Arq. Bras. Oftalmol. 2013; 76 (1): 10.1590/S0004-27492013000100012
Total: 2808
Heloisa Andrade Maestrini1; Angela Andrade Maestrini2; Danuza de Oliveira Machado3; Daniel Vitor Vasconcelos Santos4; Homero Gusmão de Almeida4
DOI: 10.1590/S0004-27492013000100012
ABSTRACT
Bilateral acute depigmentation of the iris (BADI) is a recently described entity characterized by acute onset of pigment dispersion in the anterior chamber, depigmentation of the iris, and heavy pigment deposition in the anterior chamber angle. Involvement is always bilateral, simultaneous, and symmetrical. We report the case of a 61-year-old man who presented with bilateral ocular pain, red eyes, and severe photophobia. Examination revealed a dense Krukenberg spindle, heavy pigment dispersion in the anterior chamber, extensive transillumination iris defects, and a heavy pigment deposition in the trabecular meshwork bilaterally. Intraocular pressure increased to 48 mmHg in both eyes. The patient received topical steroids, maximum hypotensive treatment and oral valacyclovir. Intraocular pressure gradually decreased throughout the second and third months, and medications were gradually tapered. The time to complete resolution of pigment dispersion was 18 weeks. Visual acuity and visual fields remained normal, but the photophobia was permanent.
Keywords: Iris diseases; Acute disease, Transillumination; Intraocular pressure; Gonioscopy; Pigment epithelium of eye; Case reports; Humans; Male; Middle age
RESUMO
Despigmentação aguda bilateral da íris (BADI) é uma nova doença caracterizada pela despigmentação aguda da íris, dispersão de pigmentos na câmara anterior e intensa deposição de pigmentos no seio camerular. O acometimento é sempre bilateral, simultâneo e simétrico. Relatamos o caso de um paciente de 61 anos, com dor ocular bilateral aguda, hiperemia e intensa fotofobia. Ao exame, apresentava denso fuso de Krukenberg, importante dispersão de pigmentos na câmara anterior, extensos defeitos à transiluminação iriana e densa deposição de pigmentos no seio camerular em ambos os olhos. O paciente recebeu corticoide tópico, terapia hipotensora máxima e valacyclovir oral. A pressão intraocular chegou a 48 mmHg em ambos os olhos mas foi reduzindo gradativamente ao longo do segundo e terceiro meses, permitindo a suspensão gradativa da medicação. A resolução completa da dispersão pigmentar demorou 18 semanas. A acuidade e os campos visuais permaneceram normais, mas o paciente manteve a fotofobia.
Descritores: Doenças da íris, Doença aguda; Transiluminação; Pressão intraocular; Gonioscopia; Epitélio pigmentado ocular; Relatos de casos; Humanos; Masculino; Meia-idade
CASE REPORT RELATO DE CASO
Bilateral acute depigmentation of the iris (BADI): first reported case in Brazil
Despigmentação aguda bilateral da íris (BADI): primeiro relato de caso no Brasil
Heloisa Andrade MaestriniI; Angela Andrade MaestriniII; Danuza de Oliveira MachadoIII; Daniel Vitor Vasconcelos SantosIV; Homero Gusmão de AlmeidaIV
IPhysician, Glaucoma Service, Oculare Ophthalmology Center, Belo Horizonte, Brazil
IIPhysician, Retina and Cataract Services, Oculare Ophthtalmology Center, Belo Horizonte (MG), Brazil
IIIPhysician, Uveitis Service, Department of Ophthalmology, Universidade Federal de Minas Gerais - UFMG - Belo Horizonte (MG), Brazil
IVPhysician, Department of Ophthalmology, Universidade Federal de Minas Gerais - UFMG - Belo Horizonte (MG), Brazil
ABSTRACT
Bilateral acute depigmentation of the iris (BADI) is a recently described entity characterized by acute onset of pigment dispersion in the anterior chamber, depigmentation of the iris, and heavy pigment deposition in the anterior chamber angle. Involvement is always bilateral, simultaneous, and symmetrical. We report the case of a 61-year-old man who presented with bilateral ocular pain, red eyes, and severe photophobia. Examination revealed a dense Krukenberg spindle, heavy pigment dispersion in the anterior chamber, extensive transillumination iris defects, and a heavy pigment deposition in the trabecular meshwork bilaterally. Intraocular pressure increased to 48 mmHg in both eyes. The patient received topical steroids, maximum hypotensive treatment and oral valacyclovir. Intraocular pressure gradually decreased throughout the second and third months, and medications were gradually tapered. The time to complete resolution of pigment dispersion was 18 weeks. Visual acuity and visual fields remained normal, but the photophobia was permanent.
Keywords: Iris diseases; Acute disease, Transillumination; Intraocular pressure; Gonioscopy; Pigment epithelium of eye; Case reports; Humans; Male; Middle age
RESUMO
Despigmentação aguda bilateral da íris (BADI) é uma nova doença caracterizada pela despigmentação aguda da íris, dispersão de pigmentos na câmara anterior e intensa deposição de pigmentos no seio camerular. O acometimento é sempre bilateral, simultâneo e simétrico. Relatamos o caso de um paciente de 61 anos, com dor ocular bilateral aguda, hiperemia e intensa fotofobia. Ao exame, apresentava denso fuso de Krukenberg, importante dispersão de pigmentos na câmara anterior, extensos defeitos à transiluminação iriana e densa deposição de pigmentos no seio camerular em ambos os olhos. O paciente recebeu corticoide tópico, terapia hipotensora máxima e valacyclovir oral. A pressão intraocular chegou a 48 mmHg em ambos os olhos mas foi reduzindo gradativamente ao longo do segundo e terceiro meses, permitindo a suspensão gradativa da medicação. A resolução completa da dispersão pigmentar demorou 18 semanas. A acuidade e os campos visuais permaneceram normais, mas o paciente manteve a fotofobia.
Descritores: Doenças da íris, Doença aguda; Transiluminação; Pressão intraocular; Gonioscopia; Epitélio pigmentado ocular; Relatos de casos; Humanos; Masculino; Meia-idade
INTRODUCTION
Bilateral acute depigmentation of the iris (BADI) is a recently described clinical entity(1) characterized by acute onset of pigment dispersion in the anterior chamber, depigmentation of the iris, and heavy pigment deposition in the anterior chamber angle. Involvement is always bilateral, simultaneous, and symmetrical. Clogging of the trabecular meshwork with pigment may cause an acute rise of intraocular pressure (IOP). Patients typically present with acute and usually severe photophobia, red eye, and ocular discomfort or pain, which sometimes simulates acute bilateral iridocyclitis. Cases often occur after a flulike illness or upper respiratory tract infection, some of them after the use of oral moxifloxacin(2-4). Middle-aged women are most commonly affected.
Two clinical sub-types have been described. In the first(1,5), pigment discharge originates in the iris stroma. Patients show a geographic or diffuse depigmentation of the iris and a change in iris texture and color without transillumination defects or pupil distortion. It often has a benign and short course. Increase in IOP is uncommon, and iris changes may be reversible. In the second and more severe sub-type, described as bilateral acute iris transillumination(6), pigment discharge originates in the iris pigment epithelium causing extensive and diffuse iris transillumination. Patients typically show an atonic, mydriatic, or distorted pupil and occasional posterior synechiae. An early and severe rise in IOP is common. Both sub-types have a self-limited course and a good prognosis. In the first sub-type, complete resolution of pigment discharge occurs after 8 to 16 weeks. In the second sub-type, complete resolution may take months or more than 1 year. The etiopathogenesis is unknown, but might be related to a viral infection.
Previous cases have been reported in Turkey(5,6) (51 cases), Netherlands(3,7) (4 cases), Belgium(3,4,6) (4 cases), Spain(2) (one case) and France(8) (one case). We describe the first reported case in the Southern Hemisphere. Informed consent was obtained from the patient. This case report was approved by the Ethical Committee/Investigational Review Board of the Federal University of Minas Gerais.
CASE REPORT
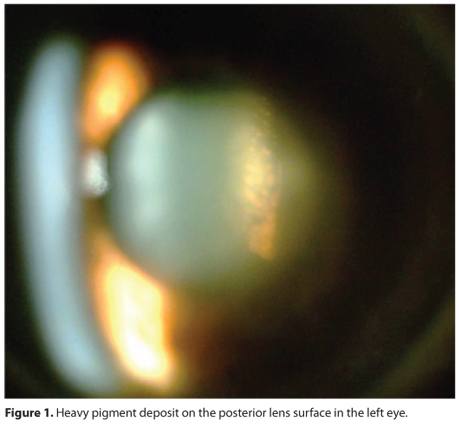
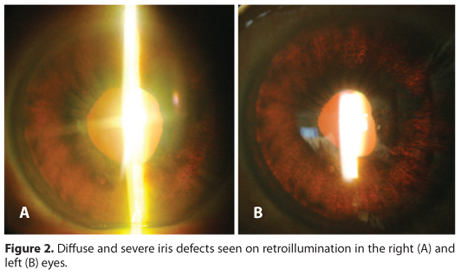
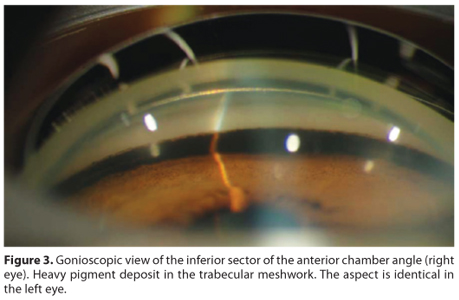
A 61-year-old man presented in July 2011 with acute onset of bilateral and simultaneous ocular pain, red eye, and severe photophobia. Visual acuity was 20/20 OU. Examination revealed 2+ pigmented cells in the anterior chamber and a slight deposition of pigment on the corneal endothelium. IOP was low (6/9 mmHg OD/OS). The initial diagnosis was bilateral anterior uveitis, and the patient was treated using a topical steroid (1% prednisolone every 3 hours) with marked relief of symptoms. However, on the fourth day, while playing "footvolley", his vision suddenly blurred. The next day, slit-lamp evaluation revealed a dense Krukenberg spindle bilaterally. The aqueous humor was turbid with heavy pigment dispersion in the anterior chamber. Pigment granules were deposited on the anterior surface of the iris and posterior lens surface (Figure 1). Transillumination showed extensive bilateral iris defects (Figure 2). IOP was 36/40 mmHg OD/OS. Gonioscopy revealed a wide open angle, a dark trabecular meshwork 360 degrees, and a heavy pigment deposition, particularly in the inferior sector (Figure 3). The vitreous was clear, the fundus was normal, and the optic nerve head cup-disc ratio was 0.1 bilaterally. Over the following days, IOP increased to 48 mmHg in both eyes. The pupil became progressively irregular with small posterior synechiae (Figure 4) and iris transillumination gradually increased. Corneal endothelial cell density was normal (2,877 cells/mm2 OD and 2,984 cells/mm2 OS).

Previous clinical and ocular histories were unremarkable, with the exception of a previous laser photocoagulation in the right eye to treat a peripheral retinal tear 1 year prior to BADI onset. IOP was normal at that time (10 mmHg bilaterally).
The patient underwent a complete laboratory evaluation, including complete blood count, erythrocyte sedimentation rate, liver enzymes, chest X-ray, anti-nuclear factor, rheumatoid factor, C-reactive protein, tuberculin skin test, blood and urinary calcium, angiotensin converting enzyme, and lysozyme. The results were unremarkable. Serological tests for toxoplasmosis, syphilis, herpes simplex virus (HSV) I and II, varicella-zoster virus, and cytomegalovirus (CMV) were performed. All IgM antibodies were negative. IgG antibodies were positive against toxoplasmosis, HSV I and II, varicella-zoster virus and CMV.
Prednisolone eye drops were administered every 3 hours and the maximum tolerated hypotensive treatment was instituted (timolol, brimonidine, and oral acetazolamide 750 mg/day), which lowered IOP to 25-30 mmHg bilaterally. Mydriasis always caused an acute rise in IOP up to 42 mmHg because of an increase in pigment discharge. Abrupt discontinuation of prednisolone resulted in immediate relapse. On day 28, empirical treatment with oral valacyclovir 3 g/day was introduced resulting in a significant reduction in pigment dispersion in a few days. After 3 weeks, the dose was reduced to 1,500 mg/day for 3 more weeks, and then to 500 mg/day for 8 weeks. Prednisolone was gradually tapered and completely discontinued after 18 weeks. IOP gradually decreased throughout the second and third months, and hypotensive medications were gradually tapered until discontinuation after 24 weeks. The time to complete resolution of pigment dispersion was 18 weeks. No cupping of the optic discs was observed; however, in the seventh week, a small disc hemorrhage appeared in the left eye. Visual acuity and visual fields remained normal; however, the photophobia was permanent. Six months after complete resolution, we performed a water drinking test and IOP remained at normal levels (IOP rose from 13 to 19 mmHg bilaterally). After 1 year, the patient developed bilateral cataracts, which were removed uneventfully. IOP was high on the first postoperative day (34/26 mmHg OD/OS), but returned to12 mmHg after 1 week.
DISCUSSION
BADI is a recently described and rare entity. Our patient presented with the more severe BADI sub-type showing a severe rise in IOP, extensive areas of iris transillumination, distorted pupils, and posterior synechiae, but no change in iris color.
Differential diagnosis includes herpetic iridocyclitis(9) (tipically unilateral), Fuchs' uveitis (bilateral in only 5-10% of cases), pigment dispersion syndrome, and pseudoexfoliation syndrome (do not have an acute onset).
Although the cause is not known, BADI shares some features of viral herpetic iridocyclitis. The marked improvement in our patient following valacyclovir treatment suggests a possible viral etiology.
REFERENCES
1. Tugal-Tutkun I, Urgancioglu M. Bilateral acute depigmentation of the iris. Graefes Arch Clin Exp Ophthalmol [Internet]. 2006[cited 2010 Jun 23];244(6):742-6. Available from: http://download.springer.com/static/pdf/167/art%253A10.1007%252Fs00417-005-0137-x.pdf?auth66=1365100095_059b651a5046293dc04e84295d29658b&ext=.pdf
2. Bringas Calvo R, Iglesias Cortiñas D. [Acute and bilateral uveitis secondary to moxifloxacin]. Arch Soc Esp Oftalmol [Internet]. 2004 [cited 2011 Mar 19];79(7):357-9. Spanish. Available from: http://www.oftalmo.com/seo/archivos/articulo.php?idSolicitud=1358&numR=7&mesR=7&anioR=2004&idR=84
3. Wefers Bettink-Remeijer M, Brouwers K, van Langenhove L, De Waard PW, Missotten TO, Martinez Ciriano JP, et al. Uveitis-like syndrome and iris transillumination after the use of oral moxifloxacin. Eye (Lond) [Internet]. 2009 [cited 2011 Jul 21];23(12):2260-2. Comment in: Eye (Lond). 2010;24(8):1419; author reply 1419-20. Available from: http://www.nature.com/eye/journal/v23/n12/full/eye2009234a.html
4. Willermain F, Deflorenne C, Bouffioux C, Janssens X, Koch P, Caspers L. Uveitis-like syndrome and iris transillumination after the use of oral moxifloxacin. Eye (Lond) [Internet]. 2010 [cited 2011 Mar 19];24(8):1419; author reply -20. Comment on: Eye (Lond). 2009;23(12):2260-2. Available from: http://www.nature.com/eye/journal/v24/n8/full/eye201019a.html
5. Tugal-Tutkun I, Araz B, Taskapili M, Akova YA, Yalniz-Akkaya Z, Berker N, et al. Bilateral acute depigmentation of the iris: report of 26 new cases and four-year follow-up of two patients. Ophthalmology [Internet]. 2009 [cited 2012 Oct 12];116(8): 1552-7, 7 e1. Available from: http://www.sciencedirect.com/science/article/pii/S0161642009001791#
6. Tugal-Tutkun I, Onal S, Garip A, Taskapili M, Kazokoglu H, Kadayifcilar S, et al. Bilateral acute iris transillumination. Arch Ophthalmol [Internet]. 2011[cited 2012 Jan 4];129(10):1312-9. Available from: http://archopht.jamanetwork.com/article.aspx?articleid=1106464
7. Goktas A, Goktas S. Bilateral acute depigmentation of the iris first misdiagnosed as acute iridocyclitis. Int Ophthalmol [Internet]. 2011[cited 2012 Nov 21];31(4):337-9. Available from: http://download.springer.com/static/pdf/837/art%253A10.1007% 252Fs10792-011-9452-x.pdf?auth66=1365100875_cc2c3b75db0d3efc4911fa04f5cf1332&ext=.pdf
8. Portmann A, Gueudry J, Siahmed K, Muraine M. [Bilateral acute depigmentation of the iris syndrome]. J Fr Ophtalmol. 2011;34(5):309-12. French.
9. Dastrup BT, Cantor L, Moorthy RS, Vasconcelos-Santos D, Rao N. An unusual manifestation of herpes simplex virus-associated acute iris depigmentation and pigmentary glaucoma. Arch Ophthalmol [Internet]. 2011[cited 2012 Dec 21];129(2):253-4. Available from: http://archopht.jamanetwork.com/article.aspx?articleid=426961
 Corresponding author:
Corresponding author:
Heloisa Andrade Maestrini
Rua Maranhão, 65
Belo Horizonte (MG) - 30150-330 - Brazil
E-mail: [email protected]
Submitted for publication: December 7, 2012
Accepted for publication: January 31, 2013
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: H.A.Maestrini, None; A.A.Maestrini, None; D.O.Machado, None; D.V.V.Santos, None; H.G.de Almeida, None.
Study carried out at Clínica Oculare, Belo Horizonte (MG).

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.