Arq. Bras. Oftalmol. 2026; 89 (4): 10.5935/0004-2749.2025-0180
Total: 946
Dillan Cunha Amaral1; Tiago Nelson de Oliveira Rassi2; William Binotti3; Vinícius Freire Costa Alves4; Eduardo Henrique Cassins Aguiar1 ; Raphaela Masetto Fuganti5; Raíza Jacometti6; Mário Luiz Ribeiro Monteiro4,6; Antonio Marcelo Barbante Casella5; Ricardo Noguera Louzada1,6
DOI: 10.5935/0004-2749.2025-0180
ABSTRACT
This systematic review and meta-analysis aimed to compare the effectiveness and safety profiles of anti-vascular endothelial growth factor therapy with dexamethasone vs anti-vascular endothelial growth factor alone in patients with persistent diabetic macular edema. It was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline. Our data were prospectively registered on the International Prospective Register of Systematic Reviews (CRD42023482385). We searched the PubMed, Embase, Cochrane, and Web of Science databases for studies that compared treatment with anti-vascular endothelial growth factor and dexamethasone to anti-vascular endothelial growth factor alone in patients with persistent diabetic macular edema. The primary outcomes were changes in best corrected visual acuity, changes in central macular thickness, and the incidence of serious adverse events. Four studies were included, totaling 315 eyes. Of these 154 (48.88%) received anti-vascular endothelial growth factor alone, while 161 (51.12%) underwent combined therapy. Overall, combined therapy was associated with better central macular thickness (mean difference −68.21; p<0.001), although this did not translate into a significant difference in best-corrected visual acuity at 1 month follow-up (mean difference 1.29; p=0.55). There were significantly more intraocular pressure-related events (odds ratio 10.84; p=0.02) and cataract-related events (odds ratio 41.24; p<0.001) in the combined group than the anti-vascular endothelial growth factor alone group. Our results suggest that combined therapy improves macular morphology in persistent diabetic macular edema without increasing the risk of serious adverse events. However, its effects on final visual acuity outcomes were no better than those resulting from anti-vascular endothelial growth factor therapy alone.
Keywords: Diabetic macular edema; Macular edema; Central macular thickness Dexamethasone; Ozurdex; Anti-VEGF; Bevacizumab; Ranibizumab
INTRODUCTION
Diabetic macular edema (DME) is an ocular complication that can occur in patients with diabetes. It is defined as retinal thickening toward the center of the macula(1-3). In individuals with diabetic retinopathy, DME is the predominant cause of vision impairment. The typical treatment is anti-vascular endothelial growth factor (VEGF) therapy, which yields better anatomical outcomes and greater visual improvements than alternative monotherapies(3-6). However, poor responses to the periodic administration of anti-VEGF have been demonstrated among patients with DME. In approximately 25%-35% of patients treated with anti-VEGF, fluid reaccumulation occurs in the retina. This is diagnosed as persistent DME with poor visual prognosis.
Various treatment options for persistent DME have been explored. Increasing the dose of ranibizumab from that prescribed for standard DME has been found ineffective(7,8). Combined treatment with anti-VEGF and corticosteroids, such as triamcinolone, has shown promising results(8), but the current evidence is limited(9). The combined use of dexamethasone (DEXA) and anti-VEGF has been proposed for persistent DME, and initial studies have demonstrated favorable anatomical outcomes. Still, the reported effects on vision differ among studies(10-13). Also, concerns have been expressed about whether the addition of DEXA to anti-VEGF increases the incidence of adverse events(14).
In this systematic review and meta-analysis, we aim to clarify the safety and effectiveness of anti-VEGF and DEXA for persistent DME using comparative studies of anti-VEGF + DEXA and anti-VEGF monotherapy.
METHODS
Protocol and registration
The protocol for this meta-analysis followed the Cochrane Handbook for Systematic Reviews of Interventions and Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline(15). The study has been registered with the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42023482385).
Search strategy and data extraction
We searched the PubMed, Web of Science, Embase, and Cochrane Library databases from their inception to November 2023, without language restrictions. Our search terms were (Decaject OR Decameth OR Decaspray OR Dexasone OR Dexpak OR Hexadecadrol OR Hexadrol OR Maxidex OR methylfluorprednisolone OR Millicorten OR Oradexon OR dexamethasone) AND (bevacizumab OR Avastin OR Mvasi OR “anti-VEGF”) AND “diabetic macular edema” AND (persistent OR refractory OR resistant OR intractable). One author (DC) performed the search according to the PRISMA guideline, and another author (VA) independently peer-reviewed the search outcomes. Study eligibility was assessed independently by the same two reviewers (DA and VA). Duplicates were identified and removed, and then the titles and abstracts were screened. Those who did not meet our inclusion criteria or were deemed irrelevant were excluded. The remaining studies were retrieved, and the full manuscripts were screened. Further exclusions were made of those who did not meet our requirements, and the remaining papers were included in our review. The references from all included studies, as well as previous systematic reviews and meta-analyses, were also manually searched to identify additional studies.
Inclusion criteria
Studies that met all of the following eligibility criteria were included: (1) Randomized controlled trials (RCT) or nonrandomized prospective studies; (2) The inclusion of participants with persistent DME; (3) Comparison of combined anti-VEGF and DEXA to anti-VEGF only therapy was performed; (4) No minimum follow-up time; and (5) The assessment of any of the clinical outcomes of interest listed in the “endpoints and sensitivity analysis” subsection below. Studies that combined anti-VEGF with other corticosteroids, such as triamcinolone, were excluded due to potential and evident differences in their effects, safety profiles, administration routes, and therapeutic indications compared to those of DEXA(16). Studies with overlapping populations, animal studies, and in vitro experiments were also excluded.
Endpoints and sensitivity analysis
Our clinical outcomes of interest were: (1) Best corrected visual acuity (BCVA); (2) Central macular thickness (CMT); (3) Increased intraocular pressure (IOP), as indicated by the initiation of ocular antihypertensive medication; (4) Cataract-related events; and (5) Serious adverse events, including retinal detachment, vitreous hemorrhage, systemic inflammation, endophthalmitis, and uveitis. The included studies had short follow-up durations, with a maximum of 12 months, so the BCVA and CMT outcomes could only be assessed in the short term. We also performed a leave-one-out sensitivity analysis to determine the effects of each study on the estimated pooled analysis(17-22).
Quality of evidence assessment and risk of bias
We assessed all of the included studies for risk of bias and quality of evidence using ROBINS(23) or Cochrane’s Risk of Bias 2 (ROB2)(24). Two authors (DA and VF) independently evaluated bias risk and evidence quality. Any disagreements were settled by a third author (WB).
Statistical analysis
This systematic review and meta-analysis were conducted according to the Cochrane Collaboration and the PRISMA guidelines. Odds ratios (OR) with 95% confidence intervals were used to compare treatment effects for categorical endpoints. When necessary, we extracted data from graphs using the Web Plot Digitizer tool. Continuous outcomes were described as mean differences (MD). Heterogeneity between the studies was assessed using Cochran’s Q test, the I2 statistic, and the τ2 test. The random effects model was applied in all analyses. RevMan 5.3 (Cochrane Center, The Cochrane Collaboration, Odense, Denmark) software was used for statistical analysis.
RESULTS
Study selection and characteristics
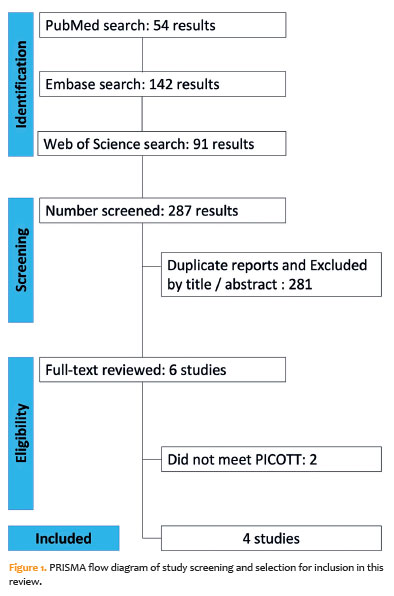
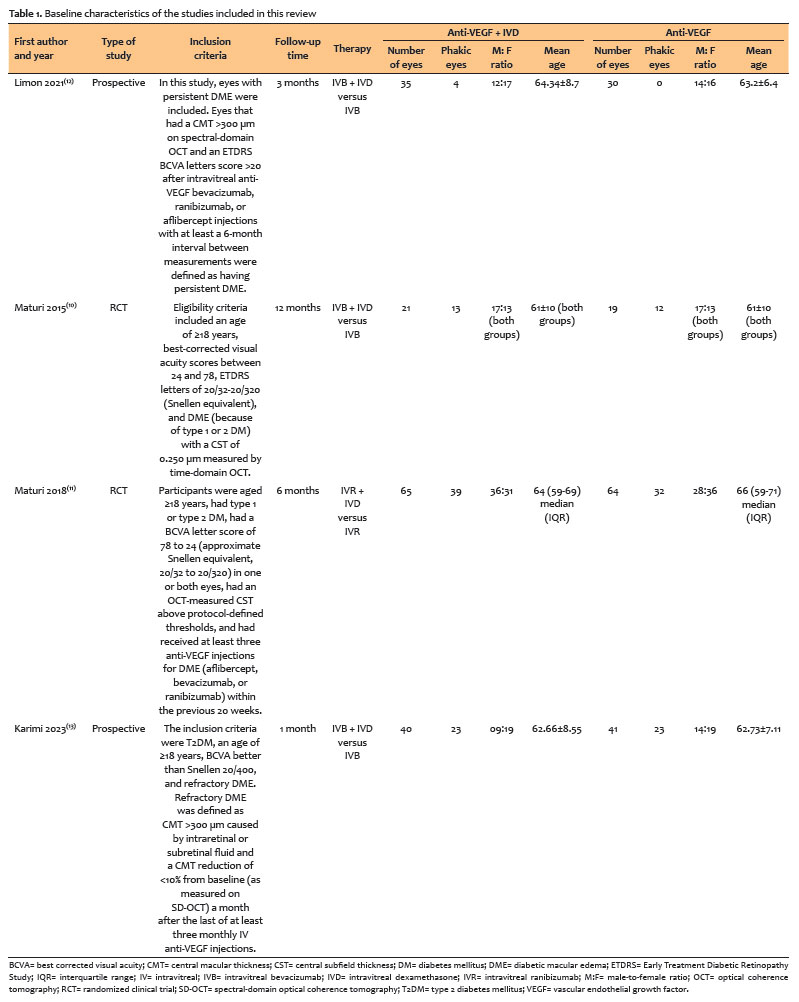
Our database searches returned a total of 287 articles. Of these, 54 were from PubMed, 142 from Embase, and 91 from Web of Science (Figure 1). After removing duplicate records and ineligible studies, six studies remained. These were thoroughly screened to ensure they met our inclusion criteria. Subsequently, two other articles were excluded, per our exclusion criteria. Finally, four studies were included in this review: two RCTs(10,11) and two nonrandomized prospective studies(12,13). A total of 315 eyes were analyzed. Of these, 161 received combined treatment and 154 received anti-VEGF only. The characteristics of the included studies are summarized in table 1.
Risk of bias assessment
To assess the risk of bias in the two RCTs, we used Cochrane’s ROB2 tool, while ROBINS-I was employed to evaluate the bias risk in the two non-RCTs. The results of the RCT assessments are shown in table 2, and those of the non-RCTs in table 3. The included RCTs were found to have either low risk or some concerns across the assessed domains. One of the RCTs showed potential bias in the measurement of outcomes(10). The non-RCTs were deemed to have low or moderate risks of bias within the evaluated domains. The moderate risks were due to possible confounders and potentially biased selection of the results reported(11,12).


Mean changes in central macular thickness
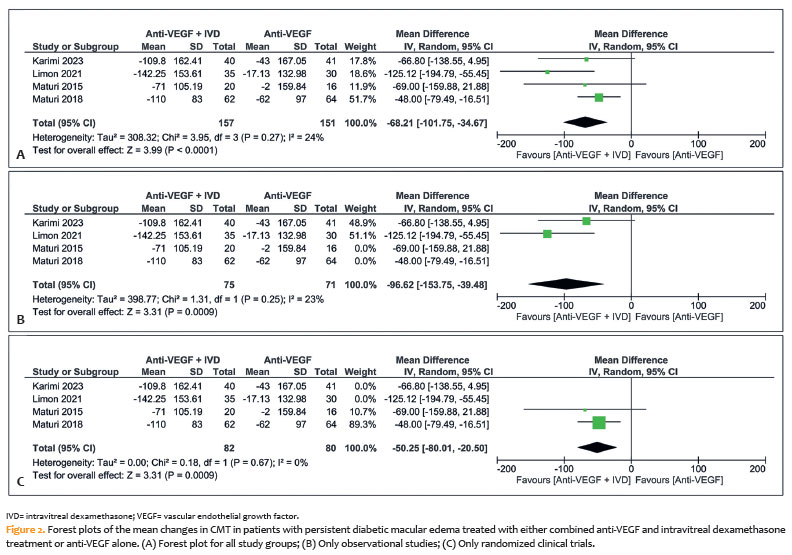
We found significantly greater improvement in CMT after treatment in the combined group than the anti-VEGF group (mean difference [MD] −68.21; 95% confidence interval (CI): −101.75 to −34.67; p<0.001; I²= 24%) (Figure 2A). Subgroup analyses of both the observational studies (MD −96.62; 95% CI: −153.75 to −39.48; p<0.001; I²= 23%) (Figure 2B) and the RCTs (MD −50.25; 95% CI: −80.01 to −20.50; p<0.001; I²= 0%) (Figure 2C) also showed significantly greater improvement in the combined therapy group.
Mean changes in best-corrected visual acuity
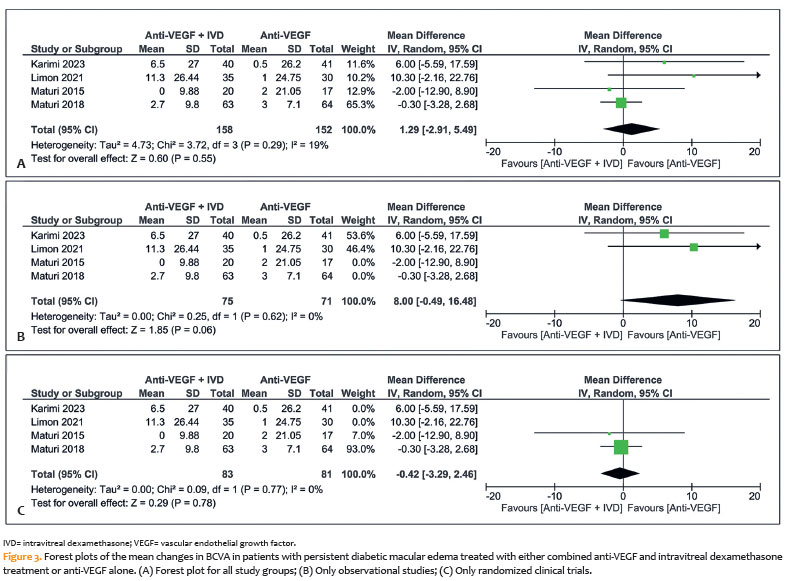
The pooled results revealed no significant difference in the mean BCVA between the two treatment groups (MD 1.29; 95% CI: −2.91 to 5.49; p=0.55; I²=19%) (Figure 3A). Subgroup analyses of only the observational studies (MD 8.00; 95% CI: −0.49 to 16.48; p=0.06; I²= 0%) (Figure 3B) and only the RCT studies (MD −0.42; 95% CI: −3.29 to 2.46; p=0.78; I²= 0%) (Figure 3C) also found no significant difference.
Increases in intraocular pressure
All of the included studies included increases in IOP among their outcomes. This was indicated by the need for ocular antihypertensive medication. The pooled results showed a significant difference in the occurrence of this outcome between the groups, with the anti-VEGF only group having a lower rate of IOP increase (OR 10.84; 95% CI: 2.38 to 49.26; p=0.002; I²=0%) (Figure 4A). Where required, the IOP was controlled with topical anti-glaucoma medications.
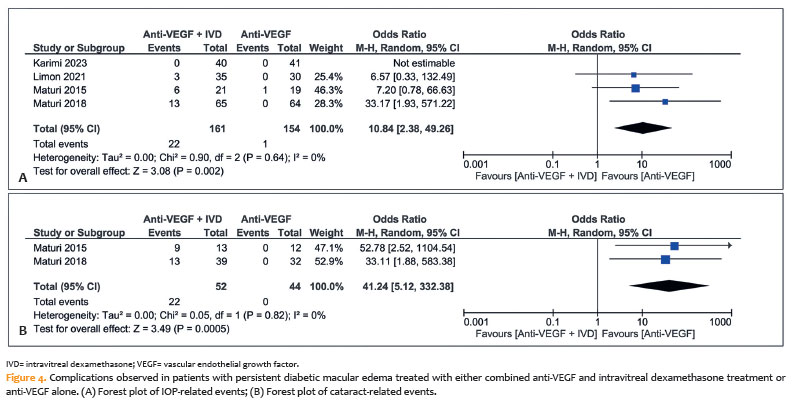
Incidence of cataract-related adverse events
Similarly, our pooled analysis showed a significantly higher incidence of cataracts in the combined therapy group than the anti-VEGF group (OR 41.24; 95% CI: 5.12 to 332.68; p<0.001; I²=0%; Figure 4B). Where required, cataract surgery was performed.
Serious adverse events
We reviewed all included studies for reports of serious complications and found three. There was one case of retinal detachment, one of vitreous hemorrhage, and one of inflammation. Maturi et al. (2018) reported between the analyzed studies(11).
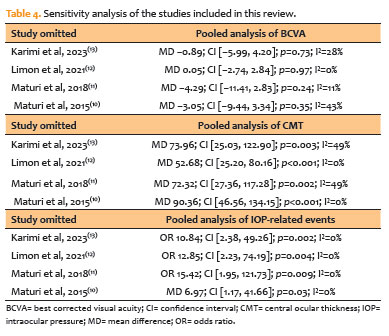
Sensitivity analysis
Our leave-one-out sensitivity analysis of the CMT, BCVA, and IOP outcomes revealed no significant deviations from the primary findings (Table 4).
DISCUSSION
This comprehensive review and meta-analysis evaluated the efficacy and safety of intravitreal anti-VEGF + DEXA for persistent DME. Our analysis included four studies, totaling 315 eyes. Specifically, these were two RCTs and two nonrandomized prospective studies. We found a notable improvement in CMT following combined therapy; however, we saw no corresponding improvement in visual acuity based on the BCVA values. There were significantly higher rates of IOP increase and cataract-related adverse events in the combined group than in the monotherapy group. Our leave-one-out sensitivity and subgroup analyses did not find any deviations from the primary findings, corroborating our main results.
Previous research has suggested that anti-VEGF + DEXA has greater therapeutic effects on CMT than anti-VEGF alone in patients with DME(25-27). Despite the limited number of comparative studies, combined therapy appears to be more effective in lowering CMT(11,12). Some studies have noted fluctuations in CMT during follow-up; however, the average CMT in combination groups remained more stable than in the monotherapy groups(10-13,25). These results suggest that the initial combination of DEXA and anti-VEGF may cause BCVA to increase more rapidly before reaching its plateau and induce a more enduring DME remission than anti-VEGF monotherapy(28).Our findings were consistent with those of previous studies, in which improvements in CMT were greater with the addition of DEXA, but with no concomitant improvement in visual acuity greater than that from anti-VEGF treatment alone(11,29). Both treatments appear to yield similar BCVA outcomes during follow-up.
This supports the contention that greater thinning of the macula may not necessarily improve visual acuity(30). Visual prognosis in patients with macular diseases tends to be more strongly correlated with the integrity of the inner and outer segments and the external limiting membrane (ELM) lines on spectral-domain OCT(31-33). The integrity of the outer retinal layers, particularly the ELM and the ellipsoid zone (EZ), is more strongly associated with BCVA than CMT. Disruption of the EZ and ELM reflects photoreceptor impairment and predicts poorer functional outcomes. Conversely, preserved or restored continuity is associated with a better posttreatment visual prognosis. Thus, these OCT biomarkers provide important prognostic information, which supports the notion that structural thinning of the macula is not the only contributor to visual recovery in DME(1,34-41). Another robust biomarker of reduced BCVA in DME and other conditions involving macular edema is an OCT finding of disorganization of the retinal inner layers (DRIL). This association has been shown to persist across multiple time points and treatment modalities(42-44). Specifically, the presence of DRIL at baseline predicts worse visual outcomes following either anti-VEGF and DEXA combination or DEXA monotherapy. Improvement or resolution of DRIL after treatment correlates with greater gains in visual acuity(43,45). In eyes treated with DEXA implants, patients without baseline DRIL were found to achieve significantly more visual improvement and greater reductions in central retinal thickness. DEXA has demonstrated the potential to ameliorate DRIL in a substantial proportion of cases(43). Similar findings have been reported with anti-VEGF therapy. Baseline DRIL and DRIL that persists after treatment are associated with poorer visual outcomes, while reductions in DRIL are linked to greater BCVA improvements(45).
There have been few comparisons of the effects of anti-VEGF + DEXA versus DEXA alone on DRIL and BCVA in the current literature. However, the available evidence indicates that both treatments can lead to DRIL improvements and consequent improvements in visual outcomes. It also consistently shows the presence or persistence of DRIL to be a negative prognostic factor, regardless of the pharmacologic approach(43,45,46).
A recent meta-analysis revealed that OCT patterns such as tractional retinal detachment (TRD), serous retinal detachment (SRD), and cystoid macular edema (CME) significantly influence the efficacy of anti-VEGF agents. Conbercept was found to be more effective in reducing CMT and improving BCVA in patients with TRD, while ranibizumab and bevacizumab performed best in cases of CME and SRD, respectively(47). This highlights the importance of a personalized approach in treating DME. OCT-based classification can inform the selection of the most suitable anti-VEGF agent, improving clinical outcomes by considering the structural and functional characteristics of the individual retina. Future randomized studies using this technology will clarify this.
Our findings are in agreement with previous studies, which show that eyes treated with both DEXA and anti-VEGF agents have a higher risk of elevated IOP and cataract progression compared to those treated with only anti-VEGF agents(48-50). Generally, corticosteroid use to treat eye conditions has been associated with cataract formation during longer follow-up(51,52). Only one study in this review reported 12-month follow-up outcomes, with follow-up in all others being relatively short. In the longer-term study, the combination group showed a higher rate of cataract progression. Similar findings have been reported in a recent meta-analysis, which found higher rates of cataracts and IOP in a combined anti-VEGF + corticosteroids group than an anti-VEGF alone group(29). The absence of visual improvement in some phakic eyes in the combination group could be explained by early cataract development in patients who had not yet undergone cataract surgery(11). Long-term studies are needed to determine the long-term outcomes in such cases.
These safety concerns further highlight the importance of tailoring therapy to individual patient characteristics. In clinical practice, the choice between anti-VEGF monotherapy and combination therapy with corticosteroids should consider patient variables. For example, phakic patients have a higher risk of cataract progression, whereas pseudophakic patients and those unresponsive to anti-VEGF alone may benefit more from adjunctive corticosteroid treatment. Similarly, patients with poor adherence, systemic contraindications to frequent injections, or persistent edema despite anti-VEGF may be candidates for a combination approach. Integrating these considerations into individualized treatment decisions is essential for achieving the optimal balance between efficacy and safety in the management of DME(1).
Anti-VEGF and DEXA treatments carry risks, including potential complications like endophthalmitis(53-56). However, we observed no significant difference in the rate of serious complications between the combined and anti-VEGF treatment groups.
Beyond anti-VEGF and dexamethasone therapies, several adjunctive or alternative treatments have been investigated for DME. Intravitreal corticosteroids, such as fluocinolone acetonide implants and triamcinolone injections, have been shown to effectively reduce macular thickness and improve BCVA; however, their use is limited by the relatively high risks of cataract progression and IOP elevation(35,36). Subthreshold and micropulse laser therapies have also emerged as nondamaging approaches that may benefit DME patients, particularly those who are refractory to anti-VEGF therapy. These methods have fewer retinal side effects than conventional laser treatments(1).
Alternative or adjunctive options for treating persistent DME include pars plana vitrectomy. This is particularly appropriate in cases with substantial vitreomacular traction(57) and is included in the American Academy of Ophthalmology’s Diabetic Retinopathy Preferred Practice Pattern (PPP) 2024 guideline. Vitrectomy may improve visual acuity in certain patients with diffuse DME that is unresponsive to macular laser photocoagulation and/or anti-VEGF therapy. However, the outcomes are variable and difficult to study in RCTs due to confounding factors(34). These alternatives highlight the diverse therapeutic landscape in which combination strategies must be contextualized.
This meta-analysis had some limitations. First, we were only able to find four relevant studies (two RCTs and two prospective nonrandomized studies), comprising a total of 315 eyes. This restricts the generalizability of our findings. The limited number of RCTs may also have reduced the statistical power, potentially preventing the detection of some differences between groups. A further impediment is that the definition of persistent DME varies greatly among studies, leading to a lack of consensus. Nonetheless, our analysis stands out as the most comprehensive to date. We found moderate to high heterogeneity between studies in the key outcomes. This may be attributed to the variable quality and differing demographics of the studies. To address this, we conducted leave-one-out sensitivity and subgroup analyses, applied rigorous inclusion criteria, and used the Mantel-Haenszel random-effects model to account for variability. Another limitation was that our meta-analysis relied on aggregated data from published studies, so individual patient data were not available for more detailed subgroup analysis, which limited the depth of our understanding of the treatment effects and prevented the identification of predictors of treatment response.
In this meta-analysis, we reviewed four studies. We collated their data to compare the safety and effectiveness of combined anti-VEGF and DEXA treatment and anti-VEGF treatment alone for persistent DME. We found that the combined therapy was more effective than anti-VEGF alone in reducing CMT, but did not improve BCVA values. The combined therapy group experienced more adverse events related to increased IOP and cataracts without evidence of increased serious adverse events in the short term. Future trials are needed to define the long-term effectiveness and obtain a better understanding of the side effects of this combined therapy. Research is also needed to establish standardized guidelines for managing treatment-resistant DME and to identify alternative options for patients with persistent DME. Large-scale RCTs are required to confirm our findings.
AUTHORS’ CONTRIBUTION
Significant contribution to conception and design: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Data Acquisition: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Data Analysis and Interpretation: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Manuscript Drafting: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Significant intellectual content revision of the manuscript: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Final approval of the submitted manuscript: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Statistical analysis: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada. Research group leadership: Dillan Cunha Amaral, Tiago Nelson de Oliveira Rassi, William Binotti, Vinícius Freire Costa Alves, Eduardo Henrique Cassins Aguiar, Raphaela Masetto Fuganti, Raíza Jacometti, Mário Luiz Ribeiro Monteiro, Antonio Marcelo Barbante Casella, Ricardo Noguera Louzada.
REFERENCES
1. Tatsumi T. Current treatments for diabetic macular edema. Int J Mol Sci. 2023;24(11):9591.
2. Bandello F, Battaglia Parodi M, Lanzetta P, Loewenstein A, Massin P, Menchini F, et al. Diabetic macular edema. Dev Ophthalmol. 2017;58(58):102-38.
3. Chauhan MZ, Rather PA, Samarah SM, Elhusseiny AM, Sallam AB. Current and Novel Therapeutic Approaches for Treatment of Diabetic Macular Edema. Cells. 2022;11(12):1950.
4. Khan MA, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of type 2 diabetes - global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107-11.
5. Rassi TN, Barbosa LM, Amaral DC, Louzada RN, Filho HN, Marques GN, et al. Meta-analysis: long/short-term efficacy of anti-VEGF vs. panretinal photocoagulation in preventing severe complications in proliferative diabetic retinopathy. Int J Retina Vitreous. 2025;11(1):76.
6. Rassi TN, Amaral DC, Mund E, Pimentel AL, Louzada RN, Maia M. Assessing long-term feasibility and efficacy of treatments for retinal vein occlusion macular edema: a systematic review and network meta-analysis of randomized clinical trials. J Ocul Pharmacol Ther. 2025;10807683251380974. https://doi.org/10.1177/10807683251380974.
7. Busbee BG, Ho AC, Brown DM, Heier JS, Suñer IJ, Li Z, Rubio RG, Lai P.; HARBOR Study Group. Twelve-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2013;120(5):1046-56.
8. Veritti D, Sarao V, Lanzetta P. Bevacizumab and triamcinolone acetonide for choroidal neovascularization due to age-related macular degeneration unresponsive to antivascular endothelial growth factors. J Ocul Pharmacol Ther. 2013;29(4):437-41.
9. Schaal S, Kaplan HJ, Tezel TH. Is there tachyphylaxis to intravitreal anti-vascular endothelial growth factor pharmacotherapy in age-related macular degeneration? Ophthalmology. 2008;115(12):2199-205.
10. Maturi RK, Bleau L, Saunders J, Mubasher M, Stewart MW. A 12-month, single-masked, randomized controlled study of eyes with persistent diabetic macular edema after multiple anti-VEGF injections to assess the efficacy of the dexamethasone-delayed delivery system as an adjunct to bevacizumab compared with continued bevacizumab monotherapy. Retina. 2015;35(8):1604-14.
11. Maturi RK, Glassman AR, Liu D, Beck RW, Bhavsar AR, Bressler NM, Jampol LM, Melia M, Punjabi OS, Salehi-Had H, Sun, JK; Diabetic retinopathy clinical research network. Effect of adding dexamethasone to continued ranibizumab treatment in patients with persistent diabetic macular edema: a DRCR network phase 2 randomized clinical trial. JAMA Ophthalmol. 2018;136(1):29-38.
12. Limon U. Early effect of simultaneous intravitreal dexamethasone and bevacizumab combination treatment in patients with persistent diabetic macular edema. J Fr Ophtalmol. 2021;44(6):849-54.
13. Karimi S, Karrabi N, Hassanpour K, Amirabadi A, Daneshvar K, Nouri H, et al. The additive effect of intravitreal dexamethasone combined with bevacizumab in refractory diabetic macular edema. J Fr Ophtalmol. 2023;46(9):1019-29.
14. Kuppermann BD, Blumenkranz MS, Haller JA, Williams GA, Weinberg DV, Chou C, Whitcup SM; Dexamethasone DDS phase ii study group. Randomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edema. Arch Ophthalmol. 2007;125(3):309-17.
15. Cumpston MS, McKenzie JE, Welch VA, Brennan SE. Strengthening systematic reviews in public health: guidance in the Cochrane Handbook for Systematic Reviews of Interventions, 2nd edition. J Public Health (Oxf). 2022;44(4):e588-92.
16. Salvetat ML, Pellegrini F, Spadea L, Salati C, Musa M, Gagliano C, et al. The treatment of diabetic retinal edema with intravitreal steroids: how and when. J Clin Med. 2024;13(5):1327.
17. Richardson M, Garner P, Donegan S. Interpretation of subgroup analyses in systematic reviews: A tutorial. Clin Epidemiol Glob Health. 2019;7(2):192-8.
18. Len P, Iskakova G, Sautbayeva Z, Kussanova A, Tauekelova AT, Sugralimova MM, et al. Meta-analysis and systematic review of coagulation disbalances in COVID-19: 41 studies and 17,601 patients. Front Cardiovasc Med. 2022;9:794092.
19. Hysong SJ. Meta-analysis: audit and feedback features impact effectiveness on care quality. Med Care. 2009;47(3):356-63.
20. Brand KJ, Hapfelmeier A, Haller B. A systematic review of subgroup analyses in randomised clinical trials in cardiovascular disease. Clin Trials. 2021;18(3):351-60.
21. Stieb DM, Zheng C, Salama D, Berjawi R, Emode M, Hocking R, et al. Systematic review and meta-analysis of case-crossover and time-series studies of short term outdoor nitrogen dioxide exposure and ischemic heart disease morbidity. Environ Health. 2020;19(1):47.
22. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-60.
23. Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
24. Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
25. Lin TC, Chung YC, Hsu TK, Huang HW, Huang YM, Chou YC, et al. Therapeutic effect of simultaneous intravitreal dexamethasone and aflibercept on diabetic macular edema. Acta Diabetol. 2022;59(4):501-8.
26. Kaya M, Atas F, Kocak N, Ozturk T, Ayhan Z, Kaynak S. Intravitreal ranibizumab and dexamethasone implant injections as primary treatment of diabetic macular edema: the month 24 results from simultaneously double protocol. Curr Eye Res. 2023;48(5):498-505.
27. Kaya M, Kocak N, Ozturk T, Bolluk V, Ayhan Z, Kaynak S. Intravitreal ranibizumab and dexamethasone implant injections as primary treatment of diabetic macular edema: simultaneously double protocol. Eye (Lond). 2021;35(3):777-85.
28. Amoaku WM, Saker S, Stewart EA. A review of therapies for diabetic macular oedema and rationale for combination therapy. Eye (Lond). 2015;29(9):1115-30.
29. Hatamnejad A, Orr S, Dadak R, Khanani A, Singh R, Choudhry N. Anti-VEGF and steroid combination therapy relative to anti-VEGF mono therapy for the treatment of refractory DME: A systematic review of efficacy and meta-analysis of safety. Acta Ophthalmol. 2024;102(3):e204-14.
30. Flaxel CJ, Edwards AR, Aiello LP, Arrigg PG, Beck RW, Bressler NM, et al. Factors associated with visual acuity outcomes after vitrectomy for diabetic macular edema: diabetic retinopathy clinical research network. Retina. 2010;30(9):1488-95.
31. Chhablani JK, Kim JS, Cheng L, Kozak I, Freeman W. External limiting membrane as a predictor of visual improvement in diabetic macular edema after pars plana vitrectomy. Graefes Arch Clin Exp Ophthalmol. 2012;250(10):1415-20.
32. Uji A, Murakami T, Nishijima K, et al. Association between hyperreflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic macular edema. Am J Ophthalmol. 2012;153(4):710-7.e1.
33. Coscas G, Coscas F, Zucchiatti I, Glacet-Bernard A, Soubrane G, Souïed E. SD-OCT pattern of retinal venous occlusion with cystoid macular edema treated with Ozurdex®. Eur J Ophthalmol. 2011; 21(5):631-6.
34. American Academy of Ophthalmology. Diabetic Retinopathy Preferred Practice Pattern®. California: American Academy of Ophthalmology; 2024.
35. Zhou B, Liu H, Xiong F. Efficacy and safety of dexamethasone or triamcinolone in combination with anti-vascular endothelial growth factor therapy for diabetic macular edema. a systematic review and meta-analysis with trial sequential analysis. PLoS One. 2025;20(2):e0318373.
36. Cheng Z, Liu X. Comparing the efficacy of glucocorticoids and anti-VEGF in treating diabetic macular edema: systematic review and comprehensive analysis. Front Endocrinol (Lausanne). 2024;15:1342530.
37. Chen C, Wang Z, Yan W, Lan Y, Yan X, Li T, et al. Anti-VEGF combined with ocular corticosteroids therapy versus anti-VEGF monotherapy for diabetic macular edema focusing on drugs injection times and confounding factors of pseudophakic eyes: a systematic review and meta-analysis. Pharmacol Res. 2023;196:106904.
38. Ma Y, Tao Y, Yuan M, Sun X. Anti-vascular endothelial growth factor combined with ocular steroid therapy for persistent diabetic macular edema. a systematic review and meta-analysis. Pharmaceuticals (Basel). 2024;17(12):1574.
39. Chi SC, Kang YN, Huang YM. Efficacy and safety profile of intravitreal dexamethasone implant versus antivascular endothelial growth factor treatment in diabetic macular edema. a systematic review and meta-analysis. Sci Rep. 2023;13(1):7428.
40. Tang HX, Li JJ, Yuan Y, Ling Y, Mei Z, Zou H. Comparing the efficacy of dexamethasone implant and anti-vegf for the treatment of macular edema: a systematic review and meta-analysis. PLoS One. 2024;19(7):e0305573.
41. Fallico M, Lotery A, Maugeri A, Favara G, Barchitta M, Agodi A, et al. Intravitreal dexamethasone implant versus anti-vascular endothelial growth factor therapy combined with cataract surgery in patients with diabetic macular oedema: a systematic review with meta-analysis. Eye (Lond). 2022;36(12): 2239-46.
42. Nanji K, Grad J, Hatamnejad A, El-Sayes A, Mihalache A, Gemae M, et al. Baseline optical coherence tomography biomarkers associated with visual acuity in diabetic macular edema: a systematic review and meta-analysis. Ophthalmology. 2025;Aug 11:S0161-6420(25)00483-X.
43. Zur D, Iglicki M, Sala-Puigdollers A, Chhablani J, Lupidi M, Fraser-Bell S, et al. Disorganization of retinal inner layers as a biomarker in patients with diabetic macular oedema treated with dexamethasone implant. Acta Ophthalmologica. 2020;98(2):e217-23.
44. Moein HR, Novais EA, Rebhun CB, Cole ED, Louzada RN, Witkin AJ, et al. Optical coherence tomography angiography to detect macular capillary ischemia in patients with inner retinal changes after resolved diabetic macular edema. Retina. 2018;38(12):2277-84.
45. Szeto SK, Hui VW, Tang FY, Yang D, Sun ZH, Mohamed S, et al. OCT-based biomarkers for predicting treatment response in eyes with centre-involved diabetic macular oedema treated with anti-vegf injections: a real-life retina clinic-based study. Br J Ophthalmol. 2023;107(4):525-33.
46. Nanji K, Hatamnejad A, Grad J, El-Sayes A, Mihalache A, Gemae M, et al. Visual outcomes associated with optical coherence tomography biomarkers in diabetic macular edema: a systematic review. Surv Ophthalmol. 2025 Sep 17:S0039-6257(25)00176-6.
47. Yao J, Huang W, Gao L, Liu Y, Zhang Q, He J, et al. Comparative efficacy of anti-vascular endothelial growth factor on diabetic macular edema diagnosed with different patterns of optical coherence tomography: A network meta-analysis. PLoS One. 2024;19(6):e0304283.
48. Kuroiwa DA, Malerbi FK, Regatieri CV. New Insights in Resistant Diabetic Macular Edema. Ophthalmologica. 2021;244(6):485-94.
49. Zur D, Iglicki M, Loewenstein A. The Role of Steroids in the Management of Diabetic Macular Edema. Ophthalmic Res. 2019; 62(4):231-6.
50. Veiga Reis F, Dalgalarrondo P, da Silva Tavares Neto JE, Wendeborn Rodrigues M, Scott IU, Jorge R. Combined intravitreal dexamethasone and bevacizumab injection for the treatment of persistent diabetic macular edema (DexaBe study): a phase I clinical study. Int J Retina Vitreous. 2023;9(1):13.
51. Rice JB, White AG, Scarpati LM, Wan G, Nelson WW. Long-term Systemic Corticosteroid Exposure: A Systematic Literature Review. Clin Ther. 2017;39(11):2216-29.
52. Gaballa SA, Kompella UB, Elgarhy O, Alqahtani AM, Pierscionek B, Alany RG, et al. Corticosteroids in ophthalmology: drug delivery innovations, pharmacology, clinical applications, and future perspectives. Drug Deliv Transl Res. 2021;11(3):866-93.
53. Falavarjani KG, Nguyen QD. Adverse events and complications associated with intravitreal injection of anti-VEGF agents: a review of literature. Eye (Lond). 2013;27(7):787-94.
54. Alfatih M, Adishabri AK, Dewi NL, Rifa’i AZ, Kemuning M, Amaral DC, et al. Proportion of eyes with visual-acuity improvement after vitrectomy for post-traumatic endophthalmitis: A meta-analysis. AJO Int. 2025;2(4):100174.
55. Pedrotti Chavez M. Rassi TNdO, Moreno Yate C, Amaral DC, Brasil LM, Vasconcelos TGC, et al. Prevalence of intravitreal silicone oil following intravitreal injections: a meta-analysis. Am J Ophthalmol. 2025 Sep 26:S0002-9394(25)00521-5.
56. Cruz MR, Amaral DC, Gonçalves OR, Cyrino LG, Nascimento LM, Barroso FV, et al. Chlorhexidine compared with povidone-iodine in intravitreal injection: a systematic review and meta-analysis. J Ocul Pharmacol Ther. 2025;41(3):162-8.
57. Louzada RN, Ferrara D, Moult EM, Fujimoto JG, Abu-Qamar O, Duker JS, et al. Full-thickness macular hole size by hypertransmission signal on spectral-domain optical coherence tomography. Retina. 2021;41(10):2059-65.
Submitted for publication:
July 17, 2025.
Accepted for publication:
October 8, 2025.
Data Availability Statement: The datasets generated and/or analyzed during the current study are available on the International Prospective Register of Systematic Reviews (registration identification: CRD42023482385)
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Caio V. Regatieri
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.