

Nora Lucía Oliva Castillo; Nancy Carolina Quezada del Cid; Martin Arturo Zimmermann Paiz; Ana Marissa Ordóñez Rivas; Verónica Yaneth Burgos Elías; Evelyn del Busto Wilhelm
DOI: 10.5935/0004-2749.202100117
Dear editor,
Amblyopia is the most common cause of monocular visual loss in children and young adults in developed countries, and its prevalence ranges between 0.5% and 6% in the general population(1).
Several reports have confirmed that amblyopia may have an effect on various components of the visual pathway, such as organic and functional changes in the geniculate nucleus and visual cortex(2-3). Moreover, the examination of optic nerve head (ONH) parameters in amblyopic eyes has revealed significant changes in some of these parameters compared to those in normal eyes(4).
There is limited information regarding the anatomic changes that occur in amblyopic eyes before and after occlusion treatment. Kavitha et al.(5) reported no significant differences in retinal nerve fiber layer (RNFL) thickness after treatment in amblyopic eyes.
Considering the lack of conclusive data regarding the anatomic changes occurring in the visual pathway due to amblyopia or its treatment, we compared peripapillary RNFL (RNFLp) thickness and ONH anatomic features in amblyopic versus sound eyes and in amblyopic eyes before and after occlusion therapy using spectral-domain optical coherence tomography (SD-OCT) findings as an attempt to provide further information.
We included 15 patients with unilateral amblyopia with a median age of 7.3 ± 1.9 years, of whom 9 were men. In the anisometropia group (n=9), 3 patients had hyperopia, 8 patients had astigmatism, and 1 patient had hyperopia and astigmatism. In the strabismic amblyopia group (n=3), all patients had horizontal and unilateral strabismus. Regarding amblyopia severity, 1 patient had mild amblyopia and was anisometropic, 9 patients had moderate amblyopia, and 5 patients had severe amblyopia. The mean basal visual acuity values were 0.7 ± 0.3 logMAR (Logarithm of the Minimum Angle of Resolution) in amblyopic eyes and 0.15 ± 0.12 logMAR in fellow eyes (p<0.05).
The clinical features of the patients are summarized in table 1.
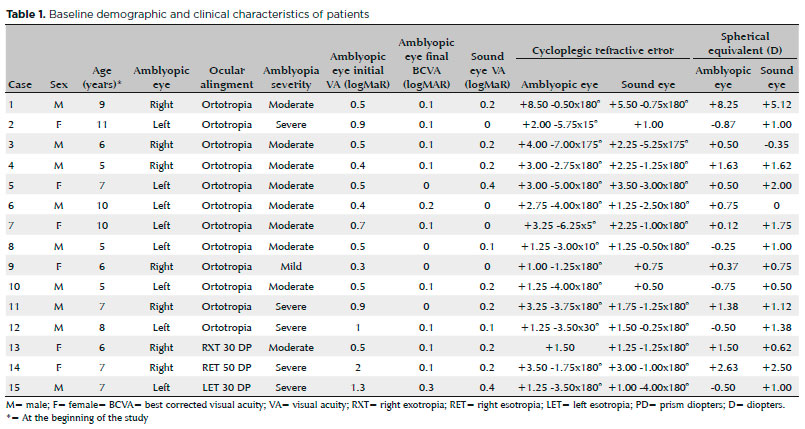
The average treatment period was 6.1 ± 4.9 months (5.5 ± 4.0 months for anisometropia and 9.0 ± 6.5 months for strabismic amblyopia, p=0.5; 5.4 ± 4.4 months for moderate amblyopia and 7.6 ± 5.7 months for severe amblyopia, p=0.5). The final visual acuity values were 0.1 ± 0.1 logMAR for patients with anisometropia and 0.2 ± 0.1 logMAR for those with strabismic amblyopia (p=0.3) and 0.1 ± 0.05 logMAR for patients with moderate amblyopia and 0.12 ± 0.1 logMAR for those with severe amblyopia (p=0.5). Patients showed improvement of an average of 4.1 ± 2.2 lines of vision; those with anisometropia showed improvement of 3.5 ± 1.4 lines, and those with strabismic amblyopia showed improvement of 6.7 ± 2.9 lines (p=0.2). Patients with moderate amblyopia showed improvement of 3.6 ± 1.5 lines of vision, and those with severe amblyopia showed improvement of 5.7 ± 3.0 lines (p=0.3).
The time taken for amblyopia resolution was 5.3 ± 4.1 months for patients with anisometropia and 9 ± 6.5 months for those with strabismic amblyopia (p=0.5). Based on the severity of amblyopia, the time taken to achieve resolution was 5.4 ± 4.4 months in patients with moderate amblyopia and 7.6 ± 5.7 months in those with severe amblyopia (p=0.5). Patient with mild amblyopia achieved resolution in 4 months.
Table 2 summarizes the comparative results of RNFLp thickness and ONH anatomic features between amblyopic and fellow eyes both before and after treatment and in amblyopic eyes. A significant difference was found only in the inferior quadrant of RNFLp thickness, which was lesser in amblyopic eyes than in fellow eyes after treatment (150.5 ± 20.9 and 159.3 ± 17.1 µm, p=0.03).
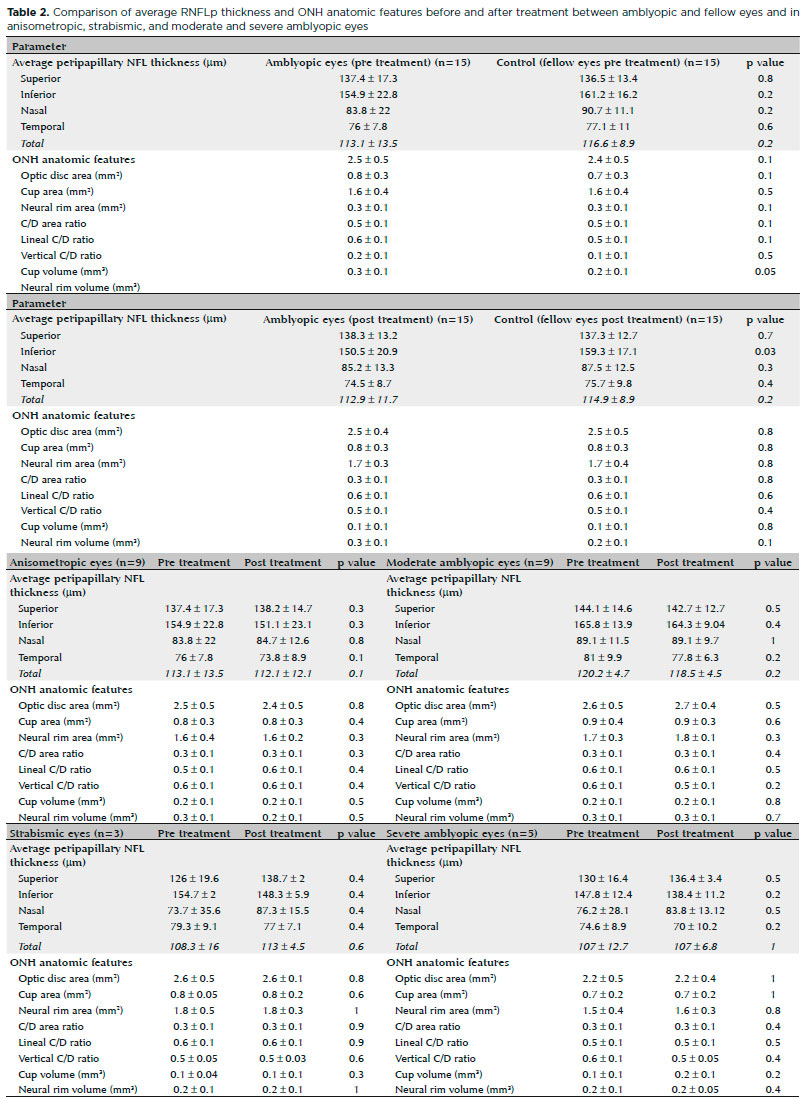
Age, sex, and spherical equivalent were identified as factors that could modify RNFLp thickness and ONH anatomic features in sound and amblyopic eyes, although they showed no significant associations (p>0.05).
Our study showed no significant difference in RNFLp thickness nor in ONH anatomic features in amblyopic eyes after amblyopia treatment and between amblyopic and fellow eyes.
Further studies are required to determine whether anatomic and structural ocular alterations occur after occlusion treatment in patients with amblyopia.
REFERENCES
1. Campos E. Amblyopia. Surv Ophthalmol. 1995;40(1):23-39.
2. Von Noorden G, Crawford M. The lateral geniculate nucleus in human strabismic amblyopia. Invest Ophthalmol Vis Sci. 1992; 33(9):2729-32.
3. Von Noorden G, Crawford M. The lateral geniculate nucleus in human anisometropic amblyopia. Invest Ophthalmol Vis Sci. 1983;24(6):788-90.
4. Araki S, Miki A, Yamashita T, Goto K, Haruishi K, Ieki Y, et. al. A comparison between amblyopic and fellow eyes in unilateral amblyopia using spectral-domain optical coherence tomography. Clin Ophthalmol. 2014;8:2199-207.
5. Kavitha V, Heralgi M, Harishkumar P, Harogoppa S, Shivaswamy H, Geetha H. Analysis of macular, foveal and retinal nerve fiber layer thickness in children with unilateral anisometropic amblyopia and their changes following occlusion therapy. Indian J Ophthalmol. 2019;67(7):1016-22. Comment in: Indian J Ophthalmol. 2019;67(7):1023-4.
Submitted for publication:
June 1, 2021.
Accepted for publication:
June 20, 2021.
Funding: This study received no specific financial support
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose
© 2024 - All rights reserved - Conselho Brasileiro de Oftalmologia
![]()
 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
