métodos: Trata-se de um estudo retrospectivo de 309 olhos submetidos à cirurgia inicial para descolamento regmatogênico da retina primário sem complicações. Os exames foram realizados no pré-operatório aos 1, 3, 6 e 12 meses pós-operatórios. Os pacientes foram divididos em dois grupos, dependendo da presença ou ausência de membrana epirretiniana.
Resultados: A incidência de membrana epirretiniana pós-operatória foi de 28,5%; 42,7% desses pacientes apresentaram desenvolvimento grave da membrana epirretiniana e, portanto, foram submetidos à remoção desta membrana. A regressão logística mostrou que as lágrimas retinianas gigantes (RC: 2,66; 95% IC: 1,045 - 6,792, p=0,040) e lágrimas em ferradura (RC: 0,534; 95% IC: 0,295-0,967, p=0,039), foram preditores significativos de membrana epirretiniana pós-operatória. A coloração com acetonida de triancinolona foi significativamente associada à prevenção da membrana epirretiniana (p=0,022). Trinta e quatro pacientes apresentaram acuidade visual melhorada, ou igual, ou acuidade visual final melhor corrigida; 4 olhos foram avaliados na consulta final de acompanhamento e apresentaram redução da acuidade visual melhor corrigida.
Conclusão: Nossa análise demonstra que as lágrimas de ferradura e as lágrimas retinianas gigantes representam fatores de risco para a membrana epirretiniana pós-operatória. A coloração com acetonida de triancinolona teve um efeito preventivo significativo na membrana epirretiniana no pós-operatório. Além disso, uma segunda rodada de vitrectomia pars plana, incluindo remoção da membrana, levou a uma melhora significativa da acuidade visual final melhor corrigida na última consulta de acompanhamento, embora a recuperação tenha sido limitada.
Keywords: Membrana epirretiniana; Descolamento da retina; Recurvamento da esclera; Acuidade visual; Vitrectomia
Arq. Bras. Oftalmol. 2025;88 (2 )
:1-9
| DOI: 10.5935/0004-2749.2023-0326
Abstract
PURPOSE: To evaluate the predictive value of initial intraocular pressure difference of the detached and fellow eyes of patients with complex rhegmatogenous retinal detachment on postoperative persistent ocular hypotony.
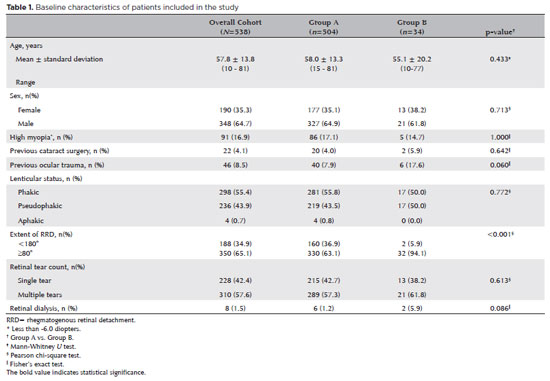
METHODS: This retrospective observational study included 538 eyes of 538 unilateral complex rhegmatogenous retinal detachment patients with a proliferative vitreoretinopathy grade of C-1 or higher, treated with silicone oil endotamponade following pars plana vitrectomy. The patients were divided into Group A (patients having silicone oil removal without ocular hypotony; n=504) and Group B (patients with persistent ocular hypotony following silicone oil removal [n=8, 23.5%] and with retained silicone oil [n=26, 76.5%] due to the risk of persistent ocular hypotony; total n=34). Ocular hypotony was defined as an intraocular pressure of <6 mmHg on two or more occasions. Patients' demographics, including age, sex, and follow-up time, and ocular characteristics, including ocular surgical and trauma history, initial and final best-corrected visual acuity, intraocular pressure and initial intraocular pressure difference of the detached and fellow eyes, and anatomical success rates and postoperative complications, were retrospectively collected from the electronic patient files.
RESULTS: The initial intraocular pressure was significantly lower in the detached eyes of Group B than in Group A (8.3 ± 3.5 vs. 12.9 ± 3.3, p<0.001). Also, the initial intraocular pressure difference was significantly higher in Group B than in Group A (8.9 ± 3.2 vs. 2.2 ± 2.7mmHg, p<0.001). The receiver operating characteristic curve analysis showed that the cutoff value of the initial intraocular pressure difference was 7.5mmHg for the risk of persistent ocular hypotony. The most influential factors on postoperative persistent ocular hypotony in the binary logistic regression analysis were the initial intraocular pressure difference and the need for a retinectomy.
CONCLUSION: In eyes with complex rhegmatogenous retinal detachment treated with pars plana vitrectomy and silicone oil tamponade, the initial intraocular pressure difference could be of value in predicting postoperative persistent ocular hypotony and could guide surgeons on the decision of silicone oil removal.
Keywords: Hypotony; Intraocular pressure; Pars plana vitrectomy; Retinal detachment; Silicone oils; Ocular hypotension; Visual acuity
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
03-tab01tb.jpg)
02-fig01.jpg)
02-fig01.jpg)
03-fig01.jpg)
05-fig01.jpg)
02-fig01.jpg)
02-fig01.jpg)
13-fig01.jpg)
04-fig01.jpg)
12-fig01.jpg)
03-fig01.jpg)