Arq. Bras. Oftalmol. 2013; 76 (6): 10.1590/S0004-27492013000600010
Total: 1509
Luci Meire Pereira da Silva1; Cristina Muccioli2; Filipe de Oliveira2; Tiago Eugênio Arantes3; Lucas Renó Gonzaga4; Célia Regina Nakanami5
DOI: 10.1590/S0004-27492013000600010
ABSTRACT
PURPOSE: To identify the frequency and causes of uveitis leading to visual impairment in patients referred to the Low Vision Service - Department of Ophthalmology - UNIFESP, over a twenty years period. METHODS: In a retrospective study, medical records of 5,461 patients were reviewed. Data from the first clinical evaluation at the Low Vision Service were collected, patient's age, gender and cause of visual impairment were analyzed. Patients with uveitis had their chart reviewed for anatomical classification and clinical diagnosis. RESULTS: The mean age of the patients referred to the Low Vision Service was 42.86 years and the mean age of patients with uveitis diagnosis was 25.51 years. Retinal disorders were the most common cause of visual impairment (N=2,835 patients; 51.9%) followed by uveitis (862 patients, 15.7%). Uveitis was posterior in 792 patients (91.9% of uveitis) and toxoplasmosis was the most common diagnosis (765 patients, 88.7%). CONCLUSIONS: In our study, uveitis represents the second cause of visual impairment in patients referred for visual rehabilitation and toxoplasmic retinochoroiditis was the most common clinical diagnosis. It affects a young working age population with a relevant social and economic impact, but the early diagnosis and treatment can improve the quality of life of these patients.
Keywords: Visually impairment person; Low vision; Intraocular inflammation; Uveitis
RESUMO
OBJETIVO: Identificar a frequência e as causas de uveítes que resultam em deficiência visual, em pacientes encaminhados ao Serviço de Visão Sub-Normal do Departamento de Oftalmologia - UNIFESP, durante um período de 20 anos. MÉTODOS: Em um estudo retrospectivo foram revisados 5.461 prontuários. Foram coletados os dados da primeira avaliação clínica realizada no Setor de Visão Sub-Normal, que inclui idade do paciente, sexo e a causa da deficiência visual. Os registros clínicos dos pacientes com diagnóstico de uveíte foram revisados para classificação anatômica e diagnóstico. RESULTADOS: A média de idade dos pacientes encaminhados para o Setor de Visão Sub-Normal foi de 42.86 anos e a média de idade dos pacientes com diagnóstico de uveíte foi de 25.51 anos. As doenças retinianas foram as causas mais comuns de deficiência visual (N=2.835 pacientes; 51.9%), seguida por uveítes (N=862 pacientes, 15.7%). Foi observado uveíte posterior em 792 pacientes (91.9% dos casos de uveíte) e, dentre estes, toxoplasmose foi o diagnóstico mais comum (765 pacientes, 88.7%). CONCLUSÕES: Em nosso estudo, uveíte representa a segunda causa de deficiência visual nos pacientes encaminhados para reabilitação visual e retinocoroidite por toxoplasmose foi o diagnóstico clínico mais comum. Uveíte afeta uma população jovem e em idade laboral, portanto com relevante impacto social e econômico, mas o diagnóstico e tratamento precoce podem melhorar a qualidade de vida destes pacientes.
Descritores: Pessoas com deficiência visual; Baixa de visão; Inflamação intraocular; Uveíte
ORIGINAL ARTICLE
Visual impairment from uveitis in a reference hospital of Southeast Brazil: a retrospective review over a twenty years period
Deficiência visual em uveítes em hospital de referência da região sudeste do Brasil: uma revisão retrospectiva de 20 anos
Luci Meire Pereira da SilvaI; Cristina MuccioliII; Filipe de OliveiraII; Tiago Eugênio ArantesIII; Lucas Renó GonzagaIV; Célia Regina NakanamiV
IClinical Research, Department of Ophthalmology, Universidade Federal de São Paulo - UNIFESP, São Paulo (SP), Brazil
IIPhysician, Department of Ophthalmology, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil
IIIPhysician, Uveitis Section, Department of Ophthalmology, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil
IVAcademic of Medical Course, Escola Paulista de Medicina, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil
VPhysician, Low Vision Service, Department of Ophthalmology, Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil
ABSTRACT
PURPOSE: To identify the frequency and causes of uveitis leading to visual impairment in patients referred to the Low Vision Service - Department of Ophthalmology - UNIFESP, over a twenty years period.
METHODS: In a retrospective study, medical records of 5,461 patients were reviewed. Data from the first clinical evaluation at the Low Vision Service were collected, patient's age, gender and cause of visual impairment were analyzed. Patients with uveitis had their chart reviewed for anatomical classification and clinical diagnosis.
RESULTS: The mean age of the patients referred to the Low Vision Service was 42.86 years and the mean age of patients with uveitis diagnosis was 25.51 years. Retinal disorders were the most common cause of visual impairment (N=2,835 patients; 51.9%) followed by uveitis (862 patients, 15.7%). Uveitis was posterior in 792 patients (91.9% of uveitis) and toxoplasmosis was the most common diagnosis (765 patients, 88.7%).
CONCLUSIONS: In our study, uveitis represents the second cause of visual impairment in patients referred for visual rehabilitation and toxoplasmic retinochoroiditis was the most common clinical diagnosis. It affects a young working age population with a relevant social and economic impact, but the early diagnosis and treatment can improve the quality of life of these patients.
Keywords: Visually impairment person; Low vision; Intraocular inflammation; Uveitis/epidemiology
RESUMO
OBJETIVO: Identificar a frequência e as causas de uveítes que resultam em deficiência visual, em pacientes encaminhados ao Serviço de Visão Sub-Normal do Departamento de Oftalmologia - UNIFESP, durante um período de 20 anos.
MÉTODOS: Em um estudo retrospectivo foram revisados 5.461 prontuários. Foram coletados os dados da primeira avaliação clínica realizada no Setor de Visão Sub-Normal, que inclui idade do paciente, sexo e a causa da deficiência visual. Os registros clínicos dos pacientes com diagnóstico de uveíte foram revisados para classificação anatômica e diagnóstico.
RESULTADOS: A média de idade dos pacientes encaminhados para o Setor de Visão Sub-Normal foi de 42.86 anos e a média de idade dos pacientes com diagnóstico de uveíte foi de 25.51 anos. As doenças retinianas foram as causas mais comuns de deficiência visual (N=2.835 pacientes; 51.9%), seguida por uveítes (N=862 pacientes, 15.7%). Foi observado uveíte posterior em 792 pacientes (91.9% dos casos de uveíte) e, dentre estes, toxoplasmose foi o diagnóstico mais comum (765 pacientes, 88.7%).
CONCLUSÕES: Em nosso estudo, uveíte representa a segunda causa de deficiência visual nos pacientes encaminhados para reabilitação visual e retinocoroidite por toxoplasmose foi o diagnóstico clínico mais comum. Uveíte afeta uma população jovem e em idade laboral, portanto com relevante impacto social e econômico, mas o diagnóstico e tratamento precoce podem melhorar a qualidade de vida destes pacientes.
Descritores: Pessoas com deficiência visual; Baixa de visão; Inflamação intraocular; Uveíte /epidemiologia
INTRODUCTION
Visual impairment affects more than 161 million people worldwide. Current data derived from recent studies shows that 37 million were blind and 124 million people present with low vision, excluding those visually impaired due to uncorrected refractive errors(1,2). Taking into account the population growth and increased life expectancy there would be 76 million blind people by 2020, if attention does not improve(3).
Uveitis consists of a large group of diseases characterized by intraocular inflammation involving the uveal tract and has become increasingly recognized as one of the major cause of treatable blindness and ocular morbidity worldwide, especially in the working-age population. It is a potentially blinding disorder accounting for 10-15% of all cases of total blindness in United States and up to 20% of legal blindness. Uveitis and its complications are even more common in the developing world accounting for up to 25% of all causes of blindness(4-11).
More than half of all patients with uveitis develop complications related to their disease, and up to 35% of patients end up with severe visual impairment. Most of the studies do not consider uveitis as a cause of visual loss, but functional and anatomic complications secondary to uveitis are described as causes of visual impairment. In a hospital based survey of blindness in West Africa, in which these sequelae were correctly attributed to uveitis, this disease was the second leading cause of blindness(6-8). Glaucoma, retinal detachment, cataract as well as macular scar are described as the most frequent causes of visual impairment in uveitic patients.
Ocular toxoplasmosis, characterized by exudative retinochoroidal lesion and macular scars, is the most common cause of posterior uveitis in several countries and represents 60-85% of the posterior uveitis cases in Brazil and 25% in the United States and France. When compared to Europe and North America, Brazil has a disproportionately high incidence and severity of ocular toxoplasmosis(11-14).
The purpose of the present study was to identify the frequency and causes of uveitis leading to visual impairment in patients referred to the Low Vision Service of the Department of Ophthalmology Federal University of São Paulo, over a twenty year period.
METHODS
A retrospective study was conducted in the Department of Ophthalmology - Federal University of São Paulo (UNIFESP) and approved by the Institutional Review Board (IRB). Medical records of 461 patients referred to the Low Vision Service over a twenty year period were reviewed. The data from the first clinical evaluation performed at the Low Vision Service were collected and included age, gender and diagnosis. All patients referred to this Service presented visual impairment, classified according to the World Health Organization (WHO), as a person who has impairment of visual functioning even after treatment and/or standard refractive correction, and has a visual acuity of less than 6/18 to light perception, or a visual field less than 10 degrees from the point of fixation. WHO has published the term low vision as moderated visual impairment combined with severe visual impairment and both are according to the International Classification of Diseases - 10(15). According to the Low Vision Service requirements, all patients have had attended to these criteria to be evaluated by this service.
Patients seen from October 1987 to November 2007 were included in this study. Patients with uveitis had their chart reviewed for anatomical classification and clinical diagnosis. The classification criteria for uveitis were those defined by the International Uveitis Study Group(16).
The distribution of continuous variables was expressed as mean ± standard deviation (SD) and categorical data were presented as absolute and relative frequencies. Relationships between two categorical variables were assessed using Chi square test. Student t test and ANOVA were used for analysis of continuous variables. The statistical package SPSS 16.0 for Windows (SPSS, Inc, Chicago, Illinois, USA) was used in the analysis of the data.
RESULTS
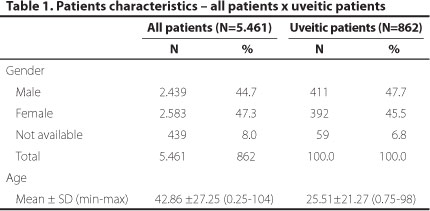
A total of 5.461 patient´s charts were reviewed; the mean age of the group including all low vision patients was 42.86 years (range from 0.25 to 104 years - SD 27.25). Patients with uveitis showed a mean age of 25.51 (range from 0.75 to 98 years - SD 21.17). The difference between gender was not statistically significant. Patient's characteristics in both groups are summarized in table 1.
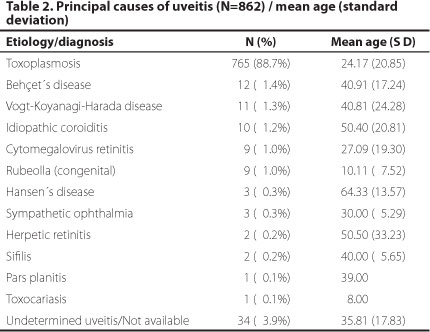
Uveitis was the second most common cause of visual impairment (862 patients; 15.8%) and toxoplasmosis was the most frequent clinical diagnosis in the uveitic group (765 cases; 88.7%), followed by Behçet disease (12 cases; 1.4%), Vogt-Koyanagi-Harada disease (11 cases; 1.3%), idiopathic choroiditis (10 cases; 1.2%), cytomegalovirus retinitis (9 cases; 1.0%), rubella (9 cases; 1.0%), Hansen´s disease (3 cases; 0.3%), sympathetic ophthalmia (3 cases; 0.3%), herpetic retinitis (2 cases; 0.2%), syphilis (2 cases; 0.2%), pars planitis (1 case; 0.1%) and toxocariasis (1 case; 0.1%). Thirty four patients (3.9%) had uveitis of undetermined etiology and/or unavailable classification, as seen in the table 2.
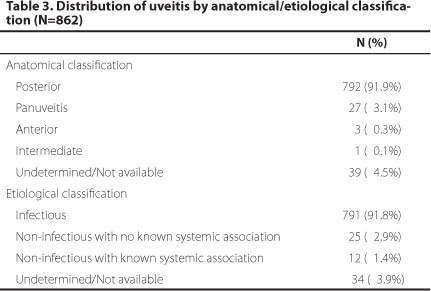
According to the anatomical classification we found 792 (91.9%) posterior uveitis, 27 (3.1%) panuveitis, 3 (0.3%) anterior uveitis, 1 (0.1%) intermediate uveitis and 39 (4.5%) undetermined and/or not available classification. According to the etiological classification, 791 (91.8%) were infectious uveitis, 25 (2.9%) non-infectious uveitis, 12 (1.4%) non-infectious associated with systemic disease and 34 (3.9%) undetermined uveitis and/or not available classification, as seen in the table 3.
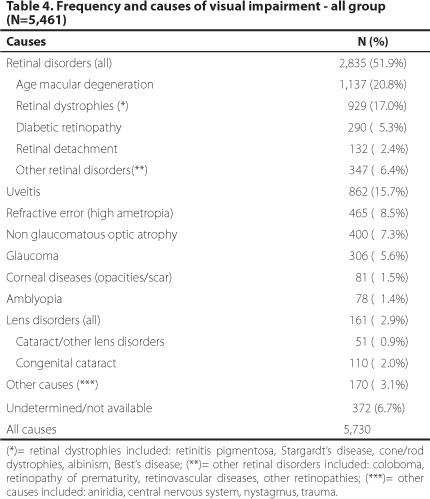
The frequency and distribution of visual impairment causes found from the 5.461 patients are presented in the table 4. Two hundred and sixty nine patients presented more than one cause of visual impairment, thus the total for the causes exceeds the overall of patients. The main causes of visual impairment were: retinal disorders (51.9%), uveitis (15.7%), refractive error (8.5%), optic atrophy (7.3%) and glaucoma (5.6%).
DISCUSSION
We conducted an institutional-based retrospective study on 5.461 medical charts of patients referred to the Low Vision Service of the Department of Ophthalmology - Federal University of São Paulo. We analyzed the characteristics of uveitis cases as well as its frequency in this population.
The patients referred to the Low Vision Service are those that require visual rehabilitation and training due to their impaired vision. The lack of visual acuity data does not prevent our goal that was to identify the frequency of visual impairment secondary to uveitis. This retrospective review is limited to the data from the first visit at the Low Vision Service, this study did not allow the clinical evaluation after the treatment and the visual prognosis.
A relatively equal distribution of male and female patients was observed in our uveitic group, as showed in most studies of different countries(11). In studies that report a gender difference, a male predominance is more common in studies from developing countries. In studies from India was observed a male predominance higher than 60%, but the reasons for this are unclear and may involve exposure patterns in agricultural societies or differences in the propensity to seek medical care. In the other hand, uveitis disorders affect men and women differently, and to analyze gender discrepancies are undoubtedly complex(11,17-21).
Considering anatomic distribution, posterior uveitis was the most common with 792 cases (91,9%), being ocular toxoplasmosis the most common cause of uveitis (88.7%). As showed by London et al.(11) posterior uveitis is more common in the developing world due to a high prevalence of infectious causes, such as toxoplasmosis in Brazil, tuberculosis in India and onchocerciasis in Africa(10,14,20,22,23). Although limited data on the epidemiology of uveitis are available from Latin America, toxoplasmosis is considered to be the most frequent cause of posterior uveitis in most studies and an unusually high prevalence is reported in southern Brazil, probably related to genetic predisposition, cultural factors such as agriculture-based economies and dietary habits(11-14).
Our study revealed a frequency of posterior uveitis higher than in the studies reviewed by London et al.(11), but it is supported by Brazilian studies that showed uveitis as a main diagnosis observed in patients who are treated on visual rehabilitation clinics(24,25). Also being a tertiary referral centre, more patients are likely to suffer from severe visual impairment secondary to uveitis. In addition, as already reported by Rothova et al.(6), ocular toxoplasmosis was the most frequent cause of both unilateral legal blindness and unilateral visual impairment.
We found in the uveitic population a mean age of 25.51 years, characterizing a young working age population, this is supported by many others studies(7,8,10-14,24-27). With a majority of the patients in the working age group, the potential social and economic costs are enormous but few data exist about visual morbidity caused by uveitis. The estimated cost of blindness to the United States economy from uveitis is equal to the cost of blindness from diabetes which incidence is twice as high as uveitis(7,28). A study by the Royal National Institute for the Blind suggested that 34% of individuals lose jobs within two years of visual impairment(29). Two studies based on the Blue Mountains Eye Study cohort found that although bilateral visual morbidity results in reduced functional status and wellbeing that is comparable to a major medical condition, visual loss also have a measurable impact on quality of life(30,31).
Considering the loss of reading ability is often considered to be the most devastating consequence of visual impairment in a young working age population, the development of rehabilitation tools is crucial to improve the vision of the uveitic patients. As found by Schmier et al., substantial differences exist in the use of services, devices, and caregiving needs across levels of visual impairment among patients with diabetic retinopathy(32).
A limitation of our study is that the visual acuity scores of each case were not collected, however according to the Low Vision Service requirements all patients have had attended the criteria a visual acuity of less than 6/18 to light perception, or a visual field less than 10 degrees from the point of fixation. Most of these cases underwent developing strategies to optimize residual vision, however the visual rehabilitation data was not analysed by this study.
CONCLUSION
In our study, uveitis represents the second cause of visual impairment among patients evaluated at the Low Vision Service of Department of Ophthalmology/São Paulo Hospital/UNIFESP. The most common causes of low vision were retinal disorders followed by uveitis, refractive errors, optic atrophy, glaucoma e other causes. Toxoplasmosis is the most common cause of visual impairment in the uveitic group.
Taking in account that uveitis affects a young working age population and shows a high prevalence in visual impaired patients, it should be considered as an important cause of visual loss with a relevant social and economic impact, but the early diagnosis and treatment can improve the quality of life of these patients.
REFERENCES
1. Resnikoff S, Pascolini D, Etya'ale D, Kocur I, Pararajasegaram R, Pokharel GP, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82(11):844-51.
2. Araujo Filho A, Salomão SR, Berezovsky A, Cinoto RW, Morales PH, Santos FR, et al. Prevalence of visual impairment, blindness, ocular disorders and cataract surgery outcomes in low-income elderly from a metropolitan region of São Paulo - Brazil. Arq Bras Oftalmol. 2008;71(2):246-53.
3. Frick KD, Foster A. The magnitude and cost of global blindness: an increasing problem that can be alleviated. Am J Ophthalmol. 2003;135(4):471-6.
4. Suttorp-Schulten MS, Rothova A. The possible impact of uveitis in blindness: a literature survey. Br J Ophthalmol. 1996;80(9):844-8.
5. Nussenblatt RB. The natural history of uveitis. Int Ophthalmol. 1990;14(5-6):303-8.
6. Rothova A, Suttorp-van Schulten MS, Frits Treffers W, Kijlstra A. Causes and frequency of blindness in patients with intraocular inflammatory disease. Br J Ophthalmol. 1996; 80(4):332-6.
7. Durrani OM, Therani NN, Moradi JE, Moradi P, Stavrou P, Murray PI. Degree, duration, and causes of visual loss in uveitis. Br J Ophthalmol. 2004;88(9):1159-62.
8. Ronday MJ, Stilma JS, Barbe RF, Kijlstra A, Rothova A. Blindness from uveitis in a hospital population in Serra Leone. Br J Ophthalmol. 1994;78(9):690-3.
9. de Boer J, Wulffraat N, Rothova A. Visual loss in uveitis of childhood. Br J Ophthalmol. 2003;87(7):879-84.
10. Dandona L, Dandona R, John RK, McCarty CA, Rao GN. Population based assessment of uveitis in an urban population in southern India. Br J Ophthalmol. 2000;84(7):706-9.
11. London NJ, Rathinam SR, Cunningham ET Jr. The epidemiology of uveitis in developing countries. Int Ophthalmol Clin. 2010;50(2):1-17.
12. Muccioli C, Belfort Jr R. Uveítes. São Paulo: Conselho Brasileiro de Oftalmologia; 2001.
13. Holland GN. Ocular toxoplasmosis: a global reassessment. Part I: epidemiology and course of disease. Am J Ophthalmol. 2003;136(6):973-88.
14. Glassner PD, Silveira C, Kruszon-Moran D, Martins MC, Burnier Júnior M, Silveira S, et al. An unusually high prevalence of ocular toxoplasmosis in southern Brazil. Am J Ophthalmol. 1992;114(2):136-44.
15. World Health Organization. Visual impairment and blindness . WHO Fact Sheet, #282, June, 2012. Available from: <http:www.who.int/mediacentre/factsheets/fs282/en/>. Accessed 2012 Oct 04.
16. Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509-16.
17. Das D, Bhattacharjee H, Bhattacharyya PK, Jain L, Panicker MJ, Das K, et al. Pattern of uveitis in North East India: a tertiary eye care center study. Indian J Ophthalmol. 2009;57(2):144-6.
18. Rathinam SR, Namperumalsamy P. Global variation and pattern changes in epidemiology of uveitis. Indian J Ophthalmol. 2007;55(3):173-83.
19. Biswas J, Narain S, Das D, Ganesh SK. Pattern of uveitis in a referral uveitis clinic in India. Int Ophthalmol. 1996-1997;20(4):223-8. Comment in Indian J Ophthalmol. 2004;52(4):345-6; author reply 346-7.
20. Das D, Biswas J, Ganesh SK. Pattern of uveitis in referral uveitis clinic in India. Indian J Ophthalmol. 1995;43(3):117-21. Erratum in Indian J Ophthalmol. 1995;43(4):176.
21. Consul BN, Sharma DP, Chhabra HN, Sahai R. Uveitis: etiological pattern in India. Eye Ear Nose Throat Mon. 1972;51(3):122-7.
22. Singh R, Gupta V, Gupta A. Pattern of uveitis in a referral eye clinic in north India. Indian J Ophtalmol. 2004;52(2):121-5. Comment in Indian J Ophthalmol. 2004;52(4):346; author reply 346-7.
23. Kaimbo Wa Kimbo D, Bifuko A, Dernouchamps JP, Missotten L. Chronic uveitis in Kinshasa (D R Congo). Bull Soc Belge Ophtalmol. 1998;270:95-100.
24. Kara José N, Carvalho KM, Pereira VL, Venturini NH, Gasparetto ME, Gushiken MT. Estudo retrospectivo dos primeiros 140 casos atendidos na clínica de visão sub-normal do Hospital de Clínicas da Unicamp. Arq Bras Oftalmol. 1988;51(2):65-9.
25. Gouveia EB, Yamamoto JH, Abdalla M, Hirata CE, Kubo P, Olivalves E. Causas das uveítes em serviço terciário em São Paulo, Brasil. Arq Bras Oftalmol. 2004;67(1):139-45.
26. Fernandes LC, Oréfice F. Aspectos clínicos e epidemiológicos das uveítes em serviços de referência em Belo Horizonte, de 1970 a 1993: parte I. Rev Bras Oftalmol. 1996;55(8):569-78.
27. Abreu MT, Hirata PS, Belfort Jr R, Domingues Neto S. Uveítes em São Paulo: estudo epidemiológico, clínico e terapêutico. Arq Bras Oftalmol. 1980;43:10-6
28. ten Doesschate J. Causes of blindness in The Netherlands. Doc Ophthalmol. 1982; 52(3-4):270-85.
29. Bruce I, McKennel A, Walker E. Blind and partially sighted adults in Britain: the RNIB survey. London: HMSO; 1991.
30. Chia EM, Mitchell P, Rochtchina E, Foran S, Wang JJ. Unilateral visual impairment and health related quality of life: the Blue Mountains Eye Study. Br J Ophthalmol. 2003;87(4):392-5.
31. Chia EM, Wang JJ, Rochtchina E, Smith W, Cumming RR, Mitchell P. Impact of bilateral visual impairment on health-related quality of life: the Blue Mountains Eye Study. Invest Ophthalmol Vis Sci. 2004;45(1):71-6.
32. Schmier JK, Covert DW, Matthews GP, Zakov ZN. Impact of visual impairment on service and device use by individuals with diabetic retinopathy. Disabil Rehabil. 2009; 31(8):659-65. .
 Correspondence:
Correspondence:
Luci Meire P. Silva
Rua Botucatu, 822 - 1o andar São Paulo (SP)
04023-062 - Brazil
E-mail: [email protected]
Submitted for publication: May 20, 2013
Accepted for publication: July 16, 2013
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: L.M.P.Silva, None; C.Muccioli, None; F.Oliveira, None; T.E.Arantes, None; L.R.Gonzaga, None; C.R.Nakanami, None.
Study carried out Universidade Federal de São Paulo - UNIFESP - São Paulo (SP), Brazil.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.