Arq. Bras. Oftalmol. 2026; 89 (3): 10.5935/0004-2749.2025-0243
Total: 518
Berire Şeyma Durmuş Ece1; Erdem Yüksel2
DOI: 10.5935/0004-2749.2025-0243
ABSTRACT
PURPOSE: To evaluate the impact of varying degrees of trabeculotomy during gonioscopy-assisted transluminal trabeculotomy surgery on postoperative intraocular pressure reduction and surgical success.
METHODS: Patients who underwent gonioscopy-assisted transluminal trabeculotomy (at least 90°) for open-angle glaucoma and had a follow-up period of at least 12 months were included. Patients were grouped according to trabeculotomy degree (Group 1: 90°<θ≤180°; Group 2: 180°<θ<360°; Group 3: θ=360°). Ophthalmic examination findings, intraocular pressure measurements, number of antiglaucoma medications, and complications were recorded. Surgical success was defined as intraocular pressure <15 mmHg with at least a 20% reduction; surgical failure was defined as failure to meet this criterion or the need for additional surgery.
RESULTS: A total of 100 patients were included: 20 in Group 1, 24 in Group 2, and 56 in Group 3. Intraocular pressure levels differed significantly only in the first postoperative month (p=0.013). At 12 months, intraocular pressure levels, percentage reduction in intraocular pressure, and mean number of antiglaucoma medications did not differ significantly (p>0.05). No correlation was found between trabeculotomy degree and percentage intraocular pressure reduction (p=0.173). At 12 months, surgical success rates were similar (60.0%, 58.3%, and 64.3% for Groups 1, 2, and 3, respectively). Complication rates were also comparable among the groups.
CONCLUSION: The degree of trabeculotomy did not affect surgical success over a 12-month follow-up period. Although early intraocular pressure reduction may differ with 360° trabeculotomy, a complete 360° incision may not be necessary to achieve optimal pressure reduction.
Keywords: Gonioscopy; Trabeculotomy; Glaucoma, open-angle; segmental GATT antiglaucoma agents; Intraocular pressure
INTRODUCTION
Gonioscopy-assisted transluminal trabeculotomy (GATT) is a minimally invasive glaucoma surgery that restores aqueous outflow through the eye’s natural drainage system while preserving the conjunctiva. It serves as an alternative to bleb-dependent procedures and effectively reduces intraocular pressure (IOP) in a cost-efficient manner. GATT is performed ab interno using a microcatheter or suture to facilitate cannulation of Schlemm’s canal (SC). Previous studies have demonstrated its effectiveness in treating primary open-angle glaucoma (POAG), congenital glaucoma, juvenile open-angle glaucoma, pseudoexfoliation (PXF) glaucoma, and steroid-induced glaucoma(1-4).
Aqueous humor outflow through the trabecular meshwork (TM) and Schlemm’s canal is segmental and nonuniform, with resistance primarily located in the juxtacanalicular tissue and the inner wall of Schlemm’s canal. Theoretically, the reduction in IOP following GATT may be proportional to the extent of TM bypassed, allowing aqueous humor to access the distal outflow system. However, a study on enucleated human eyes reported that a 360° incision in Schlemm’s canal resulted in a 75% loss of outflow resistance, whereas a 120° incision produced an 85% reduction in IOP relative to a 360° incision(5).
This observation may be explained by the structure of distal outflow pathways—including collector channels, the intrascleral venous plexus, and episcleral veins—which function as independent flow units with varying resistances. Thus, although a wider trabeculotomy may bypass a larger portion of the TM, the functional integrity of distal pathways ultimately determines the degree of IOP reduction. Furthermore, microanatomical imaging studies have shown that certain regions of the TM contribute disproportionately to aqueous outflow, suggesting that trabeculotomy performed in more active drainage regions may yield comparable outcomes even with smaller incisions(6). These findings provide a physiological rationale for investigating whether increasing trabeculotomy extent proportionally improves clinical outcomes in GATT surgery.
Previous studies have reported conflicting results: some found no correlation between trabeculotomy extent and IOP reduction, whereas others suggested improved outcomes with larger degrees of trabeculotomy(7,8). Despite numerous studies using different techniques and extents of trabeculotomy, the relationship between incision extent and clinical outcomes remains controversial(9). While several studies have compared 180° and 360° GATT, few have classified trabeculotomy into graded ranges and conducted a three-arm analysis to evaluate different extents(10,11).
The objective of this study was to assess the relationship between the degree of trabeculotomy performed during GATT surgery and postoperative IOP reduction, as well as surgical success.
METHODS
Patients with moderate to advanced open-angle glaucoma who underwent GATT (with at least 90° trabeculotomy) and had a minimum follow-up of 12 months were included in this retrospective study. Patients who had previously undergone glaucoma surgery or had incomplete follow-up were excluded. The study adhered to the principles of the Declaration of Helsinki and was approved by the local ethics committee (2023-KAEK-81). Informed consent was obtained from all patients prior to surgery.
Patients were classified into three groups based on the degree of trabeculotomy performed: 90°<θ≤180° (Group 1), 180°<θ<360° (Group 2), and θ=360° (Group 3). Ophthalmological examination findings, IOP levels, and the number of antiglaucoma medications were recorded preoperatively and at 1, 3, 6, and 12 months postoperatively. Surgical success was defined as an IOP <15 mmHg, with or without medication, along with at least a 20% reduction in IOP. Failure was defined as not meeting these criteria or requiring additional surgery to control IOP. Surgical success was assessed starting from the first postoperative month to minimize the impact of early postoperative IOP fluctuations. IOP spikes were defined as IOP ≥30 mmHg within the first postoperative month. IOP values, percentage reductions in IOP, number of antiglaucoma medications, cumulative surgical success rates (Kaplan-Meier survival analysis), frequency of hyphema on postoperative day 1, and complications were recorded and compared among the groups.
Surgical technique
A 2.4-mm slit knife was used to create a temporal corneal incision. A 20-gauge MVR blade was then used to create an approximately 15° oblique paracentesis in either the superonasal or inferonasal quadrant. Following intracameral administration of preservative-free 1% lidocaine, a dispersive viscoelastic was injected into the anterior chamber. The patient was positioned to optimize visualization of the nasal TM, and a Swan-Jacob gonioscope was used to visualize the iridocorneal angle.
A 1- to 2-mm goniotomy was performed using a 20-gauge MVR blade. A thermally blunted 5-0 polypropylene suture was advanced into SC using 23-gauge microforceps. After advancing the suture tip circumferentially (up to 360°) within the SC, it was withdrawn to complete the trabeculotomy. If cannulation was obstructed due to resistance within the SC, the suture was retracted and reinserted from the opposite side of the goniotomy to achieve reverse cannulation.
In cases where the suture could not be advanced 360°, it was grasped and withdrawn from the goniotomy site, and a limited trabeculotomy was performed up to the point of obstruction. For such cases, the degree of trabeculotomy was recorded based on the distal extent of the suture. When trabeculotomy was performed in both directions, the total degree was recorded.
Hyphema was evacuated as needed, and cataract surgery was performed in eligible patients using standard phacoemulsification techniques. Approximately 20% of the cohesive viscoelastic was intentionally left in the anterior chamber at the end of the procedure.
Postoperatively, patients were prescribed topical antibiotics for 1 week as well as topical steroids and nonsteroidal anti-inflammatory drugs for 4 weeks. Beginning in the first postoperative week, topical pilocarpine (Pilosed, 2%) was administered three times daily for 1 month.
Statistical analysis
Descriptive statistics, including mean, standard deviation (SD), frequency, and percentage, were used to summarize the data. The distribution of quantitative variables was assessed using the Kolmogorov-Smirnov or Shapiro-Wilk test, depending on sample size. Variables with a normal distribution were presented as mean±SD, whereas non-normally distributed variables were presented as median (minimum-maximum). Categorical variables were expressed as counts (n) and percentages (%).
The chi-square test or Fisher’s exact test was used to compare categorical variables. The Kruskal-Wallis test was used for comparisons among the three groups, and the Mann-Whitney U test was used for pairwise comparisons. Changes in IOP and medication counts before and after surgery within the same group were analyzed using the Wilcoxon signed-rank test.
Spearman correlation analysis was used to evaluate the relationship between trabeculotomy degree and percentage reduction in IOP at 12 months. Logistic regression models were applied to identify factors associated with surgical success at 12 months. Univariate logistic regression analysis included age, sex, glaucoma type (POAG vs. PXF glaucoma), and surgical type (GATT alone vs. combined surgery).
Kaplan-Meier survival analysis was used to evaluate cumulative surgical success over the 12-month follow-up period. Survival curves were compared using the log-rank test. A p value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS software (version 26.0; IBM Corp., Chicago, Illinois).
RESULTS
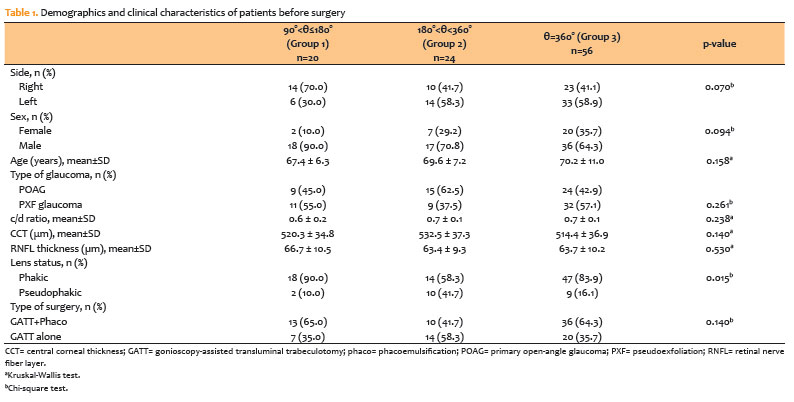
A total of 100 patients were included in the study. Based on the grouping according to GATT degree, Group 1 (90°<θ≤180°) consisted of 20 patients, Group 2 (180°<θ<360°) comprised 24 patients, and Group 3 (θ=360°) comprised 56 patients. The demographic and clinical characteristics of the patients are presented in table 1. There were no significant differences among the groups in terms of age or gender (p>0.05). Significant differences were observed in lens status (p=0.015), whereas no significant difference was found in the type of surgery performed (p=0.140). The mean GATT degrees were 168.0±24.6° (range: 120°-180°) in Group 1, 229.5±34.9° (range: 200°-270°) in Group 2, and 360.0±0.0° in Group 3.
Mean IOP levels preoperatively and at 1, 3, 6, and 12 months postoperatively, percentage reduction in IOP at 12 months, and mean number of antiglaucoma medications are shown in table 2. No significant differences were observed among the groups in preoperative mean IOP levels (p>0.05). During the postoperative period, significant differences in mean IOP were observed only at 1 month (p=0.013). Pairwise analysis at 1 month showed no significant differences between Groups 1 and 2 or between Groups 2 and 3 (p>0.05), whereas significantly lower mean IOP was observed in Group 3 compared with Group 1 (p=0.007).
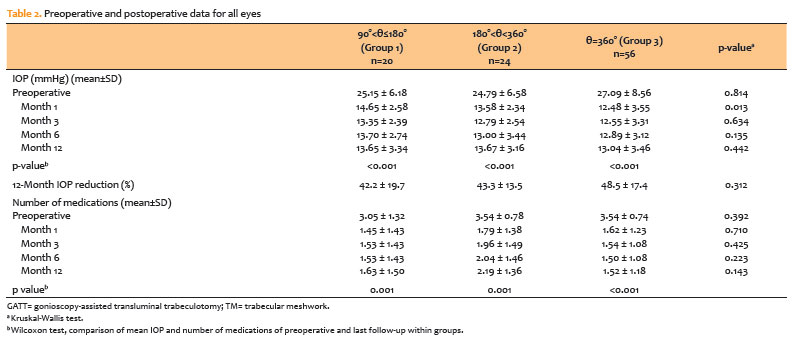
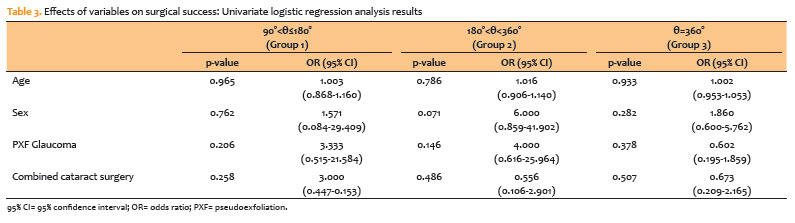
There were no significant differences among the groups in the mean number of antiglaucoma medications, either preoperatively or postoperatively (p>0.05). No correlation was found between GATT degree and percentage reduction in IOP at 12 months compared with baseline (p=0.173). Regression analysis did not reveal any significant associations between evaluated factors and surgical success at 12 months within each group (p>0.05 for all factors; table 3).
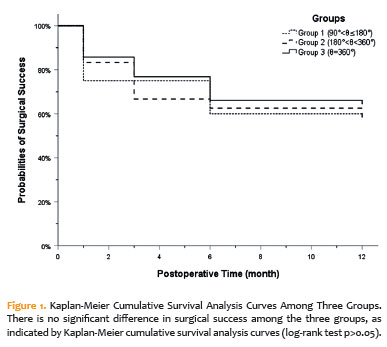
At 12 months, surgical success rates were 60.0%, 58.3%, and 64.3% for Groups 1, 2, and 3, respectively. Kaplan-Meier survival curves are shown in figure 1. Log-rank testing of the Kaplan-Meier curves showed no significant differences among the three groups (p=0.833).
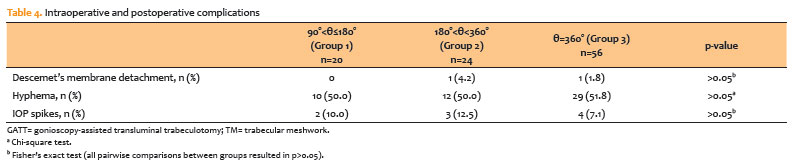
Intraoperative and postoperative complications are presented in Table 4. Hyphema involving at least 50% of the anterior chamber was observed in all three groups (50.0%, 50.0%, and 51.8% for Groups 1, 2, and 3, respectively). In all cases, hyphema resolved spontaneously within 1 week without additional surgical intervention. No significant differences were observed among the groups in complication rates (p>0.05).
DISCUSSION
In this study, patients were divided into three groups based on the degree of trabeculotomy, and significant reductions in both IOP and the number of antiglaucoma medications were observed at 12 months postoperatively in each group. Although significant differences in IOP were observed among the groups at 1 month, these differences resolved during follow-up, and no significant differences in surgical success were found at 12 months.
In the literature, a study conducted on enucleated human eyes showed that increasing the extent of trabeculotomy progressively reduced outflow resistance, but not in a linear manner. The initial 30° incision produced a disproportionately greater reduction in resistance compared with additional increments. In that study, a 360° trabeculotomy eliminated 71% of outflow resistance at a perfusion pressure of 25 mmHg, whereas a 30° trabeculotomy accounted for 41% of the total effect, and a 120° trabeculotomy accounted for 79%(12). In another study, Sato et al.(11) compared 360° trabeculotomy with superior 180° and inferior 180° incisions in GATT surgery and found similar mean reductions in IOP and medication use across all groups. They concluded that the extent and location of SC incision did not significantly influence IOP reduction or medication burden at 12 months. Similarly, Zhang et al.(10) evaluated the effect of goniotomy extent in patients with POAG undergoing 120°, 240°, and 360° procedures and reported comparable surgical success among groups, suggesting that a 120° goniotomy may be sufficient. Other studies have suggested that beyond approximately 120° of TM incision or excision, a plateau effect is reached, with no additional improvement in aqueous outflow or IOP reduction(13). In our study, patients who underwent 120°-180° trabeculotomy showed similar IOP reduction and surgical success compared with the other groups at 12 months. Taken together with the current literature, these findings suggest that trabeculotomy of 120° or greater may be sufficient to achieve effective outcomes in GATT surgery.
However, other studies have reported that the extent of trabeculotomy may influence IOP reduction(7,14). Chin et al.(7), comparing conventional trabeculotomy (120°) with 360° ab externo trabeculotomy, reported significantly lower postoperative IOP and medication use at 12 months in the 360° group. However, in that study, differences in surgical technique—including viscoelastic injection into Schlemm’s canal and the use of different instruments for TM incision—may have introduced a combined effect resembling both trabeculotomy and viscocanalostomy, potentially contributing to IOP reduction independent of incision extent.
Consistent with this, Manabe et al.(8) reported no correlation between the extent of SC incision and IOP reduction at 12 months following ab externo suture trabeculotomy without viscoelastic injection into SC. They also found that extending the incision beyond 150° did not provide additional IOP-lowering benefit within the first postoperative year.
In our study, one possible explanation for the lack of differences in surgical success among the three groups at 12 months is that the TM and SC represent only a portion of the aqueous outflow system, and abnormalities in distal outflow pathways may influence the effect of trabeculotomy extent on IOP reduction. Thus, effective IOP reduction with limited SC incision may depend on the functional integrity of distal outflow pathways. Hann et al.(6), using 3D micro-CT imaging, emphasized that the aqueous outflow system should be considered a functional unit consisting of collector channels, adjacent SC, and surrounding TM tissue.
The absence of correlation between trabeculotomy extent and IOP reduction in our study may therefore be explained by the segmented and variable resistance characteristics of the aqueous outflow pathway. In addition, the nonuniform nature of aqueous outflow along the circumferential TM(15) may account for the similar IOP reductions observed in groups undergoing less than 360° trabeculotomy.
Previous studies have reported that the trabeculotomy cleft may narrow over time due to SC scarring, membrane formation, or anterior synechiae. In our study, although a difference in mean IOP was observed at 1 month between the 360° and 90°-180° groups, this difference was not maintained at later follow-ups, which may be related to these postoperative structural changes. Rao et al.(16), using anterior segment optical coherence tomography in early postoperative GATT patients (<2 months), demonstrated fibrotic closure of the trabecular shelf in the TM region, although most patients maintained surgical success. They suggested that a complete 360° opening may compensate for localized fibrotic closure. Given the 12-month follow-up in our study, longer trabeculotomy may theoretically maintain a more extensive functional outflow pathway, potentially influencing long-term outcomes.
The effect of combining GATT with cataract surgery on surgical outcomes remains controversial. Changes induced by cataract surgery in the ciliary body, zonules, and anterior chamber angle may influence SC patency and aqueous outflow independently of trabeculotomy extent. However, our regression analysis showed that combined surgery did not significantly affect surgical success at 12 months across different trabeculotomy groups. This is consistent with studies reporting no significant difference in IOP reduction with combined surgery, although some sstudies suggest that phacoemulsification combined with GATT yields favorable outcomes regardless of trabeculotomy extent(10,17).
The influence of glaucoma type on surgical outcomes is also debated. Some studies have reported similar success rates between POAG and pseudoexfoliation (PXF) glaucoma, whereas others have shown higher failure rates in POAG compared with secondary open-angle glaucoma(18,19). Grover et al.(20) reported a mean IOP reduction of 37.3% in POAG and 49.8% in secondary open-angle glaucoma at 24 months following 360° GATT. In our study, regression analysis showed that glaucoma type (POAG vs. PXF glaucoma) did not affect surgical success across different trabeculotomy extents.
The most common complications of GATT include transient hyphema and postoperative IOP spikes. The relationship between trabeculotomy extent and these complications remains unclear. In our study, no significant differences were observed among groups in terms of hyphema or IOP spikes. Rao et al. reported that incomplete trabeculotomy may contribute to postoperative IOP elevation, whereas Ruparelia et al. suggested hemispheric GATT (hemi-GATT) as a strategy to reduce hyphema and associated IOP spikes(16,21). They reported transient hyphema in 25.9% of hemi-GATT cases, which was lower than rates observed with 360° surgery(21). Sato et al.(11) reported higher hyphema rates in the 360° group compared with the inferior 180° group, although no significant effect on IOP spikes was observed. Manabe et al.(8) found no significant association between incision extent and IOP spikes but reported a positive correlation between incision extent and hyphema severity on postoperative day 1. While longer incisions in the SC may theoretically increase blood reflux, discrepancies in the literature may be explained by variations in intraoperative techniques.
Beyond the extent, several other surgical and postoperative factors may influence IOP reduction after GATT. These include differences in technique (microcatheter-assisted versus suture-assisted trabeculotomy), use of ab externo approaches, and viscoelastic injection into Schlemm’s canal, as well as postoperative variables such as pilocarpine use, steroid regimens, and residual viscoelastic, all of which may affect aqueous outflow dynamics(8,22,23). However, the present study focused exclusively on trabeculotomy extent and did not evaluate the influence of these additional factors. Future comparative studies assessing surgical techniques and postoperative management strategies may provide a more comprehensive understanding of their relative effects on surgical outcomes.
This study has several limitations. Its retrospective design limits control over confounding variables and postoperative standardization. Another limitation is the relatively short follow-up period of 12 months, which may not capture long-term structural changes after trabeculotomy. Experimental studies have shown progressive healing of the trabeculotomy cleft, with loss of communication between the anterior chamber and Schlemm’s canal within 1 year(24). Histological studies have also demonstrated reapproximation of the trabecular flap due to fibrosis and tissue remodeling(25). Long-term imaging studies using gonioscopy and anterior segment optical coherence tomography (AS-OCT) have further shown that trabeculotomy clefts may narrow or close in certain sectors over time, while remaining patent in others(26). Our findings also suggest that trabeculotomy patency is a dynamic process that may continue to evolve beyond the first postoperative year. Therefore, a 12-month follow-up may be insufficient to fully capture long-term anatomical changes that could modify the relationship between trabeculotomy extent and surgical success. Prospective studies with extended follow-up and serial imaging would be valuable to clarify these long-term effects.
The inclusion of both standalone GATT and combined GATT with phacoemulsification cases represents another limitation; however, the similar distribution of combined procedures across groups likely minimizes its impact on comparative outcomes. In addition, although episcleral venous wave morphology provides relevant information regarding distal outflow function(27), the optimal clinical method for evaluating this system remains limited. Due to the retrospective nature of this study, distal outflow pathways could not be directly assessed.
Finally, the extent of trabeculotomy was analyzed independently of incision location. While some variability in regional outflow contribution has been proposed, recent studies suggest that surgical efficacy is not significantly influenced by the anatomical location of the trabeculotomy site(11,19).
From a clinical perspective, our findings suggest that achieving a complete 360° trabeculotomy may not be necessary in all cases. In situations where anatomical constraints, intraoperative resistance, or safety considerations limit full cannulation, partial trabeculotomy (≥120°-180°) may still provide comparable IOP reduction within the first postoperative year. This may be particularly relevant in eyes with prior inflammation, angle synechiae, or Schlemm’s canal narrowing, where forcing complete cannulation may increase complication risk. These results support a more individualized surgical approach based on intraoperative findings rather than a fixed target of 360°.
In conclusion, variations in trabeculotomy extent do not appear to influence surgical success at 12 months. Although early postoperative IOP reduction may differ from complete 360° trabeculotomy, achieving optimal outcomes within 12 months may not require a full circumferential incision.
AUTHORS’ CONTRIBUTIONS:
Significant contribution to conception and design: Berire Şeyma Durmuş Ece, Erdem Yüksel. Data Acquisition: Berire Şeyma Durmuş Ece, Erdem Yüksel. Data Analysis and Interpretation: Berire Şeyma Durmuş Ece, Erdem Yüksel. Manuscript Drafting: Berire Şeyma Durmuş Ece. Significant intellectual content revision of the manuscript: Erdem Yüksel. Final approval of the submitted manuscript: Berire Şeyma Durmuş Ece, Erdem Yüksel. Statistical analysis: Berire Şeyma Durmuş Ece Obtaining funding: not applicable. Supervision of administrative, technical, or material support: Erdem Yüksel. Research group leadership: Erdem Yüksel.
REFERENCES
1. Grover DS, Godfrey DG, Smith O, Feuer WJ, Montes de Oca I, Fellman RL. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: technique report and preliminary results. Ophthalmology. 2014;121(4):855-61.
2. Wang Y, Wang H, Han Y, Shi Y, Xin C, Yin P, et al. Outcomes of gonioscopy-assisted transluminal trabeculotomy in juvenile-onset primary open-angle glaucoma. Eye (Lond). 2021;35(10):2848-54.
3. Chen RI, Purgert R, Eisengart J. Gonioscopy-assisted transluminal trabeculotomy and goniotomy, with or without concomitant cataract extraction, in steroid-induced and uveitic glaucoma: 24-month outcomes. J Glaucoma. 2023;32(6):501-10.
4. Aktas Z, Ozmen MC, Ozdemir Zeydanli E, Oral M, Eskalen O. Efficacy and safety of gonioscopy-assisted transluminal trabeculotomy for primary congenital glaucoma. J Glaucoma. 2023;32(6):497-500.
5. Grant WM. Experimental aqueous perfusion in enucleated human eyes. Arch Ophthalmol (Chicago, Ill 1960). 1963;69(6):783-801.
6. Hann CR, Bentley MD, Vercnocke A, Ritman EL, Fautsch MP. Imaging the aqueous humor outflow pathway in human eyes by three-dimensional micro-computed tomography (3D micro-CT). Exp Eye Res. 2011;92(2):104-11.
7. Chin S, Nitta T, Shinmei Y, Aoyagi M, Nitta A, Ohno S, et al. Reduction of intraocular pressure using a modified 360-degree suture trabeculotomy technique in primary and secondary open-angle glaucoma: a pilot study. J Glaucoma. 2012;21(6):401-7.
8. Manabe SI, Sawaguchi S, Hayashi K. The effect of the extent of the incision in the Schlemm canal on the surgical outcomes of suture trabeculotomy for open-angle glaucoma. Jpn J Ophthalmol. 2017;61(1):99-104.
9. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142.
10. Zhang Y, Yu P, Zhang Y, Sugihara K, Zhu X, Zhang Y, et al.; PVP Study Group. Influence of goniotomy size on treatment safety and efficacy for primary open-angle glaucoma: a multicenter study. Am J Ophthalmol. 2023;256:118-25.
11. Sato T, Kawaji T. 12-month randomised trial of 360° and 180° Schlemm’s canal incisions in suture trabeculotomy ab interno for open-angle glaucoma. Br J Ophthalmol. 2021;105(8):1094-8.
12. Rosenquist R, Epstein D, Melamed S, Johnson M, Grant WM. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr Eye Res. 1989;8(12):1233-40.
13. Hirabayashi MT, Lee D, King JT, Thomsen S, An JA. Comparison of surgical outcomes of 360° circumferential trabeculotomy versus sectoral excisional goniotomy with the Kahook dual blade at 6 months. Clin Ophthalmol. 2019;13:2017-24.
14. Lim ME, Neely DE, Wang J, Haider KM, Smith HA, Plager DA. Comparison of 360-degree versus traditional trabeculotomy in pediatric glaucoma. J AAPOS. 2015;19(2):145-9.
15. Overby DR, Stamer WD, Johnson M. The changing paradigm of outflow resistance generation: towards synergistic models of the JCT and inner wall endothelium. Exp Eye Res. 2009;88(4):656-70.
16. Rao A, Khan SM, Mukherjee S. Causes of immediate and early IOP spikes after circumferential gonioscopy-assisted transluminal trabeculotomy using ASOCT. Clin Ophthalmol. 2023;17:313-20.
17. Takata M, Ishikawa H, Ikeda T, Gomi F. Conventional trabeculotomy versus gonioscopy-assisted transluminal trabeculotomy: a retrospective cohort study. J Clin Med. 2021;11(1):46.
18. Bektas C, Aktas Z, Ucgul AY, Karamert SS. Prognostic factors affecting the surgical success of gonioscopy-assisted transluminal trabeculotomy. Indian J Ophthalmol. 2021;69(6):1425-9.
19. Waldner DM, Chaban Y, Penny MD, Al-Ani A, Belkin A, Ahmed II, et al. Segmental suture gonioscopy-assisted transluminal trabeculotomy: comparison of superior versus inferior hemisphere outcomes. J Glaucoma. 2023;32(5):396-406.
20. Grover DS, Smith O, Fellman RL, Godfrey DG, Gupta A, Montes de Oca I, et al. Gonioscopy-assisted transluminal trabeculotomy: an ab interno circumferential trabeculotomy: 24 months follow-up. J Glaucoma. 2018;27(5):393-401.
21. Ruparelia S, Wilson D, Shoham-Hazon N. Hemi-GATT combined with phacoemulsification in patients with moderate-severe primary open-angle glaucoma: 2-year outcomes. Graefes Arch Clin Exp Ophthalmol. 2023;261(11):3257-62.
22. Otori Y, Matsuoka T, Kumoi M, Tachibana E, Tsujino C, Matsuda S. Comparison of surgical outcomes between ab interno suture trabeculotomy and ab externo metal trabeculotomy in adult patients with glaucoma. Clin Ophthalmol. 2021;15:3213-20.
23. Espinoza G, Gómez LM, Rodríguez-Una I, Duarte-Bueno LM, Parra JC, Serrano-Gómez S. effect of postoperative pilocarpine eyedrops in the outcomes of gonioscopy-assisted transluminal trabeculotomy surgery. J Glaucoma. 2025;34(8):610-5.
24. Ito S, Nishikawa M, Tokura T, Yamane A, Yamagishi K, Miki H. [Histopathological study of trabecular meshwork after trabeculotomy in monkeys]. Nippon Ganka Gakkai Zasshi. 1994;98(9):811-9. Japanese.
25. Amari Y, Hamanaka T, Futa R. Pathologic investigation failure of trabeculotomy. J Glaucoma. 2015;24(4):316-22.
26. Alagoz N, Cakir I, Altan C, Bozkurt E, Ipekli Z, Erdoğdu E, et al. Long-term structural changes observed on gonioscopy and anterior-segment OCT following gonioscopy-assisted transluminal trabeculotomy. Beyoglu Eye J. 2024;9(3):120-7.
27. Fellman RL, Grover DS. Episcleral venous fluid wave in the living human eye adjacent to microinvasive glaucoma surgery (MIGS) supports laboratory research: outflow is limited circumferentially, conserved distally, and favored inferonasally. J Glaucoma. 2019;28(2):139-45.
Data Availability Statement: The datasets produced and/or analyzed in this study can be provided to referees upon request.
Edited by
Editor-in-Chief: Newton Kara-Júnior
Associate Editor: Tiago Prata
Submitted for publication:
August 25, 2025.
Accepted for publication:
March 26, 2026.
Approved by the following research ethics committee: Kastamonu University Faculty of Medicine (Approval No. 2023-KAEK-81/05.07.2023).
Funding: This study received no specific financial support.
Disclosure of potential conflicts of interest: The authors declare no potential conflicts of interest.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.