Arq. Bras. Oftalmol. 2009; 72 (6): 10.1590/S0004-27492009000600014
Total: 2196
Priscila Hae Hyun Rim1; Eugênio Santana de Figueirêdo1; Fabio Endo Hirata1; Carlos Eduardo Steiner2; Antonia Paula Marques-de-Faria2
DOI: 10.1590/S0004-27492009000600014
ABSTRACT
A case of identical male twins with Cohen syndrome who present multiple ophthalmic findings is reported. The patients were identical 16 year-old twin boys who showed down slanting eyelids, mild ptosis, high-grade myopia, small cortical lens opacities, posterior subcapsular cataracts, myotic and corectopic pupils with poor dilation due to focal iris atrophy and retinochoroidal dystrophy. Ophthalmologists must be aware of the ocular and systemic findings of Cohen syndrome in the evaluation of young patients with mental retardation and visual impairment.
Keywords: Syndrome; Twins, monozygotic; Myopia; Retina; Mental Retardation; Abnormalities, multiple; Eye diseases; Vision, low; Male; Adolescent; Case reports
RESUMO
Relata-se caso de gêmeos idênticos com síndrome de Cohen que apresentam múltiplos achados oftalmológicos. Os pacientes eram gêmeos idênticos, do sexo masculino, que apresentavam pálpebras em forma de onda, ptose moderada, alta miopia, opacidades cristalinianas corticais discretas, catarata subcapsular posterior, pupilas mióticas e corectópicas com pobre dilatação devido à atrofia focal de íris, além de distrofia retinocoroidiana. Os oftalmologistas devem estar atentos quanto aos achados oftalmológicos e sistêmicos da síndrome de Cohen na avaliação de pacientes jovens com retardo mental e baixa visão.
Descritores: Síndrome; Gêmeos monozigóticos; Miopia; Retina; Retardo mental; Anormalidades múltiplas; Oftalmopatias; Baixa visão; Masculino; Adolescente; Relatos de casos
RELATOS DE CASOS
Ocular findings in Brazilian identical twins with Cohen syndrome: case report
Achados oftalmológicos em gêmeos idênticos brasileiros com síndrome de Cohen: relato de caso
Priscila Hae Hyun RimI; Eugênio Santana de FigueirêdoII; Fabio Endo HirataII; Carlos Eduardo SteinerIII; Antonia Paula Marques-de-FariaIII
IMD Departament of Ophthalmo/Otorhinolaringology, Universidade Estadual de Campinas - UNICAMP - Campinas (SP) - Brazil
IIMD Departament of Ophthalmo/Otorhinolaringology, UNICAMP - Campinas (SP) - Brazil
IIIPhD Departament of Medical Genetics, UNICAMP - Campinas (SP) - Brazil
ABSTRACT
A case of identical male twins with Cohen syndrome who present multiple ophthalmic findings is reported. The patients were identical 16 year-old twin boys who showed down slanting eyelids, mild ptosis, high-grade myopia, small cortical lens opacities, posterior subcapsular cataracts, myotic and corectopic pupils with poor dilation due to focal iris atrophy and retinochoroidal dystrophy. Ophthalmologists must be aware of the ocular and systemic findings of Cohen syndrome in the evaluation of young patients with mental retardation and visual impairment.
Keywords: Syndrome; Twins, monozygotic; Myopia; Retina/abnormalities; Mental Retardation; Abnormalities, multiple; Eye diseases/pathology; Vision, low; Male; Adolescent; Case reports
RESUMO
Relata-se caso de gêmeos idênticos com síndrome de Cohen que apresentam múltiplos achados oftalmológicos. Os pacientes eram gêmeos idênticos, do sexo masculino, que apresentavam pálpebras em forma de onda, ptose moderada, alta miopia, opacidades cristalinianas corticais discretas, catarata subcapsular posterior, pupilas mióticas e corectópicas com pobre dilatação devido à atrofia focal de íris, além de distrofia retinocoroidiana. Os oftalmologistas devem estar atentos quanto aos achados oftalmológicos e sistêmicos da síndrome de Cohen na avaliação de pacientes jovens com retardo mental e baixa visão.
Descritores: Síndrome; Gêmeos monozigóticos; Miopia; Retina/anormalidades; Retardo mental; Anormalidades múltiplas; Oftalmopatias/patologia; Baixa visão; Masculino; Adolescente; Relatos de casos
INTRODUCTION
First described in 1973 by Cohen et al.(1), Cohen syndrome (MIM n. 216550)(2) is a rare autosomal recessive disorder caused by mutations in gene COH1 on chromosome 8q22(3). A metabolic disorder affecting connective tissue has been suggested as the pathogenesis of Cohen syndrome(4). Although no clinical diagnostic criteria are widely accepted(5), the diagnosis is based on the combination of clinical findings including mental retardation, joint hyperextensibility, truncal obesity, cheerful disposition, as well as craniofacial, hematological and ophthalmologic abnormalities(2,6-7).
Most of the reported patients with Cohen syndrome have ocular anomalies. Typical ophthalmologic features include myopia, cataract and tapetoretinal degeneration(8). Other ocular findings are wave-shaped and down slanting eyelids, ptosis, thick eyebrows and eyelashes, astigmatism, strabismus, microcornea, microphthalmia, sluggish papillary reaction, lens subluxation, coloboma and bull's eye maculopathy. Patients usually present poor vision acuity, nyctalopia and constricted visual fields(1,9-10). Visual problems commonly begin in the preschool years(10).
In the present report, the first cases in Brazil of identical male twins with Cohen syndrome who present multiple ophthalmic findings are described.
CLINICAL REPORT
Patients were identical 16 year-old twin boys who were referred for diagnostic evaluation due to myopia, nystagmus, obesity and delayed neurological development. The twins were born after an uncomplicated pregnancy of a non-consanguineous couple. In the family history, a paternal aunt is cited as having high myopia; a maternal aunt and the maternal grandmother present with deaf-mutism. Twin 1 was born at term, weight 2,680 g, length 48 cm, Apgar scores 9/10. Twin 2 was born with a weight of 2,650g, length 44 cm and the same Apgar scores. Both presented delayed neurological development. At the age of three months they were noted to present nystagmus and high myopia. Twin 1 also had a unique seizure during a febrile episode.
At physical examination, both present overweight and normal stature and head circumference. Besides obesity, the following dysmorphic features were noted: synophrys, flat occipitum, epicantal folds, high nasal bridge, high and narrow palate, prominent upper central incisors, long arms, mild fifth finger clinodactyly, narrow fingers, flat feet, genu valgum, and lumbar lordosis. They also show mild facial asymmetry and the twin 2 has scoliosis.
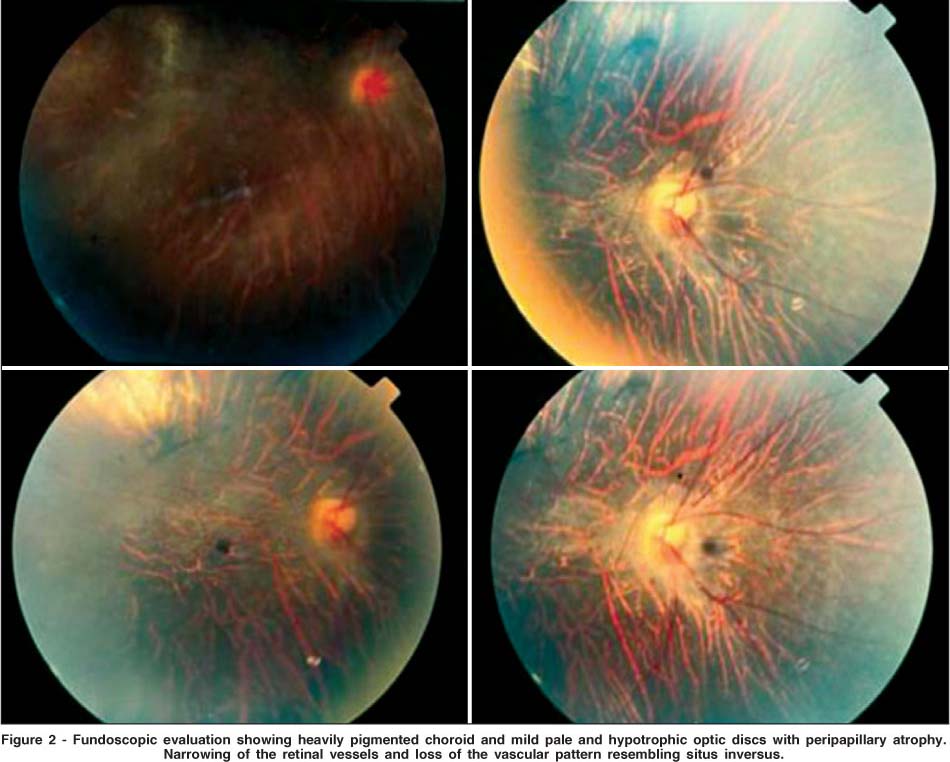
Ophthalmologic examination showed down slanting eyelids and mild ptosis (Figure 1), high-grade myopia [Twin 1: OD -10.0 diopters (D) with visual acuity of (VA) 20/200 and OS -10.5 D with VA of 20/200; Twin 2: OD -9.0 D with VA of 20/100 and OS -9.5 D with VA of 20/150]. At biomicroscopy, the following changes were observed: small cortical lens opacities, posterior subcapsular cataracts, myotic and corectopic pupils with poor dilation due to focal iris atrophy. Fundus changes presented with widespread retinochoroidal dystrophy (Figure 2). Choroid was heavily pigmented, but choroidal vessels appeared prominent because of the thin retinal pigment epithelium. Fine pigment granularity and pigment clumps were seen at the retinal periphery. Optic discs were pale and hypotrophic with peripapillary atrophy. Retinal vessels were narrow and showed loss of vascular pattern resembling situs inversus.

A venous blood sample was collected in order to determine the presence of neutropenia. However, both patients presented normal neutrophil count.
Chromosomal analysis of the patients (lymphocytes from peripheral blood, G-banding) revealed a normal 46, XY constitution. Molecular genetic analysis was not available.
DISCUSSION
Cohen et al. described a new syndrome in three patients in 1973. These young patients share in common obesity, hypotonia and mental deficiency associated with craniofacial, oral, ocular and limb anomalies. Among the ocular features, mottled retina, strabismus, myopia, microphthalmia and coloboma were mentioned(1). The cases reported in this article showed significant changes in various ocular structures including eyelid abnormalities, high myopia, iris atrophy, cataract and a generalized retinal dystrophy, resulting in an important visual impairment.
In order to encompass the phenotypic variability presented in distinct populations, some authors proposed the presence of at least two of the following major diagnostic criteria: 1) facial gestalt, characterized by thick hair, eyebrows and eyelashes, wave shaped, downward slanting palpebral fissures, prominent, beaked shaped nose, short, upturned philtrum with grimacing expression on smiling; 2) pigmentary retinopathy; 3) neutropenia (defined as <2 x 10-9/mm3). Besides, there are some minor diagnostic criteria: 1) early onset, progressive myopia, 2) microcephaly, 3) truncal obesity with slender extremities, 4) joint hyperextensibility(6).
Both brothers presented wave-shaped down slanting eyelids and mild ptosis, found in 71% and 13% of the reported patients, respectively(5).
Myopia was found in 44% of patients with Cohen syndrome in the literature. It is usually progressive and of high grade(5). The twins reported here presented myopia ranging from -9.0 to -10.5 D.
A retrospective and prospective study of 22 patients, aged from 2 to 57 years, showed lens opacities in 13 patients, including one case as early as 15 years-old. Both twins presented small lens opacities and posterior subcapsular cataract, a rare characteristic found at this age and usually observed in older patients aged over 40 years-old(9).
Chorioretinal dystrophy was added in 1984 as an important manifestation of the syndrome(4). Approximately 38% of the patients in published cases present this feature(5). This characteristic was recognized in both brothers.
There is a large phenotypic variability in Cohen syndrome patients(5-6,10). This variability is illustrated by the scoliosis and the more intense facial asymmetry in twin 2. Phenotype is associated with mutations in the COH1 gene assigned to the long arm of chromosome 8(3). The identification of more than 70 COH1 mutations in different populations demonstrates an allelic heterogeneity that could explain the variability of clinical presentation(5).
In 1984, other authors had considered neutropenia as an essencial feature for the diagnosis of Cohen syndrome in Finnish patients(4). Some authors, however, did not indentify neutropenia in all individuals of a group of English patients and considered it an important, but not obligatory characteristic for the diagnosis(6). The patients reported here did not presented low neutrophil count.
CONCLUSION
Ophthalmologists must be aware of the ocular and systemic findings of Cohen syndrome in the evaluation of young patients with mental retardation and visual impairment. Although the syndrome occurs with low frequency worldwide, it would help to avoid underdiagnosis or misdiagnosis, as well as offer the possibility of genetic counseling to the parents. No clinical diagnostic criteria are accepted at this time, but diagnosis based on the main clinical features of the syndrome has crucial importance since the molecular analysis is not always available.
REFERENCES
1. Cohen MM Jr, Hall BD, Smith DW, Graham CB, Lampert KJ. A new syndrome with hypotonia, obesity, mental deficiency and facial, oral, ocular and limb anomalies. J Pediatr. 1973;83(2):280-4.
2. Mckusick VA. Mendelian Inheritance in man: a catalog of human genes and genetic disorders. 12th ed. Baltimore: The John Hopkins University Press; 1998. p.2099.
3. Tahvanainen E, Norio R, Karitta E, Ranta S, Weissenbach J, Sistonen P, et al. Cohen syndrome gene assigned to the long arm chromosome 8 by linkage analysis. Nat Genet. 1994;7(2):201-4.
4. Norio R, Raitta C, Lindahi E. Further delineation of Cohen syndrome: report on chorioretinal dystrophy, leucopenia and consanguinity. Clin Genet. 1984; 25(1):1-14.
5. Taban M, Memoracion-Peralta DS, Wang H, Al-Gazali LI, Traboulsi EI. Cohen syndrome: Report of nine cases and rewiew of the literature, with emphasis on ophthalmic features. J AAPOS. 2007;11(5):431—7.
6. Chandler KE, Kidd A, Al-Gazali L, Kolehmainen J, Lehesjoki AE, Black GCM et al. Diagnostic criteria, clinical characteristics, and natural history of Cohen syndrome. J Med Genet. 2003;40(4):233-241.
7. Kivitie-Kallio A, Norio R. Cohen syndrome: essential features, natural history, and heterogeneity. Am J Med Genet. 2001;102(2):125-35.
8. Steinlein O, Tariverdian G, Boll HU, Vogel F. Tapetoretinal degeneration in brothers with apparent Cohen syndrome: Nosology with Mirhosseini-Holmes-Walton Syndrome. Am J Med Genet. 1991;41(2):196-200.
9. Kivitie-Kallio A, Summanen P, Raitta C, Norio R. Ophthalmologic findings in Cohen syndrome. A long term follow up. Ophthalmology. 2000;107(9):1737-45.
10. Chandler KE, Biswas S, Lloyd IC, Parry N, Clayton-Smith J, Black GC. The ophthalmic findings in Cohen syndrome. Br J Ophthalmol. 2002;86(12):1395-8.
 Correspondence address:
Correspondence address:
Priscila Hae Hyun Rim
Departament of Ophthalmo/Otorhinolaringology
Campinas State University
Caixa Postal 5.111
Rua Tessália Vieira de Camargo #126
Campinas (SP) - Brazil
CEP 13083-970
E-mail: [email protected]
Recebido para publicação em 13.11.2007
Última versão recebida em 05.06.2009
Aprovação em 03.09.2009
Trabalho realizado no Departamento de Oftalmologia e Otorrinolaringologia da Universidade Estadual de Campinas (UNICAMP) - Campinas (SP) - Brazil.

How to cite this article:
 ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
ABO is licensed under a Creative Commons Attribution-NonComercial 4.0 Internacional.
{kind=link}