Arq. Bras. Oftalmol. 2022;85 (6 )
:565-571
| DOI: 10.5935/0004-2749.20220059
Abstract
Objetivo: Avaliar o curso clínico e o manejo da ceratite infecciosa de interface após ceratoplastia endotelial da membrana de Descemet.
Métodos: Um total de 352 casos submetidos a ceratoplastia endotelial da membrana de Descemet foram revisados retrospectivamente. Pacientes com ceratite infecciosa de interface foram analisados durante o acompanhamento. As análises microbiológicas, o tempo até o início da infecção, os achados clínicos, a duração do acompanhamento, o tratamento e a acuidade visual para longe corrigida pós-tratamento foram registrados.
Resultados: Ceratite infecciosa de interface foi detectada em 8 olhos de 8 casos. Três patógenos fúngicos e três bacterianos foram identificados em todos os casos e receberam tratamento médico de acordo com a sensibilidade da cultura. O tratamento antifúngico foi iniciado em dois casos sem crescimento em cultura, com diagnóstico preliminar de ceratite infecciosa fúngica. Injeções antifúngicas intraestromais foram usadas em todos os casos com infecções fúngicas. O tempo médio para o início da infecção foi de 164 dias (variação: 2-282 dias). A ceratite infecciosa de interface pós-operatória desenvolveu-se no período inicial em dois casos. A duração média do acompanhamento foi de 13,4 ± 6,2 meses (variação: 6-26 meses). A ceratoplastia endotelial de membrana de Descemet foi realizada em dois casos (25%) e ceratoplastia penetrante terapêutica em quatro casos (50%) que não se recuperaram com tratamento médico. A acuidade visual para longe corrigida final foi de 20/40 ou melhor em 5/8 (62,5%) dos pacientes.
Conclusões: O diagnóstico e o tratamento da ceratite infecciosa de interface após ceratoplastia endotelial da membrana de Descemet são difíceis. A intervenção cirúrgica precoce deve ser o procedimento preferido se não houver resposta ao tratamento médico. Melhor sobrevida do enxerto e melhor acuidade visual podem ser alcançadas com ceratoplastia penetrante terapêutica e ceratoplastia endotelial da membrana de Descemet em pacientes com ceratite infecciosa de interface
Keywords: Transplante de Córnea; Lâmina limitante posterior; Sobrevivência de enxerto; Infecções; Injeções; Ceratite; Ceratoplastia penetrante; Acuidade visual
Arq. Bras. Oftalmol. 2025;88 (6 )
:1-5
| DOI: 10.5935/0004-2749.2024-0321
Abstract
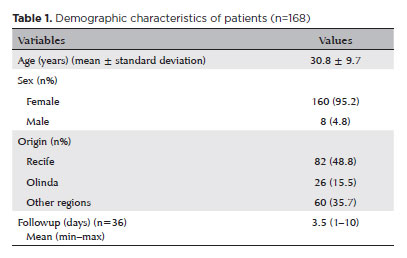
PURPOSE: To report the ophthalmological signs, symptoms, and clinical management observed during an unprecedented outbreak of chemical ocular injuries related to cosmetic hair ointments in Brazil.
METHODS: This descriptive, cross-sectional study reviewed medical records of patients treated at the emergency center of Fundação Altino Ventura for chemical ocular trauma associated with cosmetic hair ointment use between February 2022 and February 2023. Records with incomplete medical information were excluded.
RESULTS: The study included 168 patients (95.2% [n=160] female), with a mean age of 30.8 ± 9.7 years. The most frequently reported symptoms at presentation were pain (167/168, 99.4%) and photophobia (92/168, 54.8%). Severe pain was reported by 137 patients (80%). Keratitis was present in 280 of 336 eyes (83.3%), conjunctival hyperemia in 256 eyes (76.4%), and corneal abrasions in 174 eyes (51.8%). A decrease in visual acuity (worse than 20/25) was documented in 18.5% (31/168) of cases. Lubricants, antibiotics, and re-epithelialization
ointments were prescribed to 64.8% (109/168) of the patients. Topical corticosteroids and oral vitamin C were administered to 34% (57/168) and 1.2% (2/168) of patients, respectively. Followup visits were required in 19% (33/168) of cases.
CONCLUSION: The outbreak of chemical ocular injuries linked to cosmetic ointments used for braiding and hair modeling in Brazil was marked by intense ocular pain, conjunctival hyperemia, keratitis, and corneal abrasions. Most patients were treated with lubricants, antibiotics, and re-epithelialization ointments, although approximately one-fifth required followup care, and one-third received additional treatment with either topical corticosteroids and/or oral vitamin C.
Keywords: Cosmetics; Hair preparations; Eye injuries; Burns, chemical; Eye burns; Keratitis; Cornea; Corneal diseases; Visual low.
Arq. Bras. Oftalmol. 2025;88 (6 )
:1-7
| DOI: 10.5935/0004-2749.2025-0120
Abstract
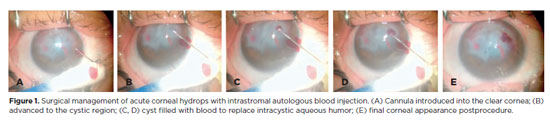
PURPOSE: To describe the technique and outcomes of intrastromal autologous blood injection in patients with severe corneal hydrops.
METHODS: Nineteen patients with corneal hydrops underwent intrastromal autologous blood injection. Postoperative assessments included best-corrected visual acuity and time to resolution of corneal edema
RESULTS: Corneal edema resolved within 1 week in 5 patients, within 1 month in 11, and within 3 months in 3. The mean duration of edema persistence was 37.94 ± 33.05 days (range, 6–124). Corneal thickness decreased from 2.06 ± 0.71-mm preoperatively to 1.34 ± 0.65-mm at day 7, 0.85 ± 0.56-mm at day 30, and 0.57 ± 0.13-mm at day 90 (p<0.001). Descemet’s membrane (DM) detachment decreased from 1.01 ± 0.75-mm to 0.44 ± 0.57-mm, 0.24 ± 0.36-mm, and 0.08 ± 0.11-mm on postoperative days 7, 30, and 90, respectively (p<0.001). DM break size decreased from 1.12 ± 1.19-mm to 0.62 ± 0.84-mm at 3 months (p<0.005). Three patients developed hematocornea; no other major complications were observed. At 3 months, mean best-corrected visual acuity improved from 2.37 ± 0.66 to 0.41 ± 0.17 logMAR with hard contact lenses (p<0.001).
CONCLUSIONS: Intrastromal autologous blood injection is an effective treatment for severe corneal hydrops, promoting faster edema resolution and visual improvement with minimal complications.
Keywords: Corneal edema; Corneal diseases; Edema; Visual acuity; keratoconus.
Arq. Bras. Oftalmol. 2025;88 (3 )
:1-7
| DOI: 10.5935/0004-2749.2023-0309
Abstract
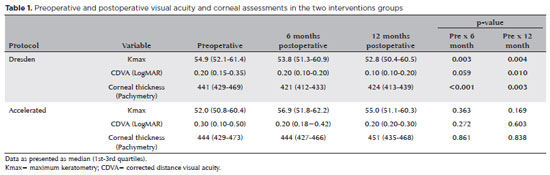
PURPOSE: Keratoconus presents certain peculiarities in pediatric patients when compared with adults. The greatest challenge in children is that the disease is more severe and faster in progression. In this retrospective study, we aimed to compare the accelerated and Dresden protocols for corneal crosslinking in patients aged <18 years who were followed-up for at least 12 months.
METHODS: A total of 36 eyes from 27 patients were included in the study. The best corrected and uncorrected visual acuity, maximal keratometry, corneal thickness, foveal thickness, and endothelial microscopy findings were evaluated at baseline and during the postoperative period at one, three, and six months. Thereafter, the patients were evaluated at one, three, six and twelve months postoperative. Corneal crosslinking was performed in all patients via the Dresden protocol (n=21 eyes) or the accelerated protocol (n=15 eyes). Data between the two groups were compared and XY statistical analysis was used.
RESULTS: Both protocols were effective in halting keratoconus progression. No patient had progression at the 12-month follow-up. A significant reduction in Kmax and improvement in the corrected distance visual acuity were observed only in the Dresden protocol group. Although the Dresden protocol was superior to the accelerated protocol in reducing Kmax (p=0.002), there was no significant difference in corrected distance visual acuity between the two groups.
CONCLUSION: The accelerated protocol is as efficient as the Dresden protocol in stabilizing keratoconus progression. Although the Dresden protocol was superior to the accelerated protocol in reducing the Kmax, it did not produce better clinical results. Thus, the accelerated protocol is an efficient option. Furthermore, considering the advantages of reduced surgical time, the accelerated protocol is effective in halting keratoconus progression in the pediatric age group.
Keywords: Keratoconus; Corneal diseases; Ultraviolet rays; Cross-linking reagents; Visual acuity
Arq. Bras. Oftalmol. 2025;88 (5 )
:1-7
| DOI: 10.5935/0004-2749.2024-0368
Abstract
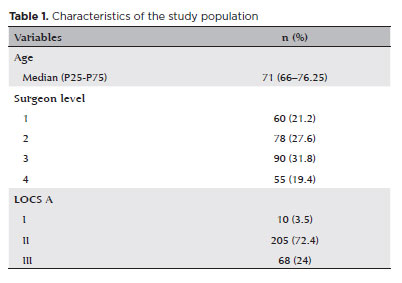
PURPOSE: To compare endothelial corneal cell changes following cataract surgery performed by phacoemulsification with intraocular lens implantation, conducted by surgeons with varying levels of experience.
METHODS: Two hundred and eighty-three eyes diagnosed with cataract were included. Lens opacity was classified into three categories (I, II, and III). Surgeons were categorized into four experience levels (1, 2, 3, and 4), based on years of practice and lifetime surgeries performed. Corneal endothelial characteristics were assessed using non-contact specular microscopy, with measurements taken before surgery and 30-60 days post-surgery.
RESULTS: Pre- and postoperative endothelial analysis showed no significant differences between surgeon levels regarding visual acuity achieved, corneal thickness, and endothelial hexagonality. However, the central endothelial cell density index showed a significantly greater reduction among level 1 surgeons (p=0.026). Grade II cataracts exhibited significant variations in the central endothelial cell density (p=0.011) and average cell size, with level 1 surgeons showing the largest increases (p=0.024).
CONCLUSIONS: The analysis revealed significant differences in visual acuity and endothelial indices between surgeon experience levels, with less experienced surgeons showing greater variations and poorer performance. Clinical protocols should consider these data to establish safer training protocols.
Keywords: Cataract extraction; Phacoemulsification; Endothelium; corneal; Lens implantation, intraocular; Visual acuity; Internship and residency; Surgeons
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
02-tab01tb.jpg)
08-fig01.jpg)
10-fig01.jpg)
03-fig01.jpg)
02-fig01.jpg)
03-fig01.jpg)
09-fig01.jpg)