

Kuddusi Teberik1; Mehmet Tahir Eski2; Emel Çalışkan3; Özge Kılınçel4; Murat Kaya1; Handan Ankaralı5
DOI: 10.5935/0004-2749.20190008
ABSTRACT
Purpose: To compare effects of 5% topical povidone iodine with prophylactic topical azithromycin and moxifloxacin on bacterial flora in patients undergoing intravitreal injection.
Methods: A total of 132 patients were randomly assigned to receive treatment with azithromycin or moxifloxacin, or no treatment (control group). In total, 528 specimens were obtained at the time of admission, 4 days before intravitreal injection, 4 days after intravitreal injection, and 8 days after intravitreal injection. Samples were immediately sent to the microbiology laboratory for incubation.
Results: The microorganism observed most frequently was coagulasenegative Staphylococcus (23.8%). When the results of samples obtained on Day 4 before injection were assessed, growth of coagulase-negative Staphylococcus was significantly lower in the moxifloxacin group, compared with controls (p=0.049). Acinetobacter baumannii continued to grow after administration of azithromycin (p=0.033). When the results of four days after intravitreal injection were evaluated, growth of coagulase-negative Staphylococcus was higher in controls, compared with patients who received azithromycin or moxifloxacin (p=0.004). Eradication rate was significantly higher in the moxifloxacin group than in the control group (p=0.001). Samples obtained on Day 8 after intravitreal injection showed similar levels of bacterial growth in all groups (p=0.217).
Conclusion: Moxifloxacin was more effective than 5% povidone iodine in controlling the growth of conjunctival bacterial flora. Use of moxifloxacin in combination with 5% povidone iodine resulted in a synergistic effect.
Keywords: Azithromycin; Conjunctiva/microbiology; Intravitreal injection; Moxifloxacin; Povidone-iodine
RESUMO
Objetivo: Comparar os efeitos de iodopovidona tópico a 5% com azitromicina e moxifloxacina profiláticas sobre a flora bacteriana em pacientes submetidos à injeção intravítrea.
Métodos: Um total de 132 pacientes foram aleatoriamente designados para receber tratamento com azitromicina ou moxifloxacina ou nenhum tratamento (grupo controle). No total, 528 amostras foram obtidas no momento na admissão, 4 dias antes da injeção intravítrea, 4 dias após a injeção intravítrea e 8 dias após a injeção intravítrea. As amostras foram imediatamente enviadas para o laboratório de microbiologia para incubação.
Resultados: O microorganismo mais frequentemente observado foi o Staphylococcus coagulase-negativo (23,8%). Quando os resultados das amostras obtidas no dia 4 antes da injeção foram avaliados, o crescimento do Staphylococcus coagulase-negativo foi significativamente menor no grupo moxifloxacina, em comparação com os controles (p=0,049). Acinetobacter baumannii continuou a crescer após a administração de azitromicina (p=0,033). Quando os resultados de 4 dias após a injeção intravítrea foram avaliados, o crescimento do Staphylococcus coagulase-negativo foi maior no controle, em comparação com pacientes que receberam azitromicina ou moxifloxacina (p=0,004). A taxa de erradicação também foi significativamente maior no grupo moxifloxacina do que no grupo controle (p=0,001). As amostras obtidas no dia 8 após injeção intravítrea mostraram níveis semelhantes de crescimento bacteriano em todos os grupos (p=0,217).
Conclusão: A moxifloxacina foi mais eficaz do que 5% de iodopovidona no controle do crescimento da flora bacteriana conjuntival. O uso de moxifloxacina em combinação com 5% de iodopovidona resultou em um efeito sinérgico.
Descritores: Azitromicina; Conjuntiva/microbiologia; Injeção intravítrea; Moxifloxacina; Iodopovidona
INTRODUCTION
In recent years, intravitreal injection is performed with increasing frequency in the practice of ophthalmology(1). Intravitreal injections are frequently used in the treatment of retinal disorders, such as diabetic retinopathy, senile macular degeneration, retinal vein occlusion, and degenerative myopia(2). Topical antibiotics and 5% povidone iodine (PI) are widely used for reducing the ocular surface bacterial load during intravitreal injections(3). Despite the evidence demonstrating that use of topical antibiotics decreases conjunctival bacterial load, several studies have demonstrated that the addition of preinjection or postinjection topical antibiotics to PI antisepsis has no effect on the rate of endophthalmitis, compared with use of PI alone(4,5). A recent prospective study that analyzed bacterial growth using conjunctival swabs reached a similar conclusion; preoperative application of 0.5% moxifloxacin did not decrease bacterial growth beyond the level achieved with PI alone(6). However, recent studies have shown that the topical use of antibiotics after repeated injections not only decreases risk for endophthalmitis but also increases resistance of conjunctival flora to antibiotics(7). There is a consensus that instillation of PI prevents postoperative endophthalmitis(8,9). However, variations in practice patterns exist, and standardized recommendations on the use of PI in preventing postprocedure endophthalmitis are currently lacking. The present study compared 5% topical PI with prophylactic topical antibiotics (azithromycin and moxifloxacin) in terms of effects on bacterial flora in patients undergoing intravitreal injection.
METHODS
This study included patients admitted to the outpatient clinic at the Department of Ophthalmology at Düzce University Medical School during the period from June 2015 to January 2016. Only patients diagnosed with neovascular age-related macular degeneration were included in the study. A total of 132 patients were included in the study, 41 in the first group, 41 in the second group, and 50 in the third group. Assignment of patients to groups was done by simple random sampling taking age and gender matching into consideration. The number of patients in the groups was determined to be balanced. The patients and the researchers are masked to the treatment.
Exclusion criteria included age <18 yr, previous history of ocular injection, use of contact lenses, active eye infection, history of ocular surgery, use of topical ophthalmic drugs or systemic antibiotics within the last 3 months, and allergy to PI or other agents used in the study.
Conjunctival samples were obtained from lower eyelid fornix by swabs. In obtaining samples, the procedure was meticulously performed around eyelids and eyelashes to avoid contamination.
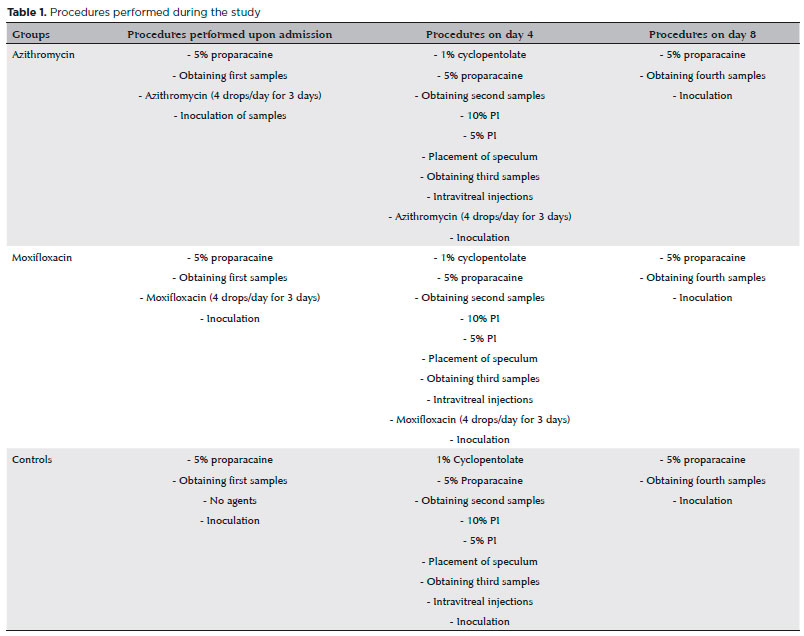
All samples were obtained from the patients in the azithromycin, moxifloxacin, and control groups on admission and Days 4 (injection before and after) and 8. On admission, the first samples were obtained from all patients, and the first and second groups were prescribed with azithromycin (Azyter, Thea Pharma, France) and moxifloxacin (Vigamox, Alcon, Greece) at the dose of four drops per day, whereas the controls were given no drugs. All patients were invited to give injections and obtain the second and third samples on Day 4 after a 3 day interval. The second conjunctival samples were obtained from all patients before injections. Eyelids and surrounding area were stained with 10% PI. After 5% PI was applied into the eyes to be injected. First, a 3 min interval was given, and sterile drapes were placed into the eyes. In order to obtain samples, an eyelid speculum was positioned, avoiding contact with the eyelids and eyelashes. Intravitreal injections were performed with 30-32G needles at a distance of 3.5 mm in pseudophakic eyes and of 4.00 mm in phakic eyes from the limbus. After the injections, the first and second groups were represcribed with azithromycin and moxifloxacin at a dose of four drops per day, whereas no treatment regime was also prescribed for the controls. All patients were invited to obtain the fourth samples on Day 8. On Day 8, the fourth samples were obtained from all patients (Table 1).
After obtaining thorough swabs from conjunctival sacs, the samples were immediately sent to the microbiology laboratory and inoculated on 5% blood agar, eosin methylene blue agar, and chocolate agar plates and incubated at 37°C for 24 h. After incubation, Gram staining was performed. Gram-positive cultures were identified by catalase and coagulase testing using an automated BD Phoenix system (Becton Dickinson Diagnostic Systems Sparks, MD, USA). Gram-negative cultures were identified using the same automated BD Phoenix system (Becton Dickinson Diagnostic Systems Sparks, MD, USA).
The ethical board at the Medical School of Düzce University approved the study (Clinical trial protocol number: 2015/43). The study was performed in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Informed consent was also obtained from all study participants.
Statistical analysis
Descriptive values of data were computed as count and percent frequencies. The relationship between the results of staining and use of antibiotics was investigated using the Fisher-Freeman-Halton test, followed by post hoc z-test with Bonferroni adjustment for contingency tables. Statistically, significant level was accepted as p<0.05, and Predictive Analytics SoftWare (PASW, version 18) was used for all calculations.
RESULTS
Of 132 patients, 68 (51.5%) were women and 64 (48.5%) were men. Culture results of the first samples obtained from all groups on admission are presented in table 2. Upon investigating the results of the first samples, it was seen that coagulase-negative Staphylococcus (CNS) was the most frequent bacteria (23.8% in 31 cases). The second most common growth of bacteria was in Acinetobacter spp. (4.5% in six cases). In addition, Staphylococcus aureus was seen in three cases (2.27%), Serratia marcescens in one case (0.7%), Morganella morganii in one case (0.7%), and Escherichia coli in one case (0.7%). Relative proportions of each bacterial species were similar across groups (p>0.05).
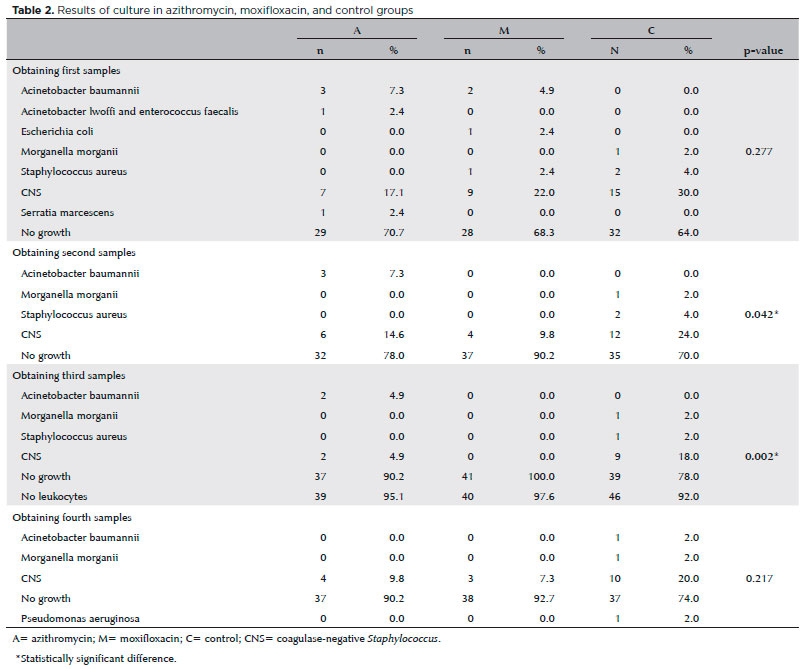
When the results of samples obtained before injection on Day 4 were assessed, CNS growth frequency was seen to be significantly lower in the moxifloxacin group, compared with the controls receiving no antibiotic treatment (p=0.049). In addition, the eradication rate was found to be significantly higher in the moxifloxacin group than in the control group (p=0.011). No growth was observed for Staphylococcus aureus, E. coli, or A. baumannii after treatment with moxifloxacin. A. baumannii continued to grow after administration of azithromycin (p=0.033). The culture results of second samples in azithromycin, moxifloxacin, and control groups are presented in table 2.
When the results of third samples were evaluated, CNS was determined to grow higher only in the controls, compared with the azithromycin and moxifloxacin groups (p=0.004). When compared with first samples, it was found out that 5% PI application and CNS frequency before the injections decreased significantly in the azithromycin and moxifloxacin groups; however, 5% PI application alone decreased CNS frequency although it was statistically insignificant. Eradication rate was significantly higher in the moxifloxacin group than in the control group (p=0.001). The findings of third samples were presented in table 2. In addition, when the second and third sample results were compared in the control group, it was seen that there was no significant difference (p>0.05). It was found that there was no difference between three groups in terms of the results of fourth samples obtained on Day 8 (p=0.217). The findings of fourth samples were presented in table 2. None of the patients included in the study developed endophthalmitis.
DISCUSSION
In our study, CNS was determined as the most commonly isolated organisms in the samples obtained on admission prior to the administration of 5% PI and antibiotics. In a study performed by Ataş et al.(10), CNS was the microorganism isolated most commonly from conjunctival samples obtained before intravitreal injection(10). In another study performed by Jason et al., CNS was detected to be the most frequently bacterial isolate as 77% obtained from conjunctiva(7). Among the most common bacteria seen in conjunctiva are Staphylococcus spp., Corynebacterium spp., and Propionibacterium spp. Normal conjunctival flora is excepted to play a protecting role against these bacteria by preventing the development of such pathogenic bacteria. S. epidermis prevents colonization by S. aureus; the latter is a more pathogenic microorganism(11,12).
Despite its protective role, Staphylococcus epidermis is the most commonly isolated organism in the clinical spectra of conjunctivitis, keratitis, and endophthalmitis(10). In this study by Dave et al., exposures to recurrent fluoroquinolones and azithromycin were reported to lead to changes in conjunctival flora and to increase the development of S. epidermidis. The same study showed that S. epidermidis constitutes 45.7% of conjunctival flora prior to injection; this value increased to 63.4% after injection(12). In another study by Milder et al., however, no significant difference was reported to be present between eyes to be intravitreally injected and those of the controls in terms of the types of bacteria isolated from the samples and the sample positivity(13). At Day 4 after injection, CNS proliferation was significantly lower in the moxifloxacin group than in the control group. Non-growth frequency was observed to be significantly higher in the moxifloxacin group, compared with the other two.
In our study, S. aureus, E. coli, and A. baumannii were seen not to grow again with the administration of moxifloxacin. We consider that such an effect might be due to the well-penetration of fourth-generation quinolones that could be inhibited both topoisomerase and DNA gyrase into ocular tissues and their broad spectrum antibacterial effects. New-generation fluoroquinolones were more effective than older-generation agents (e.g., levofloxacin, trovafloxacin, and clinafloxacin), against Gram-positive organisms, including Streptococcus pneumoniae(14).
On the other hand, we also determined that A. baumannii growth continues after the administration of the azithromycin. Azithromycin was chosen for use in our study because it is more effective than erythromycin against Gram-negative organisms and exhibits broad-spectrum activity against common bacteria. Due to the recommendation of its 3 day use, we took the use of azithromycin into account like 3 days in our study. However, azithromycin has a weak penetration capacity into ocular tissues when applied topically(5), and it is known that azithromycin has a weak effect on Acinetobacter strains(15).
When the results of third samples were investigated, CNS produced at a higher rate only in the group exposed to 5% PI, compared with the azithromycin and moxifloxacin groups. When samples obtained on Day 8 were compared with those obtained 4 days prior to injection, a nonsignificant decrease in CNS growth was observed in patients who received 5% PI prior to injection and treatment with azithromycin or moxifloxacin, compared with patients who received 5% PI only. As an antiseptic agent, 5% PI has a large impact area on both Gram-negative and Gram-positive bacteria, fungi, and viruses(16). In addition, some prospective studies showed that the topical administration of 5% PI in eyes exposed to intravitreal injection decreased significantly the rate of apositive culture for bacteria(17). Moss et al. also found a significant decrease in conjunctival flora after the topical application of 5% PI and suggested that 5% PI played a key role by increasing the permeability of antimicrobial agents through bacterial walls(5).
Although intravitreal injections are commonly administered, the optimal approach to preinjection and postinjection prophylaxis remains controversial. Most physicians routinely use 5% PI for antisepsis because of its well-known bactericidal effect(8,19). Preinjection and postinjection use of antibiotics seems to decrease increasingly. In a survey performed by the American Society of Retina Specialists (ASRS) in 2008, it was seen that the rate of retina specialists using topical antibiotics before intravitreal injection was 40%, whereas the rate of those applying after the injections was 86%. In another survey by ASRS in 2009, more than 80% of retina specialists recommended that antibiotics be used either before or after intravitreal injection. In the 2011 survey by ASRS, although 27% of specialists proposed the use of antibiotics before the injections, 62% advocated its use after the injections(20). In some studies where the results of combined topical antibiotics and 5% PI and those of 5% PI alone were compared, although the drops of topical antibiotics were confirmed to decrease conjunctival bacterial load, the incidence of endophthalmitis was demonstrated not to decrease(4,5). Similar findings were reported by a recent prospective study that investigated bacterial development in samples obtained with conjunctival swabs. However, it was suggested that preoperative administration of 0.5% moxifloxacin caused no better results in a bacterial culture than that of 5% PI(6). Another study indicated that conjunctival exposure to 5% PI for 30 s led to an important decrease in bacterial colonization, and the 30 s period was proposed as a sufficient contacting period before intravitreal injection(21). The only confirmed method for prophylaxis of endophthalmitis is sterilization of the ocular surface with 5% PI. In a large series conducted by Cheung et al., endophthalmitis developed less frequently among patients who did not receive antibiotics after intravitreal injection, compared with those who did receive antibiotics after intravitreal injection(22). Lyall et al. recommended that, in order to decrease risk for anti-VEGF endophthalmitis, topical antibiotics should be administered just before and after intravitreal injection, subconjunctival anesthesia should be avoided, and blepharitis should be treated prior to injection(23).
Several studies in the current literature attribute the lack of a standardized treatment for endophthalmitis prophylaxis to the development of antimicrobial resistance with the use of topical antibiotics after intravitreal injection. In such cases, the use of topical antibiotics was insufficient to decrease risk for endophthalmitis(24,25). Previous studies have demonstrated that microbial organisms acquiring resistance to an antiseptic agent also gain crossresistance to other antiseptic agents, such as chlorhexidine gluconate and alkyldiaminoethylglycine hydrochloride. However, microbial organism that has developed resistance to antiseptic agents remain vulnerable to treatment with 5% PI(26). Recent studies investigating the advantages of antibiotic prophylaxis have reported conflicting results(8,18,27). For each case seen at our clinic, after 3 min of conjunctival antisepsis, followed by intravitreal injection, patients are prescribed topical 0.5% moxifloxacin: four drops per day for 3-7 days.
One of the limitations of this study is its small sample size. Additional studies that include more patients will be necessary to ultimately improve patient outcomes. Because moxifloxacin has only been used in Turkey since 2011, the drug may continue to inhibit the growth of Gram-positive bacteria, with decreased ambient levels of drug resistance.
We found that moxifloxacin is more effective than 5% PI in controlling the growth of conjunctival bacterial flora, even exhibiting a synergistic effect when used in combination with 5% PI. This finding should be taken into account when azithromycin and moxifloxacin are used as first-line modalities for endophthalmitis prophylaxis, because azithromycin and moxifloxacin may not eradicate all types of bacteria commonly observed during the preinjection and postinjection periods. For this reason, combined use of antibiotics with 5% PI is recommended as the most appropriate regime for prophylaxis.
REFERENCES
1. Campbell RJ, Bronskill SE, Bell CM, Paterson JM, Whitehead M, Gill SS. Rapid expansion of intravitreal drug injection procedure, 2000 to 2008: a population-based analysis. Arch Ophthalmol. 2010; 128(3):359-62.
2. Dossarps D, Bron AM, Koehrer P, Aho-Glélé LS, Creuzot-Garcher C, FRCR net (French Retina specialists net). Endophthalmitis After Intravitreal Injections: Incidence, Presentation, Management, and Visual Outcome. Am J Ophthalmol. 2015;160(1):17-25.
3. Shimada H, Hattori T, Mori R, Nakashizuka H, Fujita K, Yuzawa M. Minimizing the endophthalmitis rate following intravitreal injections using 0.25% povidone-iodine irrigation and surgical mask. Graefes Arch Clin Exp Ophthalmol. 2013;251(8):1885-90.
4. Bhatt SS, Stepien KE, Joshi K. Prophylactic antibiotic use after intravitreal injection:effect on endophthalmitis rate. Retina. 2011; 31(10):2032-6.
5. Moss JM, Sanisio SR, Ta CN. A prospective randomized evaluation of topical gatifloxacin on conjunctival flora in patients undergoing intravitreal injections. Ophthalmology. 2009;116:1498-501.
6. Halachmi-Eyal O, Lang Y, Keness Y, Miron D. Preoperative topical moxifloxacin 0.5% and povidon-iodine 5.0% alone to reduce bacterial colonization in the conjunctival sac. J Cataract Refract Surg. 2009;35(12):2109-14.
7. Hsu J, Gerstenblith AT, Garg SJ, Vander JF. Conjunctival flora antibiotic resistance patterns after serial intravitreal injections without postinjection topical antibiotics. Am J Ophthalmol. 2014; 157(3):514-8.
8. Speaker MG, Menikoff JA. Prophylaxis of endophthalmitis with topical povidone-iodine. Ophthalmology. 1991;98(12):1769-75.
9. Ta CN. Minimizing the risk of endophthalmitis following intravitreous injections. Retina. 2004;24(5):699-705.
10. Ataş M, Başkan B, Ozköse A, Mutlu Sarıgüzel F, Demircan S, Pangal E. Effects of Moxifloxacin exposure on the conjunctival flora and antibiotic resistance profile following repeated intravitreal injections. Int J Ophthalmol. 2014;7(5):855-9.
11. Pleyer U, Baatz H. Antibacterial protection of the ocular surface. Ophthalmologica. 1997;211:Suppl 1:2-8.
12. Dave SB, Toma HS, Kim SJ. Ophthalmic antibiotic use and multidrug-resistant staphylococcus epidermidis: a controlled, longitudinal study. Ophthalmology. 2011;118(10):2035-40.
13. Milder E, Vander J, Shah C, Garg S. Changes in antibiotic resistance patterns of conjunctival flora due to repeated use of topical antibiotics after intravitreal injection. Ophthalmology. 2012;119:1420-4.
14. Park SH, Lim JA, Choi JS, Kim KA, Joo CK. The resistance patterns of normal ocular bacterial flora to 4 fluoroquinolone antibiotics. Cornea. 2009;28(1):68-72.
15. Yıldız O. Acinetobacter species. Yoğun Bakım Derg. 2007;7:144-50. http://www.yogunbakimdergisi.org/journal_issue.aspx?issue_id=26.
16. Lachapelle JM, Castel O, Casado AF, Leroy B, Micali G, Tennstedt D, et al. Antiseptics in the era of bacterial resistance: a focus on povidone iodine. Clin Pract. 2013;10(5):579-92.
17. Kim SJ, Chomsky AS, Sternberg PJr. Reducing the risk of endophthalmitis after intravitreous injection. JAMA Ophthalmol. 2013; 131(5):674-5.
18. Romero-Aroca P, Sararols L, Arias L, Casaroli-Marano RP, Bassaganyas F. Topical azithromycin or ofloxacin for endophthalmitis prophylaxis after intravitreal injection. Clin Ophthalmol. 2012;6:1595-9.
19. Berkelman RL, Holland BW, Anderson RL. Increased bactericidal activity of dilute preparations of povidone-iodine solutions. J Clin Microbiol. 1982;15(4):635-9.
20. The American Society of Retina Specialists (ASRS) (2013) Preferences and trends (PAT) surveys. http://www.asrs.org/asrs-community/pat-survey.
21. Friedman DA, Mason JO 3rd, Emond T, Mcgwin GJr. Povidone-iodine contact time and lid speculum use during intravitreal injections. Retina. 2013;33(5):975-81.
22. Cheung CS, Wong AW, Lui A, Kertes PJ, Devenyi RG, Lam WC. Incidence of endophthalmitis and use of antibiotic prophylaxis after intravitreal injections. Ophthalmology. 2012;119(8):1609-14.
23. Lyall DA, Tey A, Foot B, Roxburgh ST, Virdi M, Robertson C, et al. Postintravitreal anti-VEGF endophthalmitis in the United Kingdom: incidence, features, riskfactors, and outcomes. Eye. 2012;26(12): 1517-26.
24. Chen RW, Rachitskaya A, Scott IU, Flynn HW Jr. Is the use of topical antibiotics for intravitreal injections the standard of care ora re we better off without antibiotics? JAMA Ophthalmol. 2013; 131(7):840-2.
25. Bhavsar AR, Stockdale CR, Ferris FL 3rd, Brucker AJ, Bressler NM, Glassman AR, Diabetic Retinopathy Clinical Research Network. Update on risk of endophthalmitis after intravitreal drug injections and potential impact of elimination of topical antibiotics. Arch Ophthalmol. 2012;130(6):809-10.
26. Kunisada T, Yamada K, Oda S, Hara O. Investigation on the efficacy of povidone-iodine against antiseptic-resistant species. Dermatology. 1997;195(2):14-8.
27. Bhavsar AR, Googe JM Jr, Stockdale CR, Bressler NM, Brucker AJ, Elman MJ, Glassman AR, Diabetic Retinopathy Clinical Research Network. Risk of endophthalmitis after intravitreal drug injection when topical antibiotics are not required:the diabetic retinopathy clinical research network laser-ranibizumab-triamcinolone clinical trials. Arch Ophthalmol. 2009;127(12):1581-3.
Submitted for publication:
February 18, 2018.
Accepted for publication:
June 3, 2018.
Approved by the following research ethics committee: Düzce University (#2015/43)
Funding: No specific financial support was available for this study
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose
© 2024 - All rights reserved - Conselho Brasileiro de Oftalmologia
![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
