

Allan Christian Pieroni Gonçalves1; Rodrigo Bernal da Costa Moritz1; Mário Luiz Ribeiro Monteiro1
DOI: 10.1590/S0004-27492011000500015
ABSTRACT
Primary localized amyloidosis is rare in the orbit. We report the case of a 63-year-old woman that presented with bilateral proptosis and ophthalmoplegia. A computed tomography scan revealed an infiltrative amorphous and markedly calcified mass in both orbits while a magnetic resonance scan showed a heterogeneous hypointense signal on T2-weighted images. A biopsy was performed through an anterior orbitotomy. Microscopy revealed extracellular amorphous and eosinophilic hyaline material which stained pink with Congo red and displayed green birefringence on polarized microscopy, leading to a diagnosis of amyloidosis. The results of the systemic workup were completely normal. A two-year follow-up period without any treatment disclosed no worsening of the condition. While calcification of nonvascular orbital lesions has often been regarded as suggestive of malignant disease, our case is a reminder that it can also be a characteristic presenting sign of orbital amyloidosis.
Keywords: Amyloidosis; Orbit diseases; Exophthalmos; Magnetic resonance imaging; Ophthalmoplegia; Humans; Female; Middle aged; Case report
RESUMO
Amiloidose primária e localizada na órbita é rara. Relatamos o caso de paciente do sexo feminino, 63 anos que se apresentou com proptose bilateral e oftalmoplegia. A tomografia computadorizada mostrou uma massa infiltrativa amorfa e calcificada em ambas as órbitas enquanto que a imagem por ressonância magnética mostrou imagem heterogênea hipointensa ponderada em T2. Uma biópsia foi realizada por orbitotomia anterior. A microscopia revelou um material extracelular amorfo, hialino e eosinofílico que corou com vermelho Congo e mostrou cor verde birrefringente à microscopia com luz polarizada, levando ao diagnóstico de amiloidose. O resultado da investigação sistêmica foi inteiramente negativo. Um período de seguimento de dois anos sem qualquer tratamento não evidenciou piora da condição. Enquanto que a presença de calcificação de lesão não vascular da órbita frequentemente é considerada sugestiva de doençamaligna, o nosso caso serve para lembrar que pode também ser um sinal característico de amiloidose orbitária.
Descritores: Amiloidose; Doenças orbitárias; Exoftalmo; Imagem por ressonância magnética; Oftalmoplegia; Humanos; Feminino; Meia-idade; Relato de caso
RELATO DE CASO CASE REPORT
Primary localized amyloidosis presenting as diffuse amorphous calcified mass in both orbits: case report
Amiloidose primária localizada se apresentando como massa tumoral amorfa e calcificada em ambas as órbitas: relato de caso
Allan Christian Pieroni GonçalvesI; Rodrigo Bernal da Costa MoritzI; Mário Luiz Ribeiro MonteiroII
IPhysician, Department of Ophthalmology, Universidade de São Paulo - USP - São Paulo (SP), Brazil
IIProfessor, Department of Ophthalmology, Universidade de São Paulo - USP - São Paulo (SP), Brazil
ABSTRACT
Primary localized amyloidosis is rare in the orbit. We report the case of a 63-year-old woman that presented with bilateral proptosis and ophthalmoplegia. A computed tomography scan revealed an infiltrative amorphous and markedly calcified mass in both orbits while a magnetic resonance scan showed a heterogeneous hypointense signal on T2-weighted images. A biopsy was performed through an anterior orbitotomy. Microscopy revealed extracellular amorphous and eosinophilic hyaline material which stained pink with Congo red and displayed green birefringence on polarized microscopy, leading to a diagnosis of amyloidosis. The results of the systemic workup were completely normal. A two-year follow-up period without any treatment disclosed no worsening of the condition. While calcification of nonvascular orbital lesions has often been regarded as suggestive of malignant disease, our case is a reminder that it can also be a characteristic presenting sign of orbital amyloidosis.
Keywords: Amyloidosis; Orbit diseases/diagnosis; Exophthalmos; Magnetic resonance imaging; Ophthalmoplegia; Humans; Female; Middle aged; Case report
RESUMO
Amiloidose primária e localizada na órbita é rara. Relatamos o caso de paciente do sexo feminino, 63 anos que se apresentou com proptose bilateral e oftalmoplegia. A tomografia computadorizada mostrou uma massa infiltrativa amorfa e calcificada em ambas as órbitas enquanto que a imagem por ressonância magnética mostrou imagem heterogênea hipointensa ponderada em T2. Uma biópsia foi realizada por orbitotomia anterior. A microscopia revelou um material extracelular amorfo, hialino e eosinofílico que corou com vermelho Congo e mostrou cor verde birrefringente à microscopia com luz polarizada, levando ao diagnóstico de amiloidose. O resultado da investigação sistêmica foi inteiramente negativo. Um período de seguimento de dois anos sem qualquer tratamento não evidenciou piora da condição. Enquanto que a presença de calcificação de lesão não vascular da órbita frequentemente é considerada sugestiva de doençamaligna, o nosso caso serve para lembrar que pode também ser um sinal característico de amiloidose orbitária.
Descritores: Amiloidose; Doenças orbitárias/diagnóstico; Exoftalmo; Imagem por ressonância magnética; Oftalmoplegia; Humanos; Feminino; Meia-idade; Relato de caso
INTRODUCTION
Primary localized amyloidosis is an uncommon condition of the orbit with only 40 cases previously reported, 33 of which unilateral(1-6). Most cases presented as isolated extraocular muscle enlargement or as a mass in the area of the lacrimal gland or elsewhere in the orbit, usually in the upper part of the anterior orbit(1,2,6). The purpose of the present report was to document a patient with a unique presentation of primary localized amyloidosis characterized by a diffuse and densely calcified mass in both orbits. We emphasize the importance of including amyloidosis in the differential diagnosis of calcified lesions in the orbit.
CASE REPORT
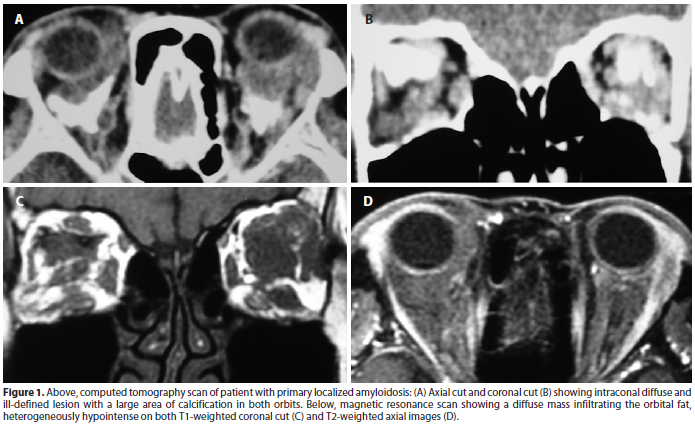
A 63-year-old woman with an otherwise unremarkable medical history reported painless progressive swelling of her left upper lid for 2 years and of both lower lids for 10 months. The external examination showed bilateral swelling of the lower eyelids and a palpable fibrous mass in both anterior orbits. Visual acuity and visual field measurements, pupillary reaction, intraocular pressure measurements and fundus examination were normal. Exophthalmometry measured 18 mm in each side. A marked limitation of eye movements was observed for all gaze positions . A slit-lamp evaluation revealed previous uncomplicated cataract surgery with intraocular lens implants in both eyes. Orbital computed tomography (CT) scans showed diffuse anterior and deep orbital amorphous fat infiltration with several foci of calcification (Figure 1). T1 and T2-weighted magnetic resonance images showed a heterogeneously hypointense diffuse mass infiltrating the orbital fat, with mild enhancement on T1-weighted fat-suppressed images following gadolinium injection (Figure 1). The results of a comprehensive workup for systemic and neoplastic disease were completely normal. A biopsy specimen was obtained via left anterior orbitotomy.
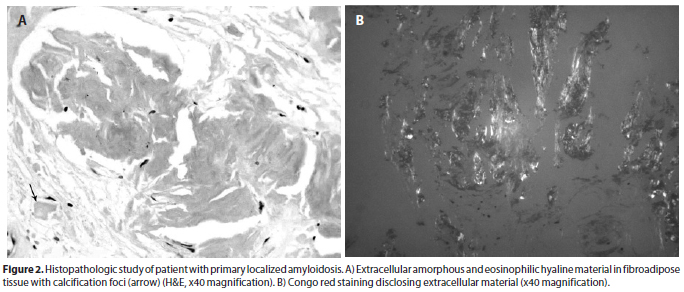
Microscopy revealed extracellular amorphous and eosinophilic hyaline material which stained pink with Congo red (Figure 2) and displayed green birefringence under polarizing microscopy. The histopathological diagnosis was amyloidosis. The clinical findings have remained unchanged over the past two years of follow-up without treatment.
DISCUSSION
The amyloidosis comprises a diverse and heterogeneous group of disorders characterized by the common finding of pathologic proteinaceous intercellular substance deposits, the amyloid, in various tissues and organs. It can be classified according to its distribution, the presence or absence of underlying chronic disease, and its immunocytochemical nature(7). Clinically, amyloidosis is categorized into two main forms, systemic and localized. Localized amyloidosis is an extremely rare condition generally occurring in the head and neck. Only 4% of such cases occur in the orbital region, mostly in the eyelid and conjunctiva(1,2). The clinical picture can be quite variable with possible involvement of the lacrimal gland, the extraocular muscles, the anterior orbit (localized mass) and the retrobulbar space (diffuse process). While orbital amyloidosis can cause mild proptosis, ocular motility restriction, secondary glaucoma and optic neuropathy, it usually has a benign course(1,4). CT findings include orbital mass infiltration which may be diffuse in the soft tissues, involve the lacrimal gland or be restricted to the extraocular muscles. In the few published reports of orbital amyloidosis which provide magnetic resonance imaging (MRI) findings, including the present case, amyloid deposition appears hypointense on T1 and T2-weighted images. This finding helps differentiate orbital amyloidosis from neoplasms, which generally have a more fluid structure that tends to brighten on T2-weighted images(2).
The imaging appearance of amyloidosis lesions is fairly non-descriptive but the presence of calcification on CT scan can be of great help in the differential diagnosis. Calcification of orbital lesions extrinsic to the lacrimal gland fossa are most likely associated with vascular lesions such as cavernous hemangioma, lymphangioma, varices and hemangiopericytoma(8). On the other hand, calcified lesions within the lacrimal gland fossa usually portend malignant disease. Metastatic tumors of the orbit, meningioma, teratoma, neurofibroma, sclerosing angioma and chondrosarcoma should also be included in the differential diagnosis of calcified orbital lesions(9). Although previous reports have documented calcification in amyloidosis, our case is interesting because of the magnitude of the calcified lesions in the orbit, exceeding that of any previously described case.
A complete workup for systemic disease is required to correctly classify the type of amyloid deposition. Systemic amyloid deposition is usually secondary to benign, low-grade, light chain-producing monoclonal gammopathy, resulting in widespread organ deposition and dysfunction. In contrast, reactive systemic amyloidosis affects patients with chronic inflammatory conditions in whom an acute response with production of serum amyloid-A protein causes hepatosplenomegaly and renal dysfunction. In our patient, the results of the systemic workup were normal and a two-year follow-up revealed no condition other than orbital deposition. The treatment of localized orbital amyloidosis is relief of symptoms, restoration of function and prevention of ocular morbidity. Surgical removal is often the treatment of choice in localized cases(2) In our case, surgical debulking would carry a significant risk of morbidity and the stability of the clinical course suggested a conservative approach.
In conclusion, we report a case of localized amyloidosis presenting with diffuse, densely calcified orbital mass in both orbits. The authors stress the importance of including amyloidosis in the differential diagnosis of calcified orbital lesions, particularly when bilateral and associated with slow disease progression.
REFERENCES
1. Taban M, Piva A, See RF, Sadun AA, Quiros PA. Review: orbital amyloidosis. Ophthal Plast Reconstr Surg. 2004;20(2):162-5.
2. Leibovitch I, Selva D, Goldberg RA, Sullivan TJ, Saeed P, Davis G, et al. Periocular and orbital amyloidosis: clinical characteristics, management, and outcome. Ophthalmology. 2006;113(9):1657-64.
3. Cheng JY, Fong KS, Cheah ES, Choo CT. Lacrimal gland amyloidosis. Ophthal Plast Reconstr Surg. 2006;22(4):306-8.
4. Oishi A, Miyamoto K, Yoshimura N. Orbital amyloidosis-induced compressive optic neuropathy accompanied by characteristic eyelid pigmentation. Ophthal Plast Reconstr Surg. 2006;22(6):485-7.
5. Holmstrom GE, Nyman KG. Primary orbital amyloidosis localised to an extraocular muscle. Br J Ophthalmol. 1987;71(1):32-3.
6. Murdoch IE, Sullivan TJ, Moseley I, Hawkins PN, Pepys MB, Tan SY, et al. Primary localised amyloidosis of the orbit. Br J Ophthalmol. 1996;80(12):1083-6.
7. Gean-Marton AD, Kirsch CF, Vezina LG, Weber AL. Focal amyloidosis of the head and neck: evaluation with CT and MR imaging. Radiology. 1991;181(2):521-5.
8. Froula PD, Bartley GB, Garrity JA, Forbes G. The differential diagnosis of orbital calcification as detected on computed tomographic scans. Mayo Clin Proc. 1993;68(3):256-61.
9. Angotti-Neto H, Cunha LP, Oliveira AV, Monteiro ML. Mesenchymal chondrosarcoma of the orbit. Ophthal Plast Reconstr Surg. 2006;22(5):378-82.
 Correspondence address:
Correspondence address:
Mário L. R. Monteiro
Av. Angélica, 1.757 - Conj 61
São Paulo -SP 01227-200 - Brazil
E-mail: [email protected]
Submitted for publication: July 6, 2010
Accepted for publication: February 7, 2011
Study carried out at the Orbital Service, Division of Ophthalmology, University of São Paulo Medical School - São Paulo (SP), Brazil
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: A.C.P.Gonçalves, None; R.B.C.Moritz, None; M.L.R.Monteiro, None.
© 2024 - All rights reserved - Conselho Brasileiro de Oftalmologia
![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Scielo
Scielo
 Pocket
Pocket

{kind=link}
{kind=link}